Patients
The present study was approved by the human research committee of the institutional review board of our hospital and complied with the guidelines of the Health Insurance Portability and Accountability Act of 1996 and the Declaration of Helsinki. The requirement for informed consent was waived due to the retrospective nature of the study. Two-hundred and eighty-two patients with histopathologically proven thyroid cancer (ATC, PDTC, or PTC) were identified from the electronic medical record database of our hospital between December 2006 and June 2023. Among them, 203 patients who did not undergo neck MRI (7 ATCs, 5 PDTCs, and 191 PTCs) were excluded. In total, 79 patients (14 ATCs, 8 PDTCs, and 57 PTCs) were enrolled in this study.
Imaging technique
MRI was performed for all patients using 1.5 Tesla MRI scanners (Intera Achieva 1.5 T Pulsar, Philips Healthcare, Best, the Netherlands, or Ingenia Prodiva 1.5 T CS, Philips Healthcare, Best, the Netherlands) or a 3.0 Tesla MRI scanner (Intera Achieva 3.0 T Quasar Dual, Philips Healthcare, Best, the Netherlands). All images were obtained at a section thickness of 3–4 mm with an intersection gap of 1 mm. Axial non-fat-suppressed T2-weighted images (T2WIs) and axial non-fat-suppressed T1-weighted images (T1WIs) were obtained from all patients. Axial short-tau inversion recovery single-shot spin-echo echo-planar diffusion-weighted images (DWIs) with b values of 0 and 1000 s/mm were obtained from 68 patients (11 ATCs, 7 PDTCs, and 50 PTCs). Axial fat-suppressed contrast-enhanced T1-weighted images (FS CE-T1WIs) were obtained from 46 patients (8 ATCs, 5 PDTCs, and 33 PTCs) after the intravenous injection of 0.1 mmol/kg of gadopentetate dimeglumine (Magnevist; Bayer HealthCare, Leverkusen, Germany) or gadobutrol (Gadavist; Bayer HealthCare).
CT imaging was performed for all patients using an 8-slice CT scanner (LightSpeed Ultra; GE Healthcare, Milwaukee, WI, USA), or 16-slice CT scanner (LightSpeed 16; GE Healthcare, Milwaukee, WI, USA), or 64-slice CT scanner (Brilliance 64; Philips, Best, the Netherlands or Discovery CT750 HD; GE Healthcare, Milwaukee, WI, USA), or 256-slice CT scanner (Revolution CT Apex Edition; GE Healthcare, Milwaukee, WI, USA). Unenhanced CT images were obtained from all patients. All transverse CT images were reconstructed with 2.5-mm section thickness and no overlap.
Imaging assessment
Two radiologists (radiologists-1 and -2) with post-training experience in head-and-neck imaging of 24 and 10 years, respectively, reviewed all MRI images individually and randomly. The reviewers were unaware of any clinical information or pathological diagnosis. Any disagreement between the two reviewers was resolved through discussion until a consensus was reached.
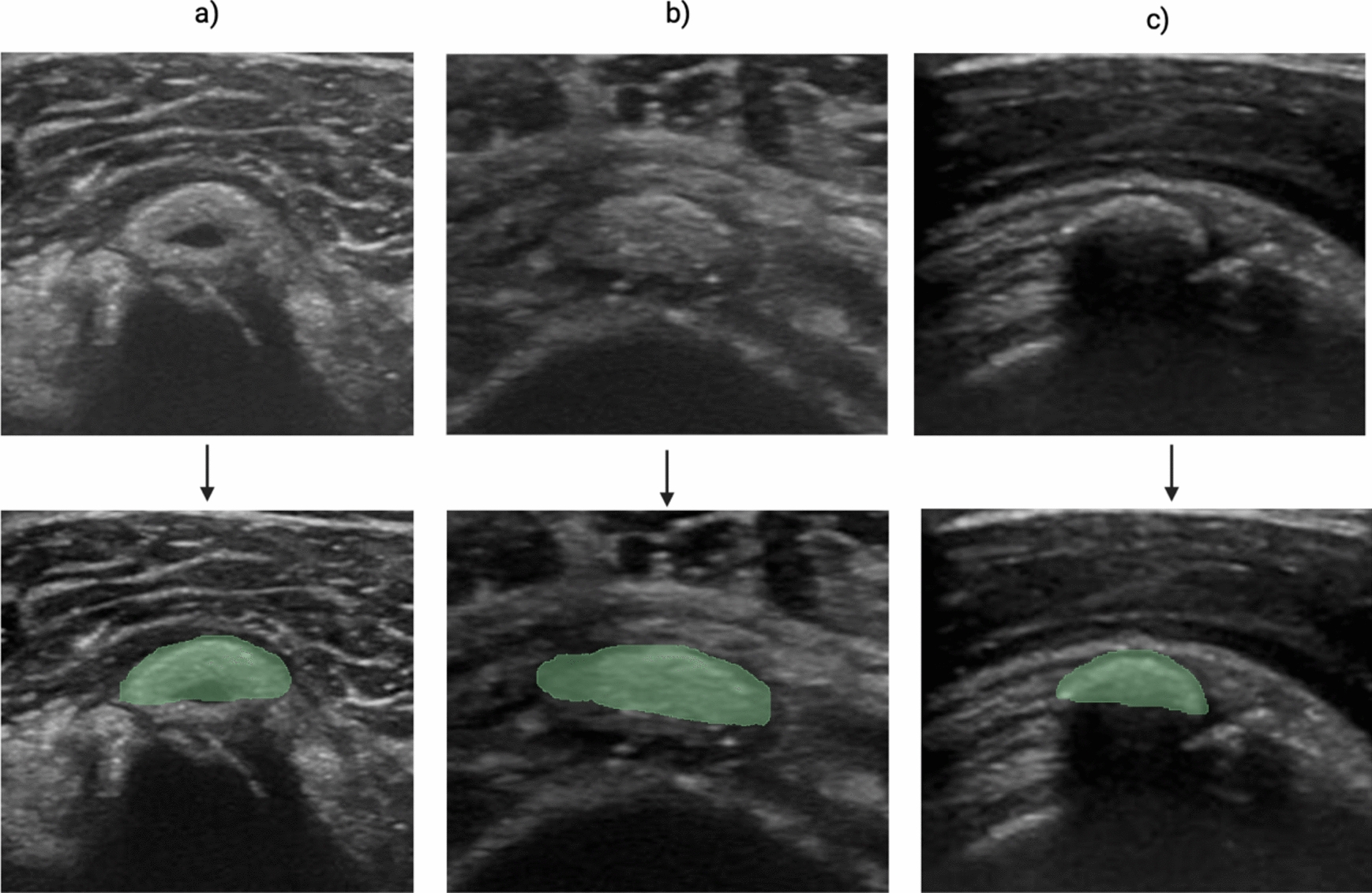
For quantitative assessments, radiologist-1 measured the maximum tumor diameter of the whole lesion and the signal intensity (SI) of the solid components of the tumors. The SI of the solid components on T1WI, T2WI, and FS CE-T1WI was measured by using regions of interest (ROIs), which were carefully placed on the solid components as widely as possible in the slice showing the maximum diameter by referring to T2WI and/or FS CE-T1WI. The reviewers measured the SI of the spinal cord at the same level as the lesion by placing 10-mm diameter circle ROIs and calculating the tumor-to-spinal cord signal intensity ratio (SIR). The mean apparent diffusion coefficient (ADC) values of the solid components of the tumor were also measured on ADC maps by placing ROIs. When ring-shaped hypointensity was found within the tumor on T2WI, the reviewers measured the diameter and maximum thickness of the area.
For qualitative assessments, radiologists-1 and -2 evaluated tumor laterality (unilateral or bilateral) and the tumor margin (well-defined or ill-defined). On T2WI and T1WI, they qualitatively evaluated internal uniformity (homogeneous or heterogeneous) and the predominant SI of the solid components relative to the spinal cord (hyperintensity, isointensity, or hypointensity). The presence of hypointensity similar to the muscle on T2WI, intratumoral ring-shaped hypointensity on T2WI, and hyperintensity relative to the muscle on T1WI were also assessed. Furthermore, on FS CE-T1WI, both radiologists assessed internal uniformity (homogeneous or heterogeneous) and the presence of an unenhanced area. In addition, the presence of extrathyroidal extension, tracheal invasion, esophageal invasion, laryngeal invasion, vascular invasion, venous thrombosis, venous tumor thrombosis, and lymphadenopathy was assessed. Extrathyroidal extension included focal outer protrusion, irregular outer protrusion, surrounding fat stranding, or adjacent organ invasion. Tracheal, esophageal, laryngeal, and vascular invasions were defined as tracheal intraluminal invasion, esophageal intramuscular invasion, laryngeal soft-tissue or cartilage invasion, and solid soft-tissue contact > 180° between the tumor and vessel circumference, respectively. Lymphadenopathy was considered positive when the minimum diameter exceeded 10 mm or an intranodal cystic area was found.
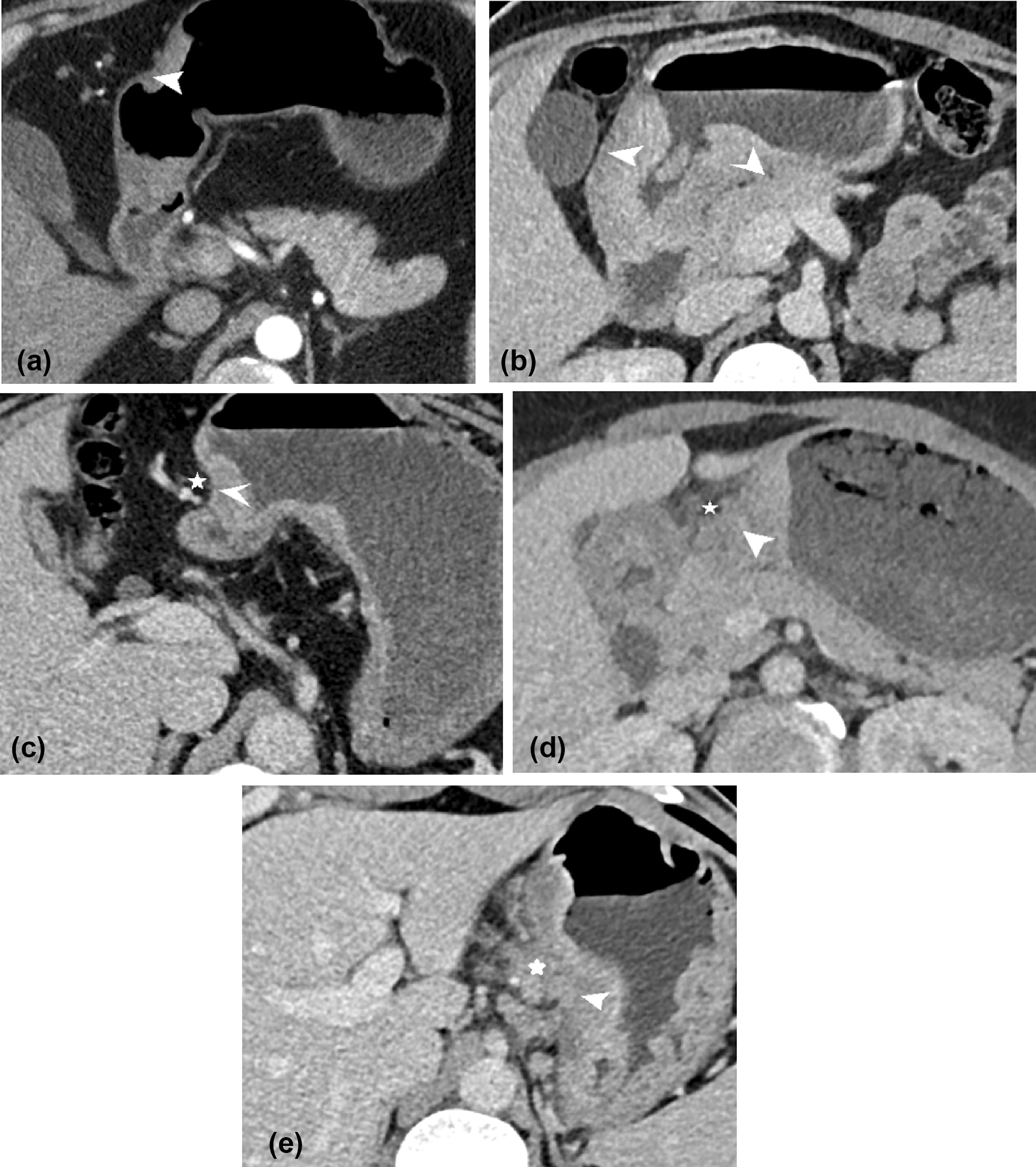
In addition, the presence of calcification within the tumor was assessed on CT images. CT attenuations of calcification were defined as > 200 HU. If calcification was observed within the tumor, the number (single or multiple) and shape (nodular- and/or ring-shaped) of calcification were determined. In the cases with ring-shaped hypointensity on T2WI, the presence of ring-shaped calcification corresponding to ring-shaped hypointensity on T2WI was assessed.
Statistical analysis
All statistical analyses were performed using the Statistical Package for the Social Sciences version 24.0 (IBM Corp.) or EZR (Saitama Medical Center, Jichi Medical University). Tukey’s post hoc test or Welch’s ANOVA with Games–Howell post hoc test was used to compare quantitative measurements (age, maximum diameter, SIR, ADC value, and diameter and maximum thickness of ring-shaped hypointensity on T2WI) between the three pathologies. Fisher’s exact test was performed to compare qualitative assessment parameters (gender, internal uniformity, predominant SI, heterogeneity, hypointensity on T2WI, ring-shaped hypointensity on T2WI, hyperintensity on T1WI, tumor laterality, unenhanced area, tumor margin, extrathyroidal extension, tracheal invasion, esophageal invasion, laryngeal invasion, vascular invasion, venous thrombosis, venous tumor thrombosis, lymphadenopathy, calcification, number and shape of calcification, and ring-shaped calcification corresponding to ring-shaped hypointensity on T2WI) between the three pathologies. When a two-sided p value < 0.05 of the test for the three groups was observed, we concluded that there was a difference in the frequency between the groups. Post hoc pairwise comparisons were performed only if the Fisher’s exact test for the three groups was statistically significant. p values were corrected according to the Bonferroni method for pairwise comparisons. Interobserver variability in qualitative assessments was evaluated using Kappa statistic. A Kappa value of ≤ 0.20 was interpreted as slight agreement, 0.21–0.40 as fair agreement, 0.41–0.60 as moderate agreement, 0.61–0.80 as substantial agreement, and ≥ 0.81 as almost perfect agreement.






留言 (0)