
記住我








After approval by the Ethics Committee of Dışkapı Yıldırım Beyazıt Training and Research Hospital (Ethics Committee 20.01.2020 No. 80/07), this prospective, randomized, controlled, single-blind study was planned and registered with ClinicalTrials.gov (registration number NCT04277559). Written and verbal informed consent was obtained from all patients in accordance with the Declaration of Helsinki. The Consolidated Standards of Reporting Trials (CONSORT) flow chart was used for patient enrollment and allocation. The study was conducted between November 2021 and July 2022 in the operating room of the general surgery clinic of Dışkapı Yıldırım Beyazıt Training and Research Hospital.
Patients between 18 and 70 years of age, American Society of Anesthesia (ASA) physical status I–II, who could speak and understand Turkish language clearly, who could read and write, and who were scheduled to undergo elective inguinal hernia surgery under general anesthesia were planned to be included in the study. Patients with severe hearing impairment, visual impairment, history of narcotic use, alcohol dependence, dementia, regular use of antidepressants, and no specific music preferences were excluded.
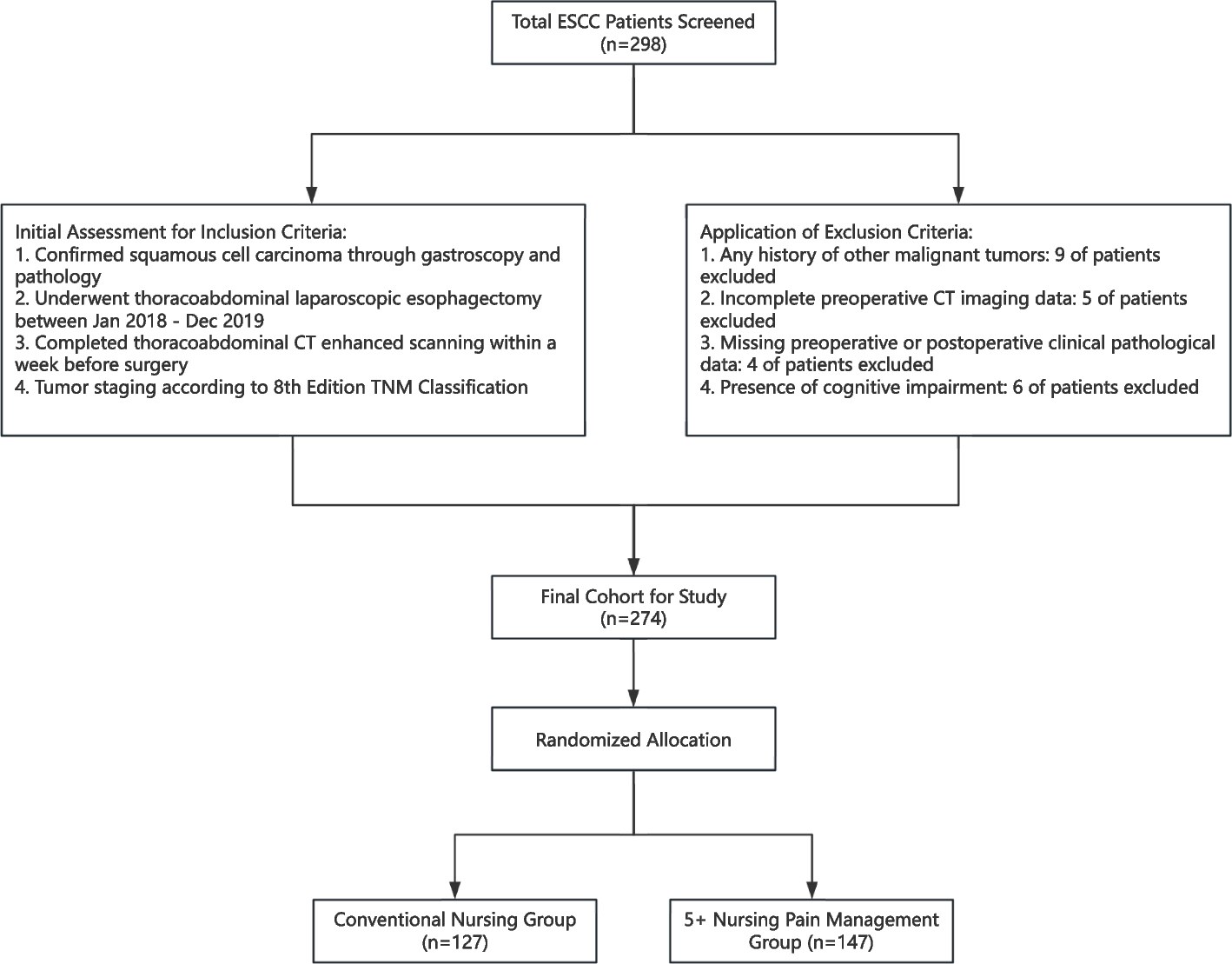
A total of 255 patients were included in the study. Of these, 30 patients were excluded because they did not meet the inclusion criteria. The 225 patients enrolled in the study were randomized into 3 groups by a computerized randomization method patient-preferred music group (group P), classical music group (group C), or no music group (group N) (Fig. 1).
Fig. 1 Preoperative management and intervention
Preoperative management and interventionDemographic data such as age, sex, height, weight, previous elective and/or emergency surgery, educational status, and marital status of the patients were recorded during the preoperative evaluation period. Patients were given the STAI-1 and STAI-2 questionnaires to self-report their current state of anxiety and the QoR-40 (40–200 points) questionnaire in their beds 1 h before surgery.
Patients were brought to the waiting room where preoperative measurements were taken. Patients were asked for their favorite music title and singer, without limiting the type of music, and were enrolled in group P. Patients in the preferred music group listened to their favorite music for 15 min. Patients in the classical music group also listened to Vivaldi’s Four Seasons for 15 min, which has been shown to be effective in similar anxiety studies (Firmeza et al. 2017; Mammarella et al. 2007). These two groups of patients used headphones that completely covered their ears to further isolate them from environmental stimuli. The volume of the music was adjusted to remain between 50 and 60 dB (Kavak Akelma et al. 2022). During the same period, patients in the control group did not listen to music or use headphones.
In groups P and C, heart rate and systolic-diastolic blood pressure were measured before and after listening to music. In the control group, heart rate, systolic-diastolic, and mean blood pressure were measured and recorded upon entering the preoperative waiting room and 15 min later. None of the patients were given premedication prior to the procedure. After this procedure, the patients were taken to the operating room.
Intraoperative managementHR, SBP, DBP, MAP, peripheral oxygen saturation, and bispectral index (BIS Quatro sensor and BIS VISTA monitor) were monitored and recorded noninvasively in the operating room. After induction of anesthesia with fentanyl citrate (1–2 μg/kg) and propofol (2–4 mg/kg), a laryngeal mask airway was inserted. Anesthesia was maintained with sevoflurane (1–1.5% end-tidal concentration) in a 50% air/50% oxygen mixture. The sevoflurane concentration was titrated to a BIS value of 40 to 60. Hypotension was defined as a decrease in MAP of at least 20% from baseline and was treated with intravenous ephedrine 5 mg. Bradycardia was defined as a heart rate of less than 45 beats per minute and was treated with intravenous atropine 0.5 mg. Surgery was performed by an experienced surgeon. All patients underwent open anterior mesh repair. After induction of anesthesia, an erector spinae plane block with 20 mL of 0.25% bupivacaine was performed unilaterally at the T7 level on the hernia side. For analgesia, 1000 mg intravenous acetaminophen and 100 mg intravenous tramadol were administered to all patients approximately 15 min before the end of surgery as part of multimodal analgesia management. In the postoperative period, 50 mg dexketoprofen-trometamol was administered intravenously every 8 h. 50 mg intravenous tramadol was administered as rescue analgesia when the NRS was 4 or higher.
OutcomesThe State-Trait Anxiety Inventory (STAI-1 and STAI-2) was determined as the primary outcome of our study. STAI-1 and STAI-2 questionnaires were administered to all patients in their rooms 1 h before surgery, and the STAI-1 questionnaire was repeated 4–6 h after surgery (Fig. 2). The State-Trait Anxiety Inventory (STAI), developed by Spielberger et al. in 1970 (Spielberger et al. 1983) and adapted to Turkish by Öner and Le Compte in 1983 (1983), is a 4-point Likert self-report scale consisting of a total of 40 items, 20 of which are assigned to the state anxiety subscale (STAI-1) and 20 to the trait anxiety subscale (STAI-2). Scores ranged from 20 to 80, with higher scores indicating higher levels of anxiety.
Fig. 2
One of the secondary outcomes of our study was the 24-h Quality of Recovery-40 Questionnaire (QoR-40) (Fig. 2). The QoR-40 was defined to assess the quality of recovery of patients in the early postoperative period from the patient’s perspective. The questionnaire includes five parameters: physical comfort (n = 12), patient support (n = 7), physical independence (n = 5), pain (n = 7), and emotional state (n = 9). The questionnaire consists of a total of 40 questions, and each question is scored on a 5-point Likert scale. These scores are summed to give a total score. The worst collection scores 40 points and the best collection scores 200 points (Myles et al. 2023; Myles et al. 2022). The QoR-40 has been used and validated in people from many different countries with cultural and physical differences (Karaman et al. 2023). Hemodynamic variables recorded before and after the musical performance were evaluated in the study groups and before entering and leaving the waiting room in the control group.
The NRS (numerical rating scale) was used to assess patient pain (0 = no pain; 10= worst pain imaginable). Postoperative NRS scores were recorded at 1, 4, 12, and 24 h (Fig. 2). The Likert scale was used to assess patient satisfaction. The Likert scale consisted of a questionnaire asking for numerical values between 1 and 7. All of these scales were administered by a blinded investigator.
Statistical analysisWe performed a priori sample size calculation, based on pilot data obtained from postoperative STAI-1 scores, using the G*Power version 3.1.9.2 (© Franz Faul, Edgar Erdfelder, Albert-Georg Lang, and Axel Buchner, 2006, 2009) (Faul et al. 2007; Erdfelder and FAul F, Buchner A, Lang AG. 2023). In the pilot study we conducted with 10 patients from each of the 3 groups, the postoperative STAI score was recorded. A sample size of 65 patients in each group was calculated with a power of 95% and an α-level of 0.05 error, 0.285 effect size. To account for a potential 15% attrition rate, a sample of 75 participants per group was required for this study.
Data analysis was conducted using IBM SPSS 25.0 (Armonk, NY: IBM Corp.) and MedCalc 15.8 (MedCalc Software bvba, Ostend, Belgium) statistical package programs. The normality of the distribution of continuous variables was evaluated using the one-sample Shapiro-Wilk test. Patient demographics and characteristics were expressed as number and percentage, median (interquartile range, IQR), and mean (standard deviation, SD), and were analyzed using the chi-square test for categorical variables and the independent t-test for normally distributed continuous variables. Mann–Whitney U test and Kruskal-Wallis were applied for comparisons of non-parametric and non-normally distributed data. Nominal data were analyzed by Pearson chi-square or Fisher’s exact test where appropriate. The corrected Bonferroni test was used for multiple comparisons. p values < 0.05 were considered statistically significant in each test.
留言 (0)