MOT are extremely rare intraoral entities that arise either de novo from elements of the tooth-forming apparatus or as a malignant transformation of a pre-existing oral lesion such as a benign OT or cyst [6]. In the latest updates of the Head and Neck WHO classification, our understanding of the evolution of MOT is expanded [5].
According to the current literature, the frequency of development of malignancy in recurrent benign OT has not been well studied. Therefore, we aimed to investigate the prevalence of MOT and to report the relative rate of malignant transformation in recurrent benign OT.
Generally, OT comprised a quite small fraction of intra-oral lesions. In this study, we found that OT accounted for only 6.4% of the cases in which oral biopsies had been performed. The majority of OT was benign accounting for 94.1% of the studied cases. The frequency of MOT accounted for only 5.8% which is consistent with the studies conducted in Brazil (5.5%) [7], Turkey (5.5%) [8], China (6.1%) [9], as well as the United Kingdom (5.7%) [10]. However, a lower fraction was stated in studies conducted in Malaysia (1.2%) [11]. On the other hand, a higher frequency was observed to be nearly 8.9% of all oral tumors in Africa and Asia [12, 13].
In our study, we found that benign tumors were the most frequent among all cases of OT (benign 94.1%, malignant 5.9%). MOT are rare, and only 21 (5.9%) patients with such tumors were recognized in this study similar to a previously performed study [14]. The most common MOT was detected in this study to be PIOC NOS, which was in agreement with the previously reported studies [1, 10], followed by AC, CCOC, and GCOC. Our noted finding was unlike most of the earlier performed studies that showed AC was the most frequently reported MOT. In addition our finding was consistent with the case series described in 2010 by Gupta and Ponniah [15].
The least common histological diagnosis was documented to be AFS, a subtype of odontogenic sarcoma, as defined in the most recent WHO classification [5]. Over the last 10 years, a single case of odontogenic sarcomas was observed but without any reported case of odontogenic carcinosarcomas, emphasizing the relative scarcity of this type of OT compared to carcinomas of odontogenic origin [5]. The reason for the absence of carcinosarcoma in this current study and many others can be attributed to being an unrecognized entity until the updated classification of WHO of head and neck tumors in 2017 [16].
The observed differences in the distribution of MOT might be due to the geographical and cultural variation among different study populations. Among the MOT, the incidence of odontogenic carcinoma is much higher than sarcomas accounting for 95.2% of cases which is in accordance with other studies [16]. Generally, the current study documented a recent increase in the frequency of MOT in Egypt. Our reported finding may be due to socioeconomic and cultural standards that obscure both the incidence and reporting of tumor types. Decreased reporting and delayed medical attention, of course, would affect the rate of recurrence and the ability to report neoplastic malignant transformation in such cases.
Although MOT may be found in any age group, their highest incidence was reported in patients in at least the fifth decade with more than 75% of cases occurring in those aged ≥ 40 years [2, 16, 17]. In this study, the overall male-to-female ratio among patients with MOTs was approximately 1.5:1. The male predominance detected in this study agrees with other published studies [18, 19]. Conversely, few studies have stated equal proportions of patients of both genders [20].
Across all the MOT, 85.7% (n = 18) were de novo while only 14.3% (n = 3) developed recurrence. Our study showed a marked maxillary involvement of recurrent MOT. All these tumors occurred as intra-osseous jaw lesions. The average patient age of recurrent MOT was 38.4 years with a slight male predilection (66.6%).
Among the recurrent MOT, two cases were diagnosed as GCOC. GCOC is a rare MOT and is considered to arise either de novo or from a calcifying odontogenic cyst (COC) or (DGCT) [21]. The first case in our study was GCOC which recurred from DGCT after its malignant transformation. Such a finding was documented previously from studies that highlighted that the development of GCOC from DGCT might take several years [22, 23].
The second case was developed from a previously diagnosed hybrid odontogenic tumor formed of AB and AOT. Hybrid odontogenic tumor types have been first documented by Yamazaki et al. in 2014, who stated that their occurrences are rare [24]. To the best of our knowledge, this is the second documentation of GCOC arising in a previously diagnosed hybrid tumor of AB and AOT [25].
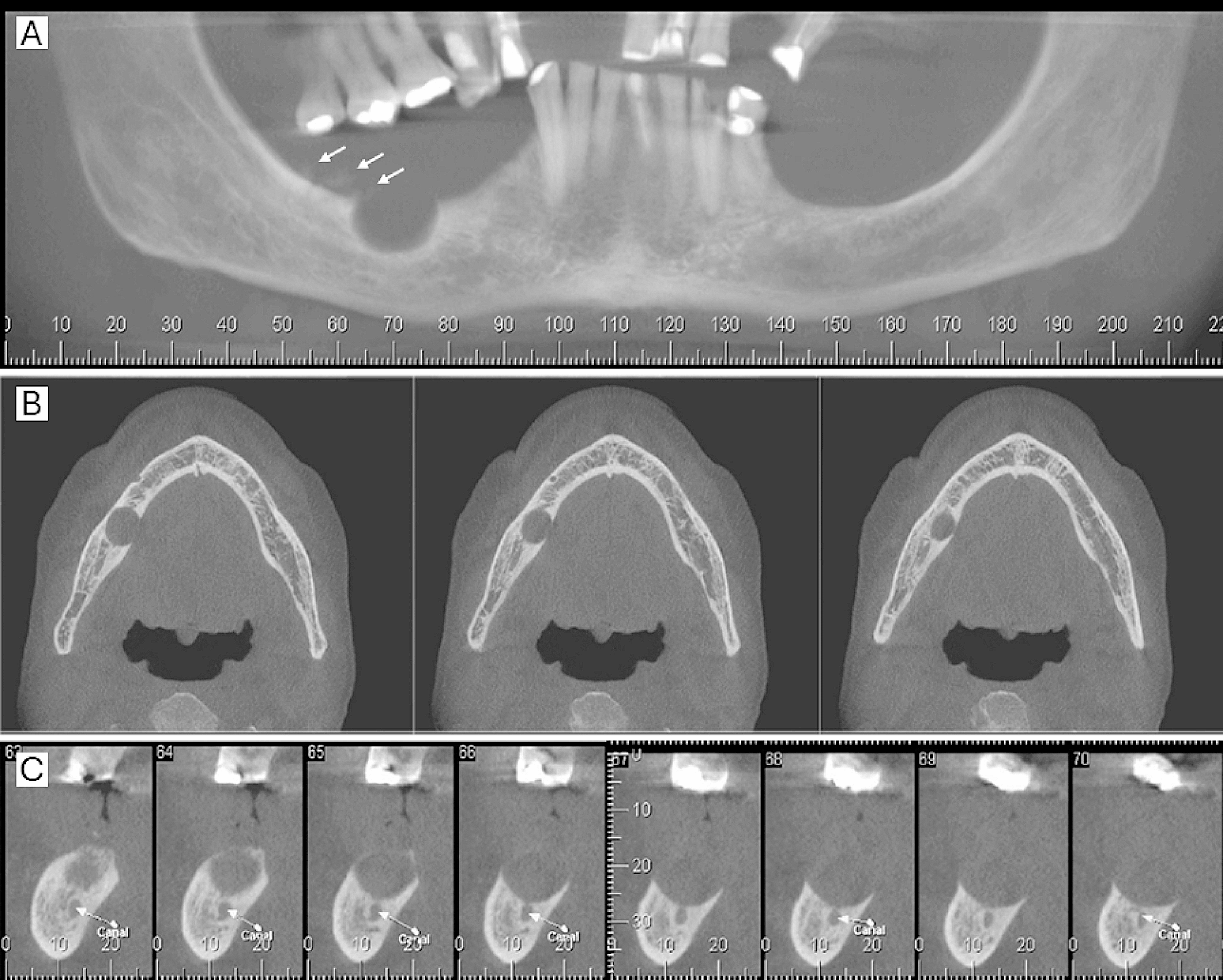
GCOC was twice as often reported in the maxilla with a predilection to males in their fourth decade. Patients typically present with signs of a rapid painful swelling and mucosal ulcer which is in accordance with our study [26,27,28]. Findings related to radiographic examination were confirmed to be a powerful tool during the malignant transformation of such cases. Those cases were more likely to present as expansile lesions with ill-defined margins, causing destruction and perforation of the cortex of jaw bones similar to our documented cases [28 & 29].
We reported only one recurrent case of PIOC NOS from a long-standing undiagnosed well-defined cystic lesion in the anterior maxillary tooth-bearing area. PIOC NOS of the jaw is a rare neoplasm that can arise either from the lining epithelium of long-lasting odontogenic cysts or de novo from odontogenic epithelial rests [29, 30]. The commonly associated cysts with PIOC NOS are odontogenic keratocysts, residual, and dentigerous cysts [31,32,33]. Unfortunately, in our study, the initial occurrence of the lesion in our case was undiagnosed.
The peak incidence of PIOC NOS is in the sixth decade of life; however, it has a wide age range from 14 to 80 years [5]. A male predilection with a ratio (2:1) has been witnessed by many authors similar to our study [5, 33]. The lower jaw was more clinically affected (especially the posterior region) than the upper jaw [32, 33]. In the current study, the incidence in an unusual location in the anterior maxilla extending from the left canine area to the right first premolar area crossing the midline was detected. Many authors accredited that the chronic inflammatory process is the main prompting factor for PIOC NOS development [34, 35]. This may explain the presence of a purulent aspirate and necrosis caused by tumorigenesis.
Radiographic imaging showed an ill-defined radiolucent lesion with cortical bone thinning and perforation simulating another previous case series [34, 35]. Clinically, the early stage of PIOC NOS might frequently be asymptomatic or might cause mild dental disorders. Therefore, lymph node metastasis may already be present during the biopsy, which was an obvious finding in our case [36]. In the end, one limitation of this study is that the included cases are from one institute; this was attributed to the lack of a standard patient filing system in many governmental hospitals in addition to the lack of patient awareness of the importance of follow-up visits.









留言 (0)