
記住我




Six mice were treated in each of the ten conditions. Rapid tumor growth was observed in the control mice, and all control mice were sacrificed on Day 19 from start of drug intervention. As single agents, plocabulin and gemcitabine exhibited a similar degree of tumor growth control. The mice that received both drugs clearly had the best outcome, with some mice showing complete tumor regressions (CI < 0.1). All mice were sacrificed and euthanized when the tumor volume reached 2,000 mm3 or at the end of the experiment at 4 weeks (Supplementary Fig. 1, data shown for 4 conditions).
Patient characteristicsThe study enrolled 57 patients (Table 1); 42 (73.7%) were females; 26 (45.6%) were white and median age was 62 years (range, 25–80 years). Most patients had ECOG PS score of 1 (n = 42, 73.7%). The most common primary tumor type was non-small cell lung cancer (NSCLC, n = 18, 31.6%), and EOC (n = 13, 22.8%). All patients had received prior systemic anticancer therapy, with a median of 3 prior lines (range, 1–7 lines) and 4 agents (range, 2–9 agents). Seventeen patients (29.8%) received ≥ 4 lines of prior anticancer therapies each. Non-medical therapy included surgery (n = 38, 66.7%) and radiotherapy (n = 36, 63.2%).
Table 1 Baseline characteristics of patients (n = 57)Safety, DLTs, MTD, and RDOf the 57 enrolled patients, 55 patients received at least one dose of study drug. Patients received a median of 3 cycles (range, 1–16 cycles) of therapy. Most patients (n = 32, 58.2%) at all DLs discontinued treatment due to disease progression. Ten patients (18.2%) refused further treatment with the combination. Five patients (9.1%) discontinued due to treatment-related AEs [PSN (G1-1; G2-2; G3-1)]; and grade 3 pneumonitis (n = 1)]. Four patients (7.3%) discontinued following a decision by the investigator in the absence of radiologically documented disease progression. Three patients (5.5%) died while on treatment due to disease-related AEs. Finally, one patient (1.8%) discontinued due to a non-treatment-related AE.
All 55 treated patients were evaluated for safety. Most treatment emergent AEs (or with unknown relationship) at all DLs were grade 1 or 2 (Table 2). The most common were fatigue (56.4% of patients), nausea (54.5%), PSN (36.4%), musculoskeletal (32.7%), diarrhea (30.9%), decreased appetite (27.3%), vomiting (27.3%), abdominal pain (16.4%), and constipation (14.5%). Treatment-related grade ≥ 3 AEs comprised fatigue (3 patients), abdominal pain, nausea, vomiting (2 patients each), arthralgia, diarrhea, dyspnea, intestinal obstruction, muscular weakness, neurotoxicity, and pneumonitis (1 patient each). None of these AEs reached grade 4.
Table 2 Treatment emergent adverse events and laboratory abnormalitiesHematological abnormalities regardless of relationship were present at all DLs. Severe myelosuppression comprised grade 3 anemia (34.6%), grade 3/4 neutropenia (26.9%), and grade 3/4 thrombocytopenia (17.3% of patients). Hematological toxicity was the cause of most cycle delays and dose omission at all DLs, but did not result in treatment discontinuations.
Most biochemical abnormalities at all DLs were grade 1 or 2, regardless of relationship. Severe biochemical abnormalities were found in only one (1.9%) to three (5.8%) patients each and were mostly grade 3; the only one to reach grade 4 was bilirubin increase in one patient who had concomitant disease-related grade 3 ALT increase and disease progression in the liver. No biochemical abnormalities resulted in cycle delays, dose omissions or dose reductions.
At all DLs, dose delays were observed in 23 patients (54.8% of 42 patients who received at least 2 cycles each) in 54 cycles (30.3% of 178 cycles susceptible of delay). Dose omissions of either gemcitabine or plocabulin were carried out in 24 patients (47.1% of 51 patients susceptible of dose omission) and 53 cycles (23.2% of 228 cycles susceptible of dose omission). Gemcitabine dose reductions occurred in 8 patients (19.0% of 42 patients) and plocabulin dose reductions also in 8 patients (19.0% of 42 patients).
DLTs were observed at 4 DLs (Table 3): two grade 3 neurotoxicity’s categorized as grade 3 PSN in one patient at DL2 (n = 6, 16.7%) and grade 3 bowel obstruction [autonomic nervous system (ANS) dysregulation] in one patient at DL8 (n = 5, 20%), grade 4 thrombocytopenia in one patient at DL6 (n = 7, 14%) and grade 3 abdominal pain in one patient at DL7 (n = 13, 7.7%). Further dose escalation was stopped following the finding at DL8 of treatment-related Cycle 1 Day 8 dose omissions and reductions from Cycle 2 onwards in 3 and 2 patients, respectively.
Table 3 DLTs and dose escalationThe MTD for a combination of gemcitabine given i.v. over 30 min followed by plocabulin given i.v. over 10 min, both on Day 1 and Day 8 q3wk, in patients with advanced solid tumors was defined at DL8 (plocabulin 10.5 mg/m2 plus gemcitabine 1000 mg/m2). Patient accrual was discontinued before an RD had been formally determined because of the narrow therapeutic index, toxicity profile, and limited antitumor activity of the combination.
Eight patients (14.5%) died during this study. Five deaths (5/55; 9.1%) were due to disease progression, and 3 (3/55; 5.4%) deaths were due to disease-related AEs (grade 4 sepsis secondary to aspiration pneumonia, grade 5 respiratory arrest and grade 5 dyspnea). All 3 patients who died due to disease-related AEs had tumor lesions in the lungs at baseline.
PharmacokineticsMean maximum plasma concentration (Cmax), area under the concentration–time curve, and half-life for plocabulin at the DL immediately below the MTD (DL7: plocabulin 10.0 mg/m2 plus gemcitabine 1000 mg/m2) in Cycle 1 were 665 μg/L, 430 h*mg/L and 4 h, respectively (Supplementary Table 1a). PK parameters for gemcitabine or dFdU at all DLs were in line with reference values from the literature (Supplementary Table 1b) [20,21,22].
Efficacy outcomesForty-six patients treated at all DLs were evaluable for efficacy. Overall, 6 patients had a response- 1 Complete response (CR) and 5 partial responses (PR) (overall response rate [ORR] = 13%) and 12 patients had stable disease (SD) ≥ 4 months. Clinical benefit (ORR plus SD ≥ 4 months) was observed in 18 of 46 (39.1%) evaluable patients (Supplementary Table 2, Figs. 1–2). Clinical benefit was observed in NSCLC (n = 6; one CR, one PR, and 4 SD ≥ 4 months), gynecological tumors (n = 5; one PR and 4 SD ≥ 4 months), EOC (n = 4; 2 PRs and 2 SD ≥ 4 months), head and neck cancer (n = 2; one PR and one SD ≥ 4 months), and breast cancer (n = 1; one SD ≥ 4 months). In 13 patients with clinical benefit, the progression free survival (PFS) values achieved with the combination were longer than the time to progression (TTP) values achieved with the last prior therapy, including patients with gynecological tumors (n = 4), EOC (n = 4), NSCLC (n = 2), head and neck cancer (n = 2), and breast cancer (n = 1).
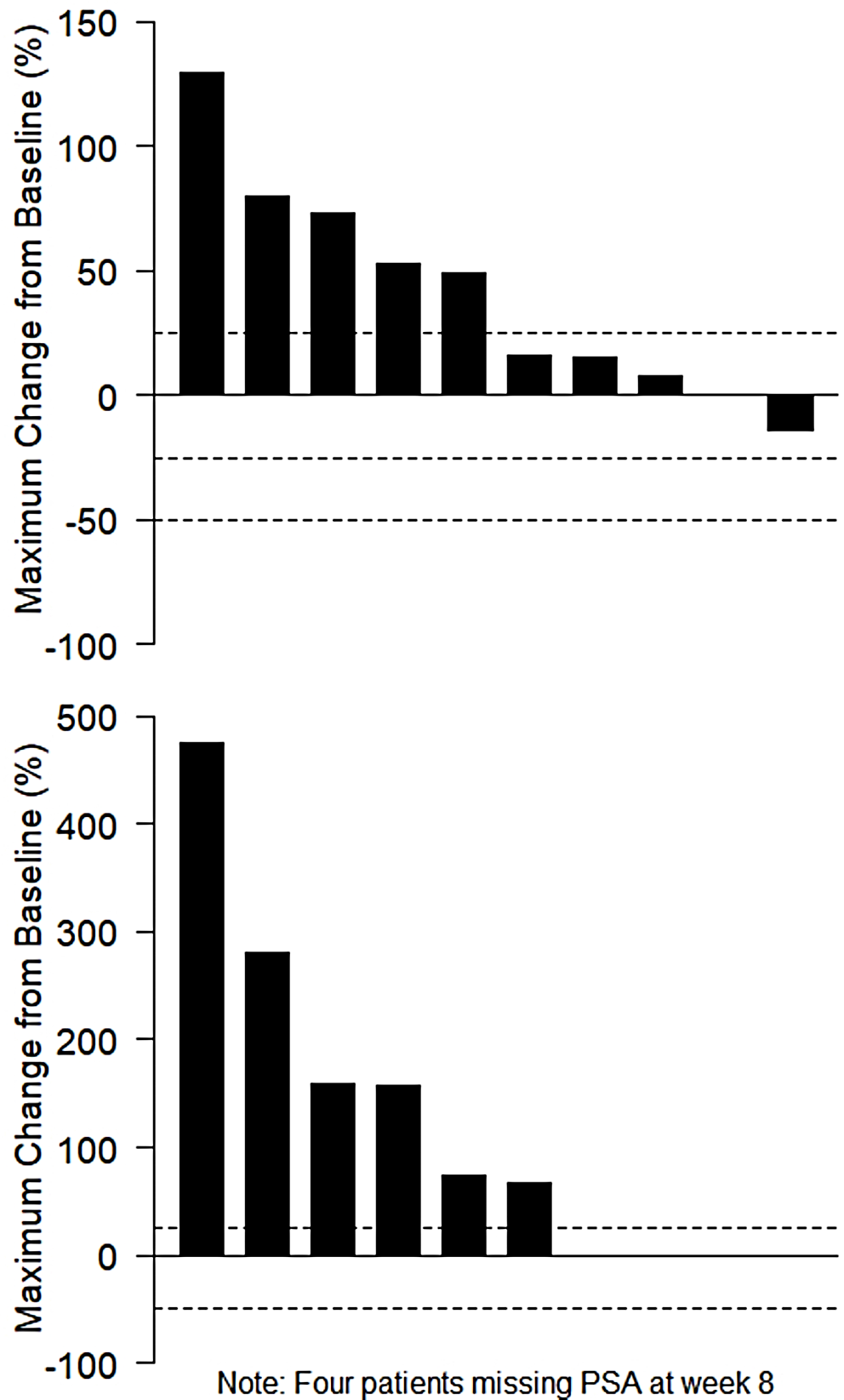
Fig. 1
Waterfall plot of best response among the 41 patients who had measurable lesions at baseline. Each tumor type is color-coded. An upward pointing bar that exceeds 20% represents progressive cancer, a downward bar exceeding 30% indicates a partial response, and the rest of bars are stable diseases. One patient had a partial response of target lesions, but not of non-target lesions. One patient experienced a complete response (not shown). CUP, cancer of unknown primary site; GCT, germ cell tumor; GIST, gastrointestinal stromal tumor; HN, head and neck squamous cell carcinoma; MBC, metastatic breast cancer; NSCLC, non-small cell lung cancer; PR, partial response
Fig. 2
Swimmer’s plot of 46 patients with color codes for each tumor type. The time of first documented response is indicated by a diamond plot. CR, complete response; CUP, cancer of unknown primary site; GCT, germ cell tumor; GIST, gastrointestinal stromal tumor; HN, head and neck squamous cell carcinoma; MBC, metastatic breast cancer; NSCLC, non-small cell lung cancer; PR, partial response
留言 (0)