Data Sources and Search Strategies
A systematic literature search was conducted across multiple databases, including Medline, Embase, CINAHL, and Cochrane Central Register of Controlled Trials to identify relevant studies. All databases were searched between July and November 2023. The search strategies were developed via close consultation with an experienced medical librarian based on Medical Subject Headings (MeSH) terms with input from the authors. The initial search was developed in Medline, and the search strategies have been subsequently adapted to other databases criteria (i.e., Embase, CINAHL, and Cochrane Central Register of Controlled Trials). A hand search for additional articles was done in Google Scholar. The detailed search strategies and the use in different databases can be found in Supplemental material 1 and 2. In addition, we set the limits to all the search to “randomised controlled trials”, “published in the last 10 years” (i.e., 2013–2023), “full text” and “English language”. The updated version of Preferred Reporting Items for Systematic Reviews and Meta-Analyses” (PRISMA) [11] was referred to conduct the current systematic review and meta-analysis. The protocol was registered at PROSPERO (www.crd.york.ac.uk/PROSPERO) as CRD42023471474.
Study Selection
Studies are included if (1) they included adults aged 18 years and older who are at risk of developing T2DM, including prediabetes, high BMI, history of gestational diabetes, family history of diabetes, elevated diabetes risk score, metabolic syndrome; (2) the participants live in the Asia Pacific Region: mainly includes countries in the Asia Pacific region according to the Federal Aviation Administration [5], as mentioned above (e.g., North East Asia, South Asia, South East Asia, and Pacific or West Pacific); (3) RCTs include any lifestyle interventions (e.g., dietary and/or physical activity) that aimed to prevent T2DM; (4) report at least one of the following outcomes as the study main outcome: T2DM incidence, fasting glucose, 2-h glucose (OGTT), HbA1C and/or implementation results. Studies are excluded if (1) they included participants aged < 18 years; (2) participants with diagnosed diabetes (type 1 or type 2); (3) included pregnant women; (4) Taking medication that would alter glycaemic outcomes; (5) Any interventions without diet or physical activity component (e.g., only supplement or pharmacological intervention); (6) combined lifestyles with drugs, supplements, or other treatment. In addition, all editorials, letters, commentaries, conference abstracts, theses/dissertations, study protocols, reviews and other reports are excluded.
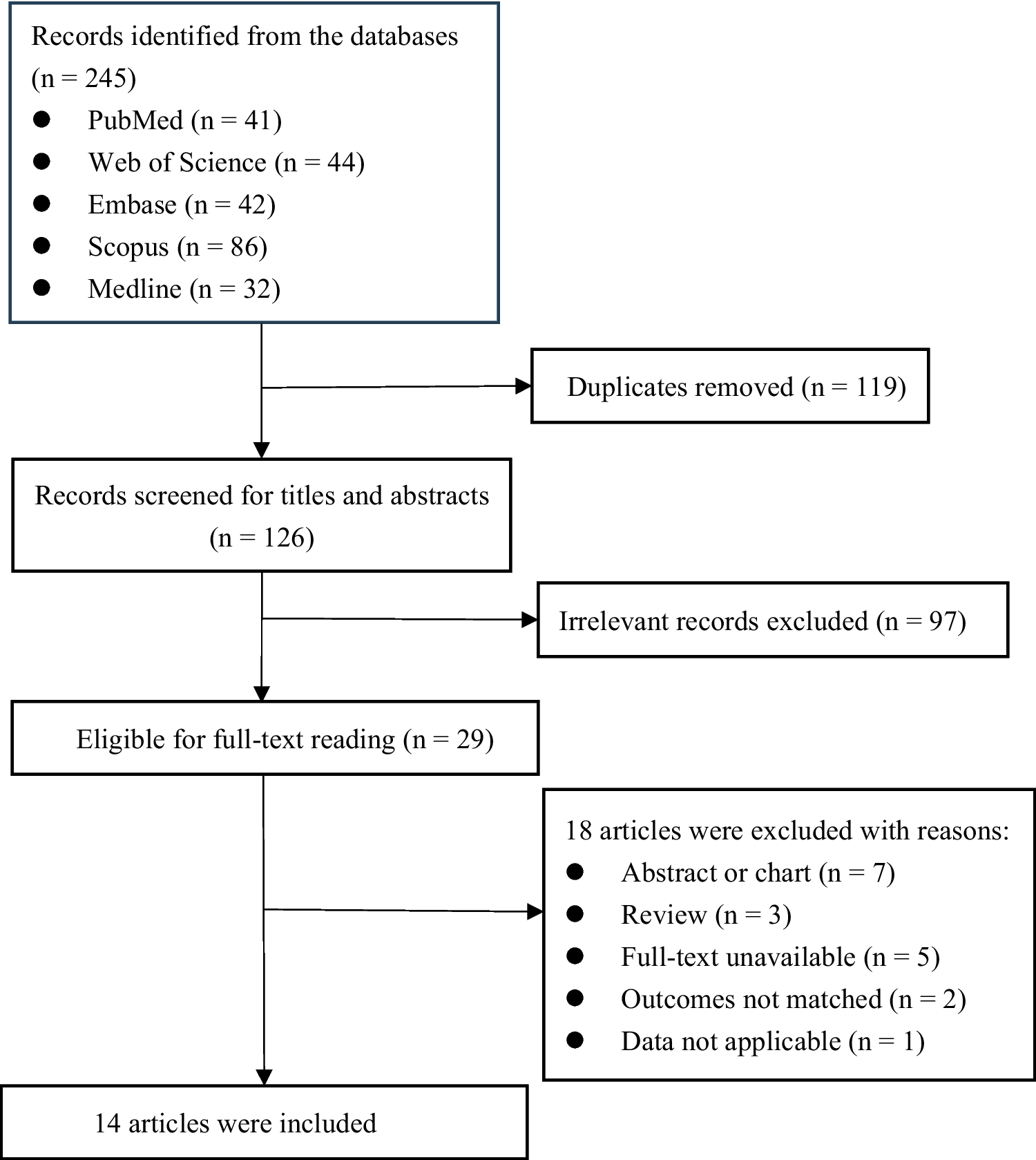
Covidence [12] was used for titles and abstracts screen, as well as full texts review and data extraction. Title and abstract screening and full-text review were performed by TC and AS according to the eligibility defined above. Any discrepancy was checked and resolved by a third reviewer (TH). Data extractions were independently performed by YC, LY, AJ and AS, and any discrepancy were resolved by consensus via group discussion.
Quality Assessments of the Studies
The JBI critical appraisal checklist for randomized control trials [13] was used to assess the quality of studies included in this review by two independent reviewers from the pool of reviewers (YC, LY, AJ and AS). There are 13 questions in total, assessing internal validity (bias related to selection and allocation, bias related to administration of intervention/exposure, bias related to assessment, detection, and measurement of the outcome, bias related to participant retention) and statistical conclusion validity. The risk of bias was assessed as either low, high, or unclear. All discrepancies and disagreements were resolved through consensus, or by a third reviewer that was not involved in the studies in the risk assessment stage.
Data Extraction
Key relevant data from each of the selected studies were extracted using the template in Covidence, with modifications where needed. These data included study characteristics, including study title, first author, country of the study, publication year, sample size, intervention characteristics, follow-up length, and outcomes. Primary outcomes included T2DM incidence (the new cases reported at the end of the study point), glycaemic outcomes (fasting and 2-h glucose levels, and HbA1c). Secondary outcomes (if reported) included anthropometric measures (body weight, BMI, waist circumference), lifestyle behaviors (energy intake and physical activity) and implementation outcomes (cost-effectiveness, feasibility, sustainability, etc.)
Data Synthesis and Analysis
The intervention effects were synthesized using random-effects meta-analysis models on fasting glucose, Hb1Ac, BMI, and waist circumference at 6 months follow-up, based on the available data for most studies. Standardized Mean Differences (SMDs) with 95% confidence intervals (CIs) were employed to represent continuous outcomes. The forest plots visually presented the effect sizes. Homogeneity among studies was assessed using the I² test, with I² > 50% indicating substantial heterogeneity. Following the Cochrane Handbook guidelines [14], an I² of 0–40% might not be important, 30–60% may represent moderate heterogeneity, 50–90% substantial heterogeneity, and 75–100% considerable heterogeneity. Publication bias was examined using funnel plots and Egger’s test. It’s important to note that Egger’s test may lack statistical power with a small number of studies. Therefore, according to Sterne et al., [15], funnel plot asymmetry tests were performed only when 10 or more studies were present. A two-sided P-value < 0.05 was considered statistically significant for all analyses. The meta package in R version 4.3.2 was utilized for conducting the analyses.





留言 (0)