
記住我
A total of 418206 infants were born within KPSC hospitals from 2010 through 2020 including 10252 babies <34 weeks gestation (2.54%). Among all births, 750 infants (0.18%) were exposed to iNO in the NICUs during this period. Thirty-six percent of all infants exposed to iNO (270) were <34 weeks gestational age. The incidence of iNO exposure was 2.63% among preterm births <34 weeks. The rate of iNO exposure reported in the California Perinatal Quality Care Collaborative during the same period [17, 18]. was 2.39% 2539/107876. Two-thirds of these infants (178) were <29 weeks gestation. All infants exposed to iNO irrespective of congenital anomalies, chromosomal aneuploidy, or moribund status were included in the analysis.
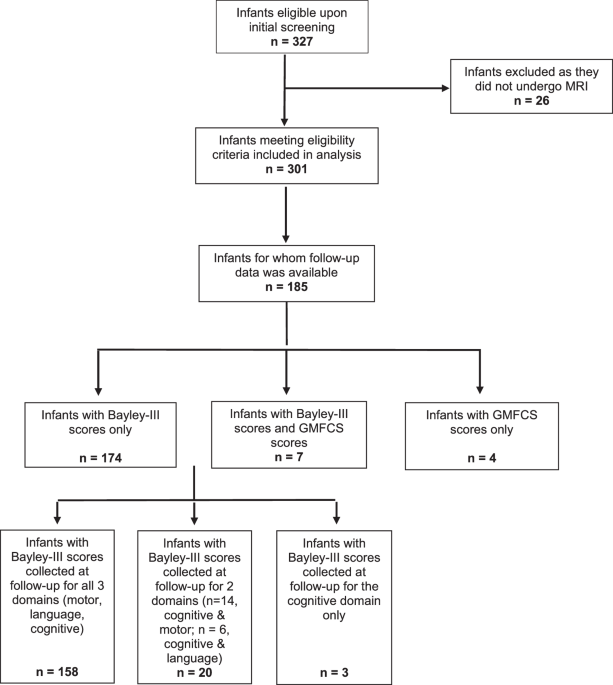
Baseline characteristicsBaseline characteristics of these infants are shown in Table 1 and the flowchart is shown in Fig. 1. Eight infants were born outside the Kaiser network and transferred to KPSC institutions. One growth restricted infant was born at 26 weeks of gestation with a birth weight of 270 g and developed HRF following ductal ligation and received iNO and survived.
Table 1 Baseline characteristics of preterm infants (<34 weeks GA) exposed to iNO (n = 270).Fig. 1: Flowchart of newborn infants born at KPSC between 2010 to 2020.
Preterm infants <34 weeks gestation exposed to iNO (n = 270), and their outcomes are shown. GA gestational age, IVH intraventricular hemorrhage, BPD bronchopulmonary dysplasia, ROP retinopathy of prematurity.
Initiation of iNOCharacteristics of infants at the time of initiation of iNO and duration of iNO exposure are shown in Table 2. The indications for iNO were HRF and PH. Majority of patients (237/270–87.8%) were in HRF and required inspired oxygen >70%. Three-fourth of infants were on 100% inspired oxygen at initiation of iNO. Fifteen infants (5.6%) were receiving ≤50% oxygen and had clinical or echocardiographic evidence of PH (3 infants on 21–30% oxygen, 3 on 31–40% and 9 on 41–50%). Fifty-nine percent of patients were acidotic with a blood pH < 7.25 at iNO initiation. Thirty-two infants (12%) had pH < 7.0 at initiation of iNO. Thirty-five infants 14.6% of 240 infants with sepsis workups had a positive blood culture at the time of iNO initiation.
Table 2 Characteristics at initiation and duration of iNO exposure (n = 270 unless specified).Oxygenation response to iNOWe arbitrarily defined oxygenation response to iNO as an absolute decrease of 25% in inspired oxygen concentration with an increase in SpO2/FiO2 (S/F) ratio by 30 or greater within 2 h of iNO initiation. 88 infants (88/270 = 32.6%) had a positive oxygenation response to iNO. Responders had lower SpO2 (74 ± 20% vs. 80 ± 13%) prior to initiation of iNO. Responders had a lower postnatal age (166 ± 305 vs. 385 ± 603 h) and higher incidence of PH on echocardiogram (49% vs. 35%) compared to non-responders. Survival to discharge was 72% among responders and 58% among non-responders but when corrected for gestational age and sex, this difference was not statistically significant.
EchocardiographyAmong the 84 patients who had echocardiograms performed prior to initiation of iNO, 36 (43%) had evidence of PH. However, only 58 echocardiograms were performed within 24 h of starting iNO and 33 (57%) had evidence of PH. Echocardiography was performed shortly after (usually on a subsequent working day) initiation of iNO in 131 (48.5%) and 50 of them (38%) had evidence of PH. Although most echocardiograms were performed during day-time hours, initiation of iNO occurred round-the-clock suggesting that factors other than echocardiographic evidence of PH (e.g., inability to maintain SpO2 despite 1.0 FiO2) were the primary drivers for initiation of iNO. Fifty-five patients who received iNO never had an echocardiogram done during the NICU course and 32 of these infants died (18 within 24 h of iNO initiation).
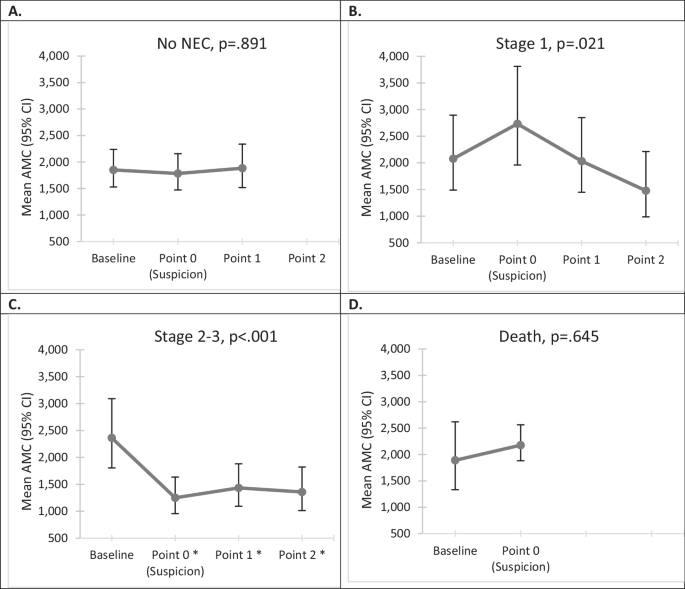
Age at initiation of iNO had a wide distribution ranging from 1 h to 6.5 months (Fig. 2A) – majority of infants received iNO during the first week of postnatal period (58.1%) and some received iNO for PH associated with BPD after the first postnatal month (14.1%). Most infants were treated with surfactant (97.4%) prior to iNO and were ventilated with high frequency-oscillatory or jet ventilation (91.1%; Table 2).
Fig. 2: Day of iNO initiation, cumulative iNO exposure and cumulative mortality.
A Cumulative percentage of preterm infants exposed to iNO based on day of initiation of iNO (n = 270). B Cumulative mortality among 58 infants with echocardiogram performed within 24 h prior to initiation of iNO. PH pulmonary hypertension.
Starting dose of iNO was 20 ppm in 223 (82.6%) of patients with a small number receiving either 5 ppm (4.8%), 10 ppm (10.7%) or 15 ppm (1.5%). One patient was started with 40 ppm of iNO.
Duration of iNO therapyThe duration of iNO therapy ranged from 1 h to 107 days (Table 2). Thirty-five infants received multiple courses of iNO (26–2 courses, 7–3 courses and 2–4 courses). A third of patients (89/270) were exposed to >5 days of iNO therapy.
Co-morbiditiesAt 36 weeks postmenstrual age, among 181 survivors, 115 infants (63.5%) met VON criteria for BPD. Ten infants with BPD at 36 weeks postmenstrual age died before NICU discharge. Intraventricular hemorrhage (IVH) was seen in 94/260 infants (36.2%) with grade 3 IVH in 21 (8.1%) and grade 4 in 31 (11.9%). Ten infants did not meet criteria for head ultrasound due to higher birthweight (>1500 g) and gestational age (>32 weeks). Screening for retinopathy of prematurity (ROP) was performed among preterm infants <30 weeks gestation or <1500 g birth weight. Fifty-nine infants did not have ROP and 37 had stage 3 and 2 had stage 4 ROP. Five infants required Laser therapy (Fig. 1).
Cost of iNOThe total cost of iNO therapy to KPSC for these 270 infants was $3,781,332. A total of 39,804 h of iNO use occurred in the NICU during the study period among infants <34 weeks gestation. The median cost per patient was $7695 with an interquartile range of $9975.
Survival to discharge and NICU mortalitySurvival to discharge overall was 63% (169/270). Nine infants were transferred to level 4 NICUs outside the KPSC network. Survival to discharge among infants who had rupture of membranes (ROM) at delivery was 62.7% (116/185), 71.4% (10/14) with ROM of 1–18 h, 78.3% (18/23) with ROM of 19–120 h and 52.1% with PROM > 120 h (25/48). The overall survival to discharge among infants with ≤18 h of ROM was 63.3% (126/199) and was not statistically different from the 60.6% (43/71) survival among infants with ROM > 18 h. Twenty-eight infants exposed to iNO had a clinical diagnosis of pulmonary hypoplasia and 14 (50%) died. Survival among male infants was 99/154 (64%) compared to 70/116 (60%) among female infants. When adjusted for gestational age, AGA/SGA/LGA status and facility, female sex [OR 2.69 (1.19–7.41), p – 0.02] was associated with improved survival.
Echocardiographic evidence of PH and survivalSurvival to discharge was not different among infants with echocardiographic evidence of PH anytime either before or after initiation of iNO (71.9%–61/86) when compared to those who had no PH on echocardiogram (65.9%–85/129). However, many of these echocardiograms were performed a few days prior to or after initiation of iNO. We selected 58 infants who had echocardiography performed within 24 h prior to initiation of iNO. Among these infants, presence of echocardiographic evidence of PH associated with initiation of iNO during the first 10 postnatal days was associated with improved survival based on unadjusted analysis (Fig. 2B). However, when analysis was adjusted for gestational age, sex, AGA/SGA/LGA status and facility, there was no significant association between presence of PH on an echocardiogram and survival with OR 1.146 (0.45–2.93, p-0.78).
Severity of HRF and survivalSeverity of HRF was related to mortality. Mortality was lower when oxygenation index (OI) was <20 at initiation of iNO (24%) as compared to an OI of 21–40 (45%) or >40 (56%). Since arterial access was not always available at the time of initiation of iNO, we assessed severity of HRF using oxygen saturation index (OSI – Supplementary Table 1). High OSI was associated with increased mortality.
Timing of initiation of iNO had an impact on NICU mortality. Initiation of iNO in the first 72 h after birth was associated with a mortality rate of 44% (64/145). Initiation of iNO in the first week (33.8%–53/157) or 1–4 weeks (21.3%–16/75) was associated with lower mortality compared to initiation of iNO after 4 weeks of postnatal age (84%–32/38).
Effect of race and ethnicity on mortality (Table 1)The NICU mortality in Hispanic infants was 38.2% (49/128), 42% among White (26/62) and 26.5% among Black infants (13/49). This difference was not statistically significant.
Effect of sex (Supplementary Table 3)There was no sex difference in mortality. Differences in mortality among male and female among Black (20.7 vs. 35% respectively), Hispanic (39 vs. 37%) or White infants (37 vs. 50%) did not reach statistical significance.
Growth status (AGA/SGA/LGA)Mortality among small for gestational age infants (SGA) was 27% (10/37), appropriate for gestation (AGA) was 39% (83/212) and among large for gestational age (LGA) infants was 42% (9/21).
The status at discharge from the NICU is shown in Table 3. Seventy-nine infants were discharged home in room air, 71 infants were discharged on supplemental oxygen through a nasal cannula and 19 infants needed a tracheostomy.
Table 3 Outcomes at NICU discharge.Follow-up at 12 monthsSixty-three percent (169/270) of preterm infants who received iNO were discharged alive from the NICU including 9 transfers. Three infants transferred for higher level of care died and 3 were discharged on home ventilator.
Five infants died after NICU discharge at 4 months, 6 months, 1, 2, and 3 years of age. Follow-up information was available for 152 infants (90% of discharged patients). Overall, 19 infants required tracheostomy and 9 were discharged on home ventilation.
The weight, length, and head circumference of all 152 infants were compared using Z-scores at birth, NICU discharge, and at 12 months follow-up using Fenton and WHO growth curves. There was a significant decrease in the Z-score for all three growth parameters from birth to discharge (supplementary Fig. 1). There was a further decrease in length between discharge and 12 months. There was no statistically significant difference between Z-scores for weight and head circumference after discharge.
Mortality after discharge, rehospitalization before 12 months of age, medication use, supplemental oxygen needs, and echocardiographic findings at follow-up are shown in supplementary Table 2. Sixteen infants needed sildenafil therapy and only 4 demonstrated PH on echocardiogram at 12 months. Of note, two infants developed hepatoblastoma and one of them died at 2 years of age. The second infant with hepatoblastoma received chemotherapy and survived. Baseline demographics, characteristics of iNO use and outcomes based on sex are shown in supplementary Table 3.
留言 (0)