
{kind=link}
記住我










Chronic obstructive pulmonary disease remains a major public health problem, associated significant social and economic burden worldwide because of its high prevalence and related disability and mortality.1 In 2019, 212.3 million prevalent cases of COPD were reported globally, with COPD accounting for 3.3 million deaths and 74.4 million DALYs.2 WHO has declared COPD is the 3rd leading cause of death at the global level.3 According to the China Pulmonary Health (CPH) study, the prevalence of COPD in the population aged 20 years or older is 8.6% and aged 40 years or older is 13.7% in China.4 Based on the Global Burden of Disease (GBD) 2019 database, the disease burden of COPD in China is relatively heavy, and the number of affected individuals is still increasing.5
The prevalence and burden of COPD vary across different regions of China, influenced by factors including the economy, society, natural environment, population demographic patterns, and others.6,7 For example, the prevalence of spirometry-defined COPD among the population 40 years or older was 11.6% in Fujian Province,8 9.8% in Anhui Province9 and 9.3% in Shanxi Province.10 Assessing the regional prevalence of COPD is of urgent significance for the development of regional public health policies and better allocating medical resources. Yunnan Province is relatively unique compared to other provinces in China, which is located in the mountainous plateaus of southwestern China, is recognized as one of the economically disadvantaged province in China. It possesses distinctive geographical features, diverse ethnic minority populations, and faces challenges related to tobacco epidemic prevalence. In short, as an undeveloped province in southwest China with a significant tobacco producing province, the substantial disease burden attributable to COPD warrants careful consideration. Despite the existence of numerous investigations concerning COPD within Yunnan province, their scope remains localized to specific geographic regions or demographic population. Thus, there is an urgent need to investigate the prevalence and explore the various risk factors associated with the condition in different regions of Yunnan Province, to promote specific prevention and control measures. To help fill the evidence gap, we conducted a cross-sectional survey, with the aim of including a large population and using screening questionnaire to identify high-risk population for COPD among participants. Then pulmonary function tests are performed on all identified high-risk individuals to estimate the prevalence of COPD and its associated risk factors among high-risk population in Yunnan Province. Furthermore, we collected and assessed the association between the prevalence of COPD and altitude as well as ethnicity.
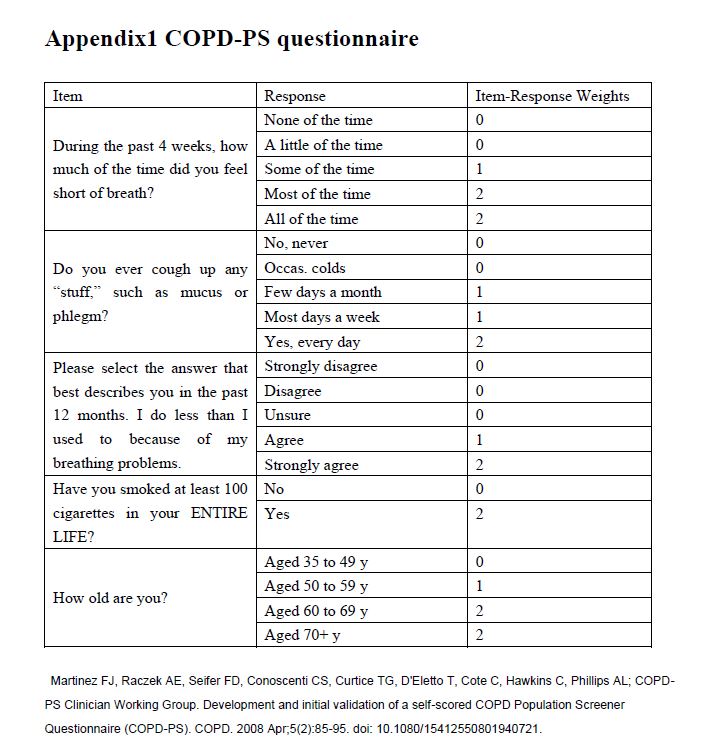
Materials and Methods Study ParticipantsOur study provides reliable estimates of the prevalence of COPD among high-risk populations in Yunnan Province. We used the COPD-PS questionnaire11 (Chinese version) and COPD-SQ questionnaire12 (Chinese version) to conduct initial screening for high-risk population from all study participants. High-risk individuals were defined as those with a COPD-SQ score of 16 or higher, or (and) a COPD-PS score of 5 or higher. The high-risk population consists of all high-risk individuals. Individuals with a COPD-PS score of less than 5 and a COPD-SQ score of less than 16 were classified as non-high-risk individuals. The COPD-PS questionnaire11 (Appendix 1) and COPD-SQ questionnaire12 mainly contain the following information:1) Self-reported chronic cough, chronic expectoration, dyspnea and other chronic respiratory symptoms; 2) Exposure to current or past smoking, indoor use of contaminated fuel and other risk factors; 3) Family history of chronic respiratory diseases. All these high-risk participants underwent a post-bronchodilator pulmonary function test.
We employed a multi-stage cluster sampling methodology to recruit a representative sample of adult residents aged 20 years and above in Yunnan Province. In the first stage, we randomly selected 13 prefectures out of the 16 prefectures in Yunnan Province. In the second stage, we randomly chose one county from each selected prefecture (with the exception of Kunming and Qujing, where 3 and 2 counties were selected, respectively, due to their larger populations) to serve as study sites, resulting in a total of 16 counties selected. Additionally, we selected 4 towns/villages located within the administrative boundaries corresponding to the selected counties. In the third stage, we stratified the final sampling by sex and age distribution based on 2020 China census data.13 We selected only one participant from every household, without replacement. We got the contact information ie name, home address and contact phone number of each selected participant from the Residents’ Health Records System14 (every resident in Yunnan Province has a unique identity (ID) of Residents’ Health Records) (Figure 1). Then village doctors informed every participant to go to the designated place for on-site investigation, when someone did not want to come, continued to carry out simple random sampling for another person to replace him.

Figure 1 Flowchart of participants through the study.
The inclusion criteria for the study population in the sampling frame were as follows: 1) aged 20 years or above; 2) permanent residents within the study sites, with a minimum of 6 months of residency within the past year before the screening; 3) voluntary participation and signed informed consent. The exclusion criteria for enrollment were as follows (if any of the following conditions were met): 1) recent history (within the last 3 months) of myocardial infarction, stroke, or shock; 2) severe heart failure, severe arrhythmias, or unstable angina within the last 4 weeks; 3) massive hemoptysis within the last 4 weeks; 4) chest, abdominal, or ocular surgery within the last 3 months; 5) psychiatric disorders including hallucinations, delusions, use of antipsychotic medications, or epilepsy requiring medication; 6) cognitive impairment, including dementia or impaired comprehension; 7) uncontrolled hypertension (systolic blood pressure >200 mmHg, diastolic blood pressure >100 mmHg), heart rate >120 beats/minute, or aortic aneurysm; 8) severe hyperthyroidism; 9) pregnancy or lactation in females; 10) respiratory infectious diseases (such as tuberculosis or influenza) within the last month.
Based on a national cross-sectional study by the research team led by Wang Chen,4 the prevalence of COPD was found to be 2.1% (in 2018) among individuals aged 20–39, and 13.7% (in 2018) among individuals aged 40 and above. We used the PASS software (NCSS, Kaysville, UT, USA)15 to calculate the sample size. Additionally, considering the possibility of refusal during field surveys, we set a conservative visit success rate of 90% and applied a design effect of 1.2 to account for the multi-stage cluster sampling design. The final sample size was 1053 for the 20–39 age group and 6056 for the 40 and above age group.
EthicsThe study was initiated and led by the First People’s Hospital of Yunnan Province and was approved by the Ethics Committee of the First People’s Hospital of Yunnan Province (KHLL2022-KY141-C-1). Written informed consent has been obtained from all study participants.
Measures Dependent VariableThe dependent variable is the presence of COPD. It is diagnosed based on the results of pulmonary function test. All high-risk participants were subjected to pulmonary function tests using the German Jaeger spirometer (MasterScreen Pneumo, Jaeger).16 Technicians trained in pulmonary function testing and quality control performed pulmonary function tests on all high-risk individuals. Pulmonary function tests were performed strictly in accordance with the guidelines.17,18 The specific operation of pulmonary function test is as follows: Step 1, turn on the pulmonary function instrument and calibrate the instrument. In the step 2, the pulmonary function testing technician explained the examination process to the subjects, demonstrated the examination action, and asked the subjects to practice the examination action, and then checked the essentials of the action. The step 3 is to measure the pulmonary function for pre-bronchodilator (the first pulmonary function test). Step 4, post-bronchodilator pulmonary function test (the second pulmonary function test): for individuals with a pre-bronchodilator FEV1/FVC < 0.7, inhale bronchodilator (salbutamol 400 μg) through a 500 mL spacer, and wait for 15 minutes, a post-bronchodilator pulmonary function test was conducted to confirm the diagnosis of COPD. Individuals who had dyspnea, chronic cough or sputum production, a history of recurrent lower respiratory tract infections and/or a history of exposure to risk factors for the disease with a post- bronchodilator FEV1/FVC < 0.7 were diagnosed as COPD patients.1
Independent VariableAll baseline covariates data were obtained by trained interviewers through standard questionnaires.4 Age, gender, nationality, and education level are self-reported. Body mass index (BMI) is defined as weight (kg) divided by the square of height (m). Marital status is divided into in marriage and not in marriage. We define current smoking as the act of having consumed a minimum of 100 cigarettes throughout one’s lifetime and presently continuing to smoke. Passive smoking is characterized as the inhalation of smoke by non-smokers in the presence of smokers. Family history of respiratory system diseases is designated by whether any individuals within the family have been diagnosed with conditions such as COPD, chronic bronchitis, or emphysema et al. Childhood history of respiratory system diseases is defined as having encountered pneumonia, asthma, bronchitis, or other respiratory system diseases at least once before the age of 14. Biomass fuel use is defined as the predominant utilization of wood fuel or animal dung for cooking or heating purposes for a period of six months or longer within the past. The counties in Yunnan Province have an altitude coefficient that varies greatly by location, ranging from 64.8 to 334.7. 16 counties in this study are categorized as high altitude (altitude>2500), middle altitude (altitude: 1500–2500), and low altitude (altitude<1500). Based on population reference values from China, we calculated the ratios of observed to predicted FEV1 and utilized them to classify the degree of obstruction. This classification includes the following stages: GOLD stage I (≥80% predicted), GOLD stage II (≥50% to <80% predicted), GOLD stage III (≥30% to <50% predicted), and GOLD stage IV (<30% predicted).19
Statistical AnalysisStatistical significance evaluation for continuous variables was conducted using non-parametric test, whereas chi-square tests were used for categorical variables. The multivariable logistic regression analysis was conducted to investigate the risk factors for COPD among all high-risk populations and high-risk individuals who have never smoked. Due to the small sample size of GOLD stage IV (n=29), individuals with GOLD stage III and IV were merged for analysis. The SPSS software (Version 26) was used to carry out all statistical analyses. All statistical inferences were set as a two-tailed p-value less than 0.05.
Results Demographic Characteristics and Risk Factors for COPD by GOLD Stage in the High-Risk PopulationBetween November 2022 and June 2023, a total of 12,481 eligible individuals (5841 males and 6640 females) were invited to participate in the survey. Of these, 11,095 individuals (including 5001 males and 6094 females) completed the study (see Figure 1). The overall response rate was 88.90% (85.62% for males and 91.78% for females). Of them, there are 2252 high-risk individuals and 8843 non-high-risk individuals. After excluding individuals with incomplete pulmonary function test or missing key variables, a total of 2252 high-risk individuals (1463 males and 789 females) were included in the final analysis.
The general characteristics and risk factors of the study population, stratified by COPD severity, are presented in Table 1. The prevalence of COPD by GOLD stages I, II, and III–IV was, respectively, 9.99%, 11.10%, and 6.08% in the high-risk population. The distribution of patients in GOLD stages I, II, and III–IV showed a significant male predominance compared to females, with statistically significant differences (P<0.05). Additionally, as age increased, the proportion of patients in each stage gradually increased. Individuals with lower education levels had a higher proportion of disease prevalence. Moreover, in low and mid-altitude areas, there was a larger proportion of patients in each stage, with statistically significant differences (the p-values for all the mentioned associations are less than 0.05). The remaining characteristics of study population with COPD are shown in Table 1.

Table 1 Demographic Characteristics and Risk Factors for COPD by GOLD Stage in the High-Risk Population of Adults Aged 20 Years and Above in Yunnan Province, China in 2022
Prevalence of COPD in the High-Risk PopulationAmong the high-risk population aged 20 years and above in Yunnan, the overall prevalence of COPD diagnosed based on lung function was 27.18% (95% CI 25.35–29.06). The prevalence among males (33.01%, 95% CI 30.61–35.49) was higher than females (16.35%, 95% CI 13.84–19.12; p<0.001, significant gender difference). This gender difference was observed in all age groups of the high-risk population and never-smoking high-risk population (see Table 2). The prevalence of COPD increased with age, with rates of 8.29% (95% CI 5.46–13.58) among individuals aged 20–49 years, 24.07% (95% CI 20.51–27.92) among those aged 50–59 years, 27.17% (95% CI 24.21–30.28) among those aged 60–69 years, and 35.75% (95% CI 32.06–39.57) among individuals aged 70 years and above (p<0.001 for age difference). The prevalence of COPD in the underweight population (BMI<18.5 kg/m2) was 41.24% (95% CI 33.91–48.87). In the normal weight population (BMI 18.5–24.9 kg/m2), the prevalence of COPD was 28.85% (95% CI 26.51–31.29), in the overweight population (BMI 25.0–29.9 kg/m2), the prevalence of COPD was 20.00% (95% CI 16.72–23.61), and in the obese population (BMI≥30.0 kg/m2), the prevalence of COPD was 18.35% (95% CI 11.58–26.91). It can be observed that as BMI increased, the prevalence of COPD in high-risk populations decreased, and this difference was statistically significant (trend test p-value < 0.001). This difference is observed in both males and females, as well as in high-risk populations who have never smoked (see Table 2). As education level increases, the prevalence of COPD decreases accordingly, with statistically significant differences (P<0.05).

Table 2 Prevalence of COPD in the High-Risk Population Aged 20 and Above Based on Spirometry in Yunnan Province in 2022
The prevalence of COPD among never smokers was 19.83% (95% CI 17.34–22.51), among former smokers was 38.86% (95% CI 34.67–43.18), and among current smokers was 28.29% (95% CI 25.14–31.61), with statistically significant differences (P<0.001). This difference trend was also observed in males, while no such difference was observed in females. Furthermore, as smoking amount increases, the prevalence of COPD also increases accordingly, with statistically significant differences (trend test p-value < 0.001). Individuals with a history of respiratory system diseases during childhood have a significantly higher prevalence of COPD (38.17%, 95% CI 29.82–47.06) compared to those without a history of respiratory system diseases during childhood (26.75%, 95% CI 24.82–28.75), with statistically significant differences (P<0.05). This difference is observed in both males and females, as well as in high-risk populations who have never smoked.
The incidence rate of COPD exhibits a notable disparity among regions of varying altitudes. A comprehensive analysis reveals a heightened prevalence of COPD in low-altitude areas, estimated at 26.44% (95% CI 23.38–29.67), as well as in mid-altitude counties, approximated at 28.71% (95% CI 26.28–31.24). In contrast, high-altitude regions display a comparatively lower prevalence rate of 17.95% (95% CI 12.27–27.89), with statistically significant differences (P<0.05). This notable divergence is further evident within high-risk groups including both males and females (Figure 2).

Figure 2 Prevalence of spirometry-defined COPD among high risk population aged 20 years or older in different altitude regions of Yunnan Province in 2022. Bars represent proportion and error bars 95% CI. COPD=chronic obstructive pulmonary disease.
In the Han Chinese population, the spirometry-defined prevalence of COPD was documented at 27.79% (95% CI, 25.69–29.96). Among this population subset, the prevalence among males was observed to be significantly higher at 33.63% (95% CI, 30.88–36.46) as compared to females with a prevalence rate of 16.78% (95% CI, 13.88–20.01). Similarly, among minority ethnic groups, the overall COPD prevalence was reported as 25.10% (95% CI, 21.40–29.08). Further stratification by gender revealed a higher prevalence among males at 30.89% (95% CI, 25.92–36.20), while among females, it was lower at 14.97% (95% CI, 10.19–20.91). Notably, the observed differences in COPD prevalence between genders were found to be statistically significant. These findings contribute valuable insights into the epidemiology of COPD within the Han Chinese and minority ethnic populations, underscoring the importance of gender-specific considerations in disease management and prevention strategies (Figure 3).

Figure 3 Prevalence of spirometry-defined COPD among high risk population aged 20 years or older in different ethnic groups of Yunnan Province in 2022. Bars represent proportion and error bars 95% CI. COPD=chronic obstructive pulmonary disease.
Result of Multivariate Analysis of COPDIn the multivariable adjusted analysis, male gender (OR=2.291, 95% CI: 1.584–3.313), age (OR=1.501, 95% CI: 1.338–1.685), underweight (BMI<18.5kg/m2) (OR=1.747, 95% CI: 1.225–2.491), previous smoking (OR=1.712, 95% CI: 1.182–2.478), passive smoking (OR=1.444, 95% CI: 1.159–1.800), and a history of respiratory system diseases in childhood (OR=2.010, 95% CI: 1.346–3.001) were significantly associated with an increased risk of COPD. Conversely, being overweight (BMI 25.0–29.9kg/m2) (OR=0.636, 95% CI: 0.489–0.828), having a family history of respiratory system diseases (OR=0.722, 95% CI: 0.540–0.965), and residing in high-altitude counties (OR=0.445, 95% CI: 0.263–0.754) were negatively correlated with the risk of COPD (see Table 3). Furthermore, among never smokers, family history of respiratory system diseases and altitude showed no significant association with COPD, while the other influencing factors were consistent with the entire population.

Table 3 Multiple-Adjusted ORs for COPD Associated with Risk Factors in the General Adult High-Risk Population Aged 20 Years or Older in Yunnan Province in 2022
DiscussionTo the best of our knowledge, our study represents the largest survey of COPD in a representative sample of the general adult population in Yunnan Province, and it fills several knowledge gaps about the COPD epidemic in Yunnan. Our investigation utilized COPD-SQ and COPD-PS screening tools in a large-scale population and then used pulmonary function test to diagnose COPD. Most surveys on the prevalence of COPD use the method of pulmonary function test across the entire population, with few studies using a combination of screening questionnaires and pulmonary function test. There are three reasons why we adopt this approach. Firstly, the US Preventive Services Task Force recommended against screening for COPD in asymptomatic adults and stated that whole-population screening for COPD using spirometry has no net benefit.20,21 Secondly, previous studies have shown that screening in primary care has been demonstrated to have a significant impact.22,23 Finally, the economy of Yunnan Province is underdeveloped, and the level of economic development in different regions is uneven. A cross-sectional analysis demonstrated that screening instruments for COPD were feasible to administer in the low- and middle-income settings.24 So, through the research implementation process, we have confirmed the feasibility of screening questionnaire combined with pulmonary function test in the early detection of COPD in Yunnan Province, especially in primary care of county hospitals and township health centers which are the cornerstones of Chinese medical system.
We found that high-risk individuals for COPD accounted for 20.30% of the screened population aged 20 years and older. And the prevalence of spirometry-defined COPD among the high-risk individuals was 27.18%. The research which used COPD-SQ combined with pulmonary function test from across the country showed that among the high‐risk population who received pulmonary function test, 31.59% were screened and diagnosed as COPD patients.25 This ratio is higher than that of our study, which may be related to different sampling methods. Another study in Fengning Manchu Autonomous County used COPD-PS combined with pulmonary function test, the prevalence of spirometry-defined COPD among the high-risk individuals was 24.27%.26 The study also showed that for COPD high risk patients, receiving early screening has a cost-effective advantage over no screening.
Additionally, we observed a higher proportion of severe and extremely severe COPD patients in Yunnan Province than the national average and other provinces. The results of this study showed that severe and very severe COPD cases (GOLD stages III–IV) accounted for 22.4% of all COPD patients, which was much higher than the national level (7.4%)6 and other provinces (2.4% in Gansu,27 4.9% in Guizhou,28 and 7.0% in Zhejiang29). Yunnan Province is located in Yunnan-Guizhou Plateau, with special geographical environment and backward economic development, which leads to limited medical accessibility, and these severe and extremely severe COPD patients have not been diagnosed and treated in time. That may be a reason why the proportion of severe and extremely severe COPD patients in Yunnan is higher than that in other regions. Which indicates that the severity of COPD in Yunnan Province is relatively high, emphasizing the urgent need for early diagnosis and detection of COPD patients in Yunnan Province.
COPD is the result of the interaction of multiple factors such as genetics, environment, and growth and development. The risk factors causing COPD have diverse characteristics. Well known risk factors include tobacco and second-hand tobacco, biomass exposure, occupational exposure, low BMI, family history and childhood history of respiratory disease, socioeconomic status, etc.30–32 Consistent with these, we also found that males, low BMI, childhood history of respiratory disease and smoking were risk factors. However, we did not find any family history of respiratory diseases or biomass exposure as risk factors. Against other studies,33,34 this research demonstrates that individuals with a family history of respiratory system diseases (OR=0.722, 95% CI: 0.540–0.965) were negatively correlated with COPD. Our data demonstrates that a considerable percentage of males (66.4%) and those aged above 50 years (92.1%) in the high-risk category do not possess a family history of respiratory diseases. Further, among this group, there is a high incidence of smoking (59.1%). This observation may imply that a family history of respiratory diseases serves as a protective factor against developing COPD. This phenomenon may arise from individuals with a familial predisposition to respiratory ailments altering their personal habits, notably abstaining from smoking, as a proactive measure against respiratory afflictions. But we can explore it further on the pathophysiological mechanism for the argument that family history of respiratory disease may serve as a protective factor against developing COPD in the following research.
The analysis of this study revealed that the prevalence of COPD in high-risk male population was 33.01% (95% CI: 30.61–35.49%), which was significantly higher than the prevalence in females, which was 16.35% (95% CI: 13.84–19.12%). This difference was statistically significant (P < 0.001). Gender is an important factor influencing the risk of developing COPD, with multiple studies finding that males are at a higher risk for COPD, whereas females are associated with lower disease risk.35 Both domestic and international studies36–38 have shown a significant trend of higher COPD prevalence in males compared to females, and smoking, as the main risk factor for COPD,39 has a significantly higher prevalence and smoking intensity in males compared to females,4 which may be the main reason for the significant difference in COPD incidence between genders. Additionally, the incidence of COPD increases with age, which may be due to age-related declines in bodily function and organ function, as well as the increased rigidity of the chest wall, reduced lung elastic recoil, decreased airway diameter, and degeneration of elastic fibers around the alveolar ducts, leading to decreased lung function.40 The incidence of COPD is also closely related to the duration of exposure to risk factors.
Smoking is a well-established risk factor for developing COPD.4,41–43 Our data also reveals that former smokers (OR=1.712,95% CI 1.182–2.478) have a higher risk of COPD. Furthermore, in view of the high prevalence of passive smoking and COPD among non-smokers. Passive smoking has been associated with COPD in epidemiological studies.44,45 Smoking prevention and cessation are important strategies for reducing the burden of COPD and related diseases in populations. But we are surprised that in the multivariate analysis, present smokers had a non-significant OR for COPD. The participants of this study is high-risk population. Besides smoking accidents, other risk factors such as age, family history of respiratory diseases and chronic respiratory diseases are also considered when screening high-risk population. Whether other risk factors dilute the influence of smoking on COPD needs further in-depth study. And we found the prevalence of COPD among never smokers was high 19.83%. This observation suggests that, in addition to smoking, alternative factors such as respiratory infections and environmental exposures may also contribute to the occurrence of COPD. Which is also reported by Rotterdam Study.46
This finding is consistent with Wang Chen’s research on the influence of BMI on COPD,4 which shows that underweight (body mass index < 18.5 kg/m2) may be an important risk factor for individuals to develop COPD and overweight and obese (BMI>25 kg/m2) individuals are less likely to have COPD compared to those with normal weight. Meanwhile, Xingyao Tang et al47 research on the relationship between BMI and lung function also showed the same finding. The interplay between BMI and COPD is intricate. Certain academics posit48 that they mutually exacerbate each other. Firstly, the dysregulation between energy expenditure and dietary intake in COPD patients precipitates BMI decline. Conversely, diminished BMI instigates muscle protein degradation and alterations in muscle fiber architecture, culminating in respiratory muscle atrophy and weakened respiratory muscle strength. This diminishes immunoglobulin and complement production, impairing immune function and heightening susceptibility to respiratory infections, thereby exacerbating respiratory ailments. These findings underscore the importance of emphasizing nutritional support and ameliorating low body weight in COPD management.
Individuals with a history of respiratory system diseases in childhood (OR=2.010, 95% CI: 1.346–3.001) were significantly associated with an increased risk of COPD. Research suggests that during pregnancy, at birth, and during adolescence, any direct or indirect exposure factors that can affect lung growth and development have the potential to increase the risk of developing COPD. Poor lung growth and development are identified as independent risk factors for COPD.49,50 The most crucial factors in this regard are low birth weight and childhood lower respiratory tract infections, which have significant impacts on the development of COPD.
We found that high altitude has a significant protective effect on the prevalence of COPD. Studies abroad show that the incidence of COPD is negatively correlated with altitude.51,52 Some scholars believe that this may be related to the increase of airway diameter in plateau environment than the increase of lung volume. In addition, the air density in plateau area decreases, and the atmospheric pressure also decreases, which leads to the increase of FEV1/FVC solid ratio, which eventually leads to the low incidence of chronic obstructive pulmonary disease in plateau.28 Some scholars also believe that53,54 with the passage of time and the development of generations, people in high altitude areas have undergone physiological and genetic adaptation in order to adapt to extreme heights and cope with chronic hypoxia and ordinary high-intensity exercise. However, the relationship between altitude and COPD is controversial. A pooled analysis of individual data from the PREPOCOL-PLATINO-BOLD-EPI-SCAN studies shows living at high altitude is not associated with a difference in COPD prevalence after accounting for individual risk factors. However, high altitude itself was associated with an increased risk of undiagnosed COPD.55 A cross-sectional study based on Gansu population from China points out that high altitude is a risk factor for COPD.56 Therefore, we need to conduct more research to explore the relationship between high altitude and COPD in the future. There are many ethnic minorities in Yunnan province, however this study shows that there is no statistical difference in the prevalence of COPD between Han nationality and ethnic minorities among high-risk population. But Brakema EA et al57 showed that high COPD prevalence at high altitude, the household air pollution plays an important role in explaining the high prevalence of COPD at high altitude.
Our study has several limitations. Firstly, it is a cross-sectional study, which cannot establish a causal relationship between COPD and its influencing factors. However, the findings of this study are consistent with previous literature. Secondly, individuals with COPD-PS<5 and COPD-SQ<16 were not screened for pulmonary function, which may have resulted in the exclusion of some COPD patients. In future research, a sample from this subgroup will be screened for pulmonary function. Thirdly, air pollution as a vital risk factor for COPD. But our study only collected the information of biofuels used to indirectly and roughly assess the indoor air pollution. Despite the above limitations, our study suggested that it is necessary to carry out early screening, early diagnosis and early treatment of COPD in Yunnan Province. Identifying high-risk groups, carrying out publicity and education, pulmonary function screening and consulting services, and improving individual protection awareness and physical fitness are the keys to COPD prevention and treatment.
ConclusionOur data indicate that COPD has a high prevalence (27.18%) among the adult high-risk population in Yunnan Province, China. The proportion of severe and very severe COPD patients in Yunnan Province is higher than the national average and other provinces. Male, age, underweight (BMI<18.5kg/m2), previous smoking, passive smoking, and a history of respiratory system diseases in childhood were significantly associated with an increased risk of COPD. Conversely, high-altitude residence has been found to be associated with a lower prevalence of COPD. There is no significant difference in COPD prevalence between Han and ethnic minority populations. Smoking is a major preventable risk factor for this disease. Prevention and early detection of COPD should be a public health priority in Yunnan Province to reduce the incidence and mortality rates associated with this disease.
AbbreviationsCOPD, Chronic Obstructive Pulmonary Disease; GOLD, Global Initiative for Chronic Obstructive Lung Disease; FEV1, Forced Expiratory Volume in 1 second; FVC, Forced Vital Capacity; OR=Odds Ratio; CI= Confidence Interval; BMI, Body mass index.
Data Sharing StatementData generated and/or analyzed during the study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to ParticipateThis study strictly complies with the Declaration of Helsinki. The study was initiated and led by the First People’s Hospital of Yunnan Province and was approved by the Ethics Committee of the First People’s Hospital of Yunnan Province (KHLL2022-KY141-C-1). Written informed consent has been obtained from all study participants.
AcknowledgmentsWe would like to thank Liping Chen (the First People’s Hospital of Anning), Yunyan Zeng (the second people’s hospital of Baoshan), Juan Wu (the People’s Hospital of Changning County), Jianglei Li (the People’s Hospital of Chuxiong Yi Autonomous Prefecture), Guohui Li (the People’s Hospital of Deqin Tibetan Autonomous Prefecture), Qiong Huang (the People’s Hospital of Huize County), Zhishan Che (the First People’s Hospital of Lancang County), Xiao Zhao (the People’s Hospital of mengzi city), Yongfang Zhang (the People’s Hospital of Songming County), Meiyan He (the People’s Hospital of Xishuangbanna Prefecture), Yonglan Qi (the People’s Hospital of Xiangyun County), Heping Fu (the First People’s Hospital of Xuanwei City), Liang Xu (the people’s hospital of Yanshan county), Zhongyuan Zhang (the First People’s Hospital of Yiliang County), Hong Gao (the Third People’s Hospital of Yuxi), Yunwu Ou (the People’s Hospital of Yun County), Jiang Wang (the First People’s Hospital of Zhaotong City). We thank Academician Chen Wang, Professor Simiao Chen, Professor Ting Yang and other members of the academician team.
FundingThis study was funded by the Strategic Research and Consulting Project of “Comprehensive Prevention and Control of Chronic Obstructive Pulmonary Disease in Yunnan Province based on Population Medical Model” of Chinese Academy of Engineering (NO. 2022-DFZD-30).
DisclosureThe authors declare that they have no conflicts of interest in this work.
References1. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. 2024 report. Available from: https://goldcopd.org/2024-gold-report/. Accessed May14, 2024.
2. Collins GS, Kolahi AA, Kaufman JS. Burden of chronic obstructive pulmonary disease and its attributable risk factors in 204 countries and territories, 1990-2019: results from the Global Burden of Disease Study 2019. BMJ. 2022;378:e069679. doi:10.1136/bmj-2021-069679
3. World Health Organization. The top 10 causes of death.2020. Available from: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death. Accessed May14, 2024.
4. Wang C, Xu J, Yang L, et al. Prevalence and risk factors of chronic obstructive pulmonary disease in China (the China Pulmonary Health [CPH] study): a national cross-sectional study. Lancet. 2018;391(10131):1706–1717. doi:10.1016/S0140-6736(18)30841-9
5. Li M, Hanxiang C, Na Z, et al. Burden of COPD in China and the global from 1990 to 2019: a systematic analysis for the Global Burden of Disease Study 2019. BMJ Open Respir Res. 2023;10(1):e001698. doi:10.1136/bmjresp-2023-001698
6. Fang L, Gao P, Bao H, et al. Chronic obstructive pulmonary disease in China: a nation- wide prevalence study. Lancet Respir Med. 2018;6:421–430. doi:10.1016/S2213-2600(18)30103-6
7. Yin P, Wu J, Wang L, et al. The burden of COPD in China and its provinces: findings from the global burden of disease study 2019. Front Public Health. 2022;10:859499. doi:10.3389/fpubh.2022.859499
8. Chen J, Yin Y, Zhang Y, et al. Chronic obstructive pulmonary disease prevalence and associated risk factors in adults aged 40 years and older in southeast China: a cross-sectional study during 2019-2020. Int J Chron Obstruct Pulmon Dis. 2022;17:2317–2328. doi:10.2147/COPD.S377857
9. Zha Z, Leng R, Xu W, et al. Prevalence and risk factors of chronic obstructive pulmonary disease in Anhui Province, China: a population-based survey. BMC Pulm Med. 2019;19(1):102. doi:10.1186/s12890-019-0864-0
10. Wang R, Xu J, Wang Y. A population-based survey of the prevalence and risk factors of chronic obstructive pulmonary disease in Shanxi Province, China. Rev Clin Esp. 2022;222(4):218–228. doi:10.1016/j.rceng.2021.04.011
11. Martinez FJ, Raczek AE, Seifer FD, et al. Development and initial validation of a self-scored COPD Population Screener Questionnaire (COPD-PS). COPD. 2008;5(2):85–95. doi:10.1080/15412550801940721
12. Zhou YM, Chen SY, Tian J, et al. Development and validation of a chronic obstructive pulmonary disease screening questionnaire in China. Int J Tuberc Lung Dis. 2013;17(12):1645–1651. doi:10.5588/ijtld.12.0995
13. National Bureau of Statistics of China. 2020 Population Census; 2020. Available from: https://www.stats.gov.cn/english/Statisticaldata/yearbook/. Accessed May14, 2024.
14. Zheng YW, Huang B, Fan GH. Summary of the scope of the promotion effect of electronic health records combined with new media carriers on community residents’ health. Chine General Med. 2023;21(06):1048–1052. doi:10.6766/j.cnki.issn.10016.100100001106
15. Newcombe RG. Two-sided confidence intervals for the single proportion: comparison of seven methods. Stat Med. 1998;17(8):857–872. doi:10.1002/(sici)1097-0258(19980430)17:8<857::aid-sim777>3.0.co;2-e
16. Feng Y, Yu XH, Song YX, et al. Establishment of a predictive equation for pulmonary ventilation function in school-aged children in northeast China: a prospective study. Zhongguo Dang Dai Er Ke Za Zhi. 2021;23(11):1119–1126. doi:10.7499/j.issn.1008-8830.2108139
17. Task Force for Pulmonary Function of Chinese Thoracic Society. Guidelines for Pulmonary Function Testing (Part 2) – spirometry. J Chine Tuberculosis Respir Dis. 2014;37(7):481–486. doi:10.3760/cma.j.issn.1001-0939.2014.07.001
18. Task Force for Pulmonary Function of Chinese Thoracic Society. Guidelines for Pulmonary Function Testing (Part 4)—Bronchodilation Test. J Chine Tuberculosis Respir Dis. 2014;37(9):655–658. doi:10.3760/cma.j.issn.1001-0939.2014.09.007
19. Jian W, Gao Y, Hao C, et al. Reference values for spirometry in Chinese aged 4-80 years. J Thorac Dis. 2017;9(11):4538–4549. doi:10.21037/jtd.2017.10.110
20. Siu AL, Bibbins-Domingo K; US Preventive Services Task Force (USPSTF), et al. Screening for chronic obstructive pulmonary disease: US Preventive Services Task Force recommendation statement. JAMA. 2016;315:1372–1377. doi:10.1001/jama.2016.2638
21. Preventive Services Task Force US, Mangione CM, Barry MJ, et al. Screening for Chronic Obstructive Pulmonary Disease: US Preventive Services Task Force Reaffirmation Recommendation Statement. JAMA. 2022;327(18):1806–1811. doi:10.1001/jama.2022.5692
22. Yawn BP, Duvall K, Peabody J, et al. The impact of screening tools on diagnosis of chronic obstructive pulmonary disease in primary care. Am J Prev Med. 2014;47(5):563–575. doi:10.1016/j.amepre.2014.07.030
23. Yawn BP, Martinez FJ. POINT: can Screening for COPD Improve Outcomes? Yes Chest. 2020;157(1):7–9. doi:10.1016/j.chest.2019.05.034
24. Siddharthan T, Pollard SL, Quaderi SA, et al. Discriminative Accuracy of Chronic Obstructive Pulmonary Disease Screening Instruments in 3 Low- and Middle-Income Country Settings. JAMA. 2022;327(2):151–160. doi:10.1001/jama.2021.23065
25. Li W, Huang K, Tang XY, et al. Analysis of screening status of high-risk population of chronic obstructive pulmonary disease in “Happy Breathing” project area. Chine J Health Management. 2022;16(02):77–82. doi:10.3760/cma.j.cn115624-20210503-00239
26. Du M, Hu H, Zhang L, et al. China county based COPD screening and cost-effectiveness analysis. Ann Palliat Med. 2021;10(4):4652–4660. doi:10.21037/apm-21-812
27. Li YL. Prevalence and Influencing Factors Analysis of Chronic Obstructive Pulmonary Disease in Rural Areas of Gansu Province. Lanzhou University; 2021.
28. Huang L. Prevalence and Influencing Factors Analysis of Chronic Obstructive Pulmonary Disease Among Residents Aged 40 Years and Above in Guizhou Province. Guizhou Medical University; 2022.
29. Chen XY, Fang L, Zhao M, et al. Study on the prevalence and influencing factors of chronic obstructive pulmonary disease among residents aged 40 years and above in Zhejiang Province in 2019. Chine Jo Chronic Dis Prevention Control. 2023;31(02):96–100.
30. Adeloye D, Song P, Zhu Y, et al. Global, regional, and national prevalence of, and risk factors for, chronic obstructive pulmonary disease (COPD) in 2019: a systematic review and modelling analysis. Lancet Respir Med. 2022;10(5):447–458. doi:10.1016/S2213-2600(21)00511-7
31. Global strategy for prevention, diagnosis and management of COPD: 2024 Report. Available from: https://goldcopd.org/2024-gold-report/. Accessed May14, 2024.
32. Chuchalin AG. Guidelines for diagnosis and treatment of chronic obstructive pulmonary disease (revised in 2021). Chine J Tuberculosis Respiration. 2021;44(3):36.
33. Foreman MG, Wilson C, DeMeo DL, et al. Alpha-1 antitrypsin PiMZ genotype is associated with chronic obstructive pulmonary disease in two racial groups. Ann Am Thorac Soc. 2017;14(8):1280–1287. doi:10.1513/AnnalsATS.201611-838OC
34. Fell AKM, Svendsen MV, Kim JL, et al. Exposure to second-hand tobacco smoke and respiratory symptoms in non-smoking adults: cross-sectional data from the general population of Telemark, Norway. BMC Public Health. 2018;18(1):843. doi:10.1186/s12889-018-5771-4
35. Yin L, Huang YL, Jin DH, et al. Analysis of the prevalence and influencing factors of chronic obstructive pulmonary disease among residents aged 40 years and above in Hunan Province. Chine Jo Chronic Dis Prevention Control. 2020;28(10):731–734.
36. Soriano JB, Alfagemec I, Miravitlles M, et al. Prevalence and determinants of COPD in Spain: EPISCAN II. Arch Bronconeumol. 2021;57(1):61–69. doi:10.1016/j.arbres
37. Leung C, Bourbeau J, Sin DD, et al. The prevalence of chronic obstructive pulmonary disease (COPD) and the heterogeneity of risk factors in the Canadian population: results from the Canadian Obstructive Lung Disease (COLD) study. Int J Chron Obstruct Pulmon Dis. 2021;16:305–320. doi:10.2147/COPD.S285338
38. Hwang YI, Park YB, Yoo KH. Recent trends in the prevalence of chronic obstructive pulmonary disease in Korea. Tuberc Respir Dis. 2017;80(3):226–229. doi:10.4046/trd.2017.80.3.226
39. Terzikhan N, Verhamme KMC, Hofman A, et al. Prevalence and incidence of COPD in smokers and non-smokers: the Rotterdam Study. Eur J Epidemiol. 2016;31(8):785–792. doi:10.1007/s10654-016-0132-z
40. Fragoso CA. Epidemiology of chronic obstructive pulmonary disease (COPD) in aging populations. COPD. 2016;13(2):125–129. doi:10.3109/15412555.2015.1077506
41. Gershon AS, Warner L, Cascagnette P, et al. Lifetime risk of developing chronic obstructive pulmonary disease: a longitudinal population study. Lancet. 2011;378(9795):991–996. doi:10.1016/S0140-6736(11)60990-2
42. Jha P, Ramasundarahettige C, Landsman V, et al. 21st-century hazards of smoking and benefits of cessation in the United States. N Engl J Med. 2013;368(4):341–350. doi:10.1056/NEJMsa1211128
43. Cai L, Wang XM, Fan LM, et al. Socioeconomic variations in chronic obstructive pulmonary disease prevalence, diagnosis, and treatment in rural Southwest China. BMC Public Health. 2020;20(1):536. doi:10.1186/s12889-020-08687-5
44. Yin P, Jiang CQ, Cheng KK, et al. Passive smoking exposure and risk of COPD among adults in China: the Guangzhou Biobank Cohort Study. Lancet. 2007;370(9589):751–757. doi:10.1016/S0140-6736(07)61378-6
45. Hagstad S, Bjerg A, Ekerljung L, et al. Passive smoking exposure is associated with increased risk of COPD in never smokers. Chest. 2014;145(6):1298–1304. doi:10.1378/chest.13-1349
46. Terzikhan N, Verhamme KM, Hofman A, et al. Prevalence and incidence of COPD in smokers and non-smokers: the Rotterdam Study. Eur J Epidemiol. 2016;31(8):785–792. doi:10.1007/s10654-016-0132-z
47. Tang X, Lei J, Li W, et al. The relationship between BMI and lung function in populations with different characteristics: a cross-sectional study based on the enjoying breathing program in China. Int J Chron Obstruct Pulmon Dis. 2022;17:2677–2692. doi:10.2147/COPD.S378247
48. Ran PX, Wang C, Yao WZ, et al. Relationship between body mass index and chronic obstructive pulmonary disease and quality of life. Chine J Tuberculosis Respir Med. 2007;30(1):18–22.
49. Barker DJ, Godfrey KM, Fall C, et al. Relation of birth weight and childhood respiratory infection to adult lung function and death from chronic obstructive airways disease. BMJ. 1991;303(6804):671–675. doi:10.1136/bmj.303.6804.671
50. Stern DA, Morgan WJ, Wright AL, et al. Poor airway function in early infancy and lung function by age 22 years: a non-selective longitudinal cohort study. Lancet. 2007;370(9589):758–764. doi:10.1016/S0140-6736(07)61379-8
51. Menezes AM, Perez-Padilla R, Jardim JR, et al. Chronic obstructive pulmonary disease in five Latin American cities (the PLATINO study): a prevalence study. Lancet. 2005;366(9500):1875–1881. doi:10.1016/S0140-6736(05)67632-5
52. Laniado-Laborin R, Rendón A, Bauerle O. Chronic obstructive pulmonary disease case finding in Mexico in an at-risk population. Int J Tuberc Lung Dis. 2011;15(6):818–823. doi:10.5588/ijtld.10.0546
53. Xia JJ, Zou XX, Qiu Y, et al. Investigation and influencing factors analysis of chronic obstructive pulmonary disease among permanent residents aged 40 and above in Hongyuan County, Aba autonomous Prefecture, Sichuan Province. Shandong Med. 2022;63(05):51–54.
54. Guo Y, Xing Z, Shan G, et al. Prevalence and Risk Factors for COPD at High Altitude: a Large Cross-Sectional Survey of Subjects Living Between 2100-4700 m Above Sea Level. Front Med Lausanne. 2020;7:581763. doi:10.3389/fmed.2020.581763
55. Horner A, Soriano JB, Puhan MA, et al. Altitude and COPD prevalence: analysis of the PREPOCOL-PLATINO-BOLD-EPI-SCAN study. Respir Res. 2017;18(1):162. doi:10.1186/s12931-017-0643-5
56. Lin A, Mao C, Rao B, et al. Development and validation of nomogram including high altitude as a risk factor for COPD: a cross-sectional study based on Gansu population. Front Public Health. 2023;11:1127566. doi:10.3389/fpubh.2023.1127566
57. Brakema EA, Tabyshova A, Kasteleyn MJ, et al. High COPD prevalence at high altitude: does household air pollution play a role? Eur Respir J. 2019;53(2):1801193. doi:10.1183/13993003.01193-2018
留言 (0)