This retrospective study compares the clinical outcome of two three-dimensional osteosynthesis plates of different plate geometry and thickness.
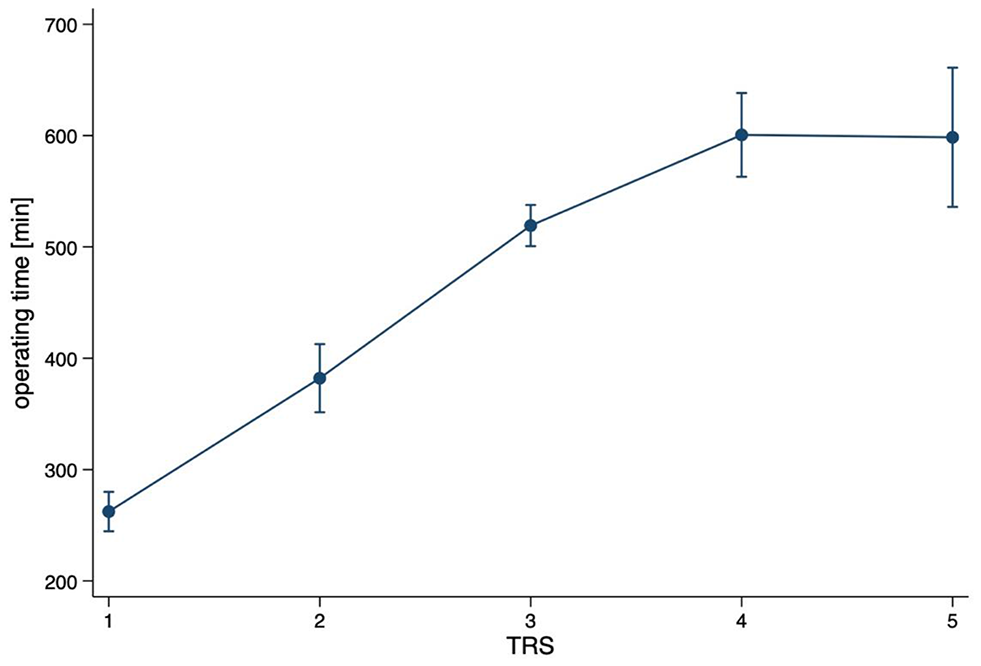
Three-dimensional plates provide the advantage of stabilizing fracture sides in a rigid manner against forces in three dimensions, including shear, bending, and torsional forces [21]. The ease of handling three-dimensional plates and their impact on surgery time remains unclear [15, 22, 23], as it may depend on various factors, such as surgeon experience, fracture pattern, plate thickness, and geometry. This study shows that plates with different designs, such as the △-plate, may be more difficult to handle, what is reflected in the longer operation times, as the bending of these plates is much more demanding. This seems to be one reason why there is a tendency in the literature to use three-dimensional plates in fractures with minimal or no displacement. Nevertheless, their use is independent of location and associated with reliable outcome prediction [24]. However, some studies have suggested the need for caution when using three-dimensional plates in mandibular angle fractures [15, 25].
Mandibular angle fractures place special demands on adequate fracture treatment due to the high tensile forces of the attaching musculature [26]. Mobile fragments, inadequate and unstable fracture reduction or malcompliance of the patient itself can be the reason for postoperative infections, non-unions and treatment failures. Therefore, the stability of the plates are seen to be crucial to keep these problems low, especially in the case of condylar head fractures [27,28,29]. However, the use of open reduction and stable internal fixation in treating angle fractures is still associated with a high complication rates, where three-dimensional plating systems are accounted for about 15–53% [25, 30,31,32].
The relatively low incidence of wound dehiscence and infection, reported in the current literature similar to the findings of this study, can be attributed to the use of careful surgical techniques and adherence to established treatment protocols, including the use of antibiotics [33]. However, some authors argue that postoperative wound infections are principally caused by fracture mobility and should be addressed by increasing fracture immobilization [15]. Even indicating an inverse relationship between the stiffness of the fixation and the occurrence of complications [34]. In comparative studies, three-dimensional plates exhibited superior performance when related to alternative methods of fixation such as a 2.0 mm plate, two 2.0 mm plates, a reconstruction plate, or MMF. This is likely due to the stability provided in three dimensions and resistance to torque and malleability. The success rate of three-dimensional plates was over 80%, except in three comparative studies [13, 22, 35].
However, it should be noted that depending on the type and localization of the fracture, the requirements for the plates and their design change [1, 6, 36].
The success of an osteosynthesis plate lies primarily in an assured fracture healing, which could not be achieved in two cases in the present study. Also in the comparative literature, non-unions were found with three-dimensional plates [13]. Of course, the surgeon’s inexperience or the patient’s characteristics, such as existing diseases or patients’ non-compliance, inadequate fracture reduction and instability can also be responsible for a non-union. Since adequate blood supply is essential for fracture healing, depending on the size of the plate to be inserted, more extensive deperiosteation has to be done, which impairs blood supply [37]. Whether this plays an additional role requires further investigation. In the two cases in this study, however, this seems unlikely, which is why another, less recognized cause must be considered, that of stress shielding.
Stress shielding is a phenomenon that occurs when the mechanical load on a bone decrease as a result of the insertion of a stiff implant. This effect has been observed in the use of rigid internal fixation plates on mandibular bone grafts. When the bone is not subjected to the normal stress and strain patterns, it can result in a reduction of bone density and weakening of the bony structure over time. This can occur due to the mechanical properties of the implant causing it to bear more of the load than the bone itself, leading to a reduction in the natural bone remodeling process. Potentially resulting in implant loosening or failure and may require revision surgery [38].
Based on the findings, plate fractures in this study only occurred after the fracture had completely healed. These plates are possibly too rigid, i.e. a combination of plate size, geometry and thickness, will suppress transmission of micromovements that could stimulate the bone. In this sense, the △-plate may have too rigid fixation in the mandibular angle region if it is too large, after which a reduction in plate size could be helpful. This study is restricted by the limited number of patients. Nevertheless, both plate designs seem to be feasible for the treatment of mandibular angle fractures, whereby the ☐-plate performed better. Further studies should address this question. In conclusion, a sufficient treatment of mandibular angle fractures is feasible by using 1.0 mm square-designed plate systems. The employment of thicker three-dimensional, triangular-designed osteosynthesis plates appears to substantially prolong the surgical duration and elevate the risk of complications.








留言 (0)