Results indicated that 12-month outcomes for retinal fluid, BVA, and CST were not significantly different between limited-early response and early response groups. However, all early response groups demonstrated significant improvement in their VA, CST, and retinal fluid volumes by 12 months relative to changes in respective limited-early response groups suggesting better anatomic and visual outcomes for the early response groups. Furthermore, the ER group showed the largest improvement in CST and BVA between baseline and 3 months after initiating injections indicating that the change in BVA and CST by 3 months is indicative of 12-month outcomes.
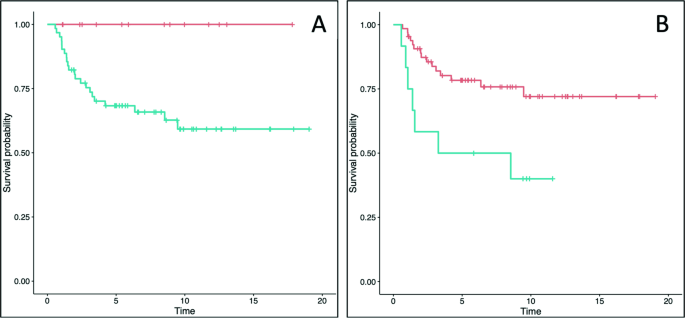
By month 12, the aLER and aER groups had significantly different outcomes relative to the other limited-early and early response groups indicating that those with limited CST reduction at 3 months after initial monthly injection had worse BVA and CST outcomes 12 months after initiating treatment. This finding is consistent with current DMO studies demonstrating a moderate correlation between worse CST and worse BVA [20, 21]. Time variance analysis and Fig. 1 demonstrates the greatest BVA change occurred within the first three months of initiating anti-VEGF injections suggesting limited BVA improvement after 3 months for all limited-early and early responders likely due to reacting to initial anti-VEGF treatment noted in Piermaci et al. study [11]. Furthermore, all early response groups had significantly higher mean ETDRS letter gain and mean CST improvement indicating that all early responders have better VA and CST outcomes 12-months after initiating treatment. Dugel et al.’s study—which categorized limited-early responders as those with ≤ 20% central retinal thickness (CRT) reduction at 12 weeks after initial anti-VEGF injection—similarly found that early responders had significantly better BVA and CRT improvement at 52 and 156 weeks [13]. The data can be explained by the floor and roof effect due to better anatomical and visual baselines in limited-early response groups in both studies. Since the limited-early response groups had better baseline values than their early response counterparts, they had limited room for improvement compared to the early responders. Further study into the effect of baseline CST and VA on LER/ER outcomes could provide more insight into their impact on long-term outcomes.
Moreover, CST and BVA change appears more gradual within the limited-early response groups relative to the rapid change seen in early response groups (Fig. 1). Time variance analysis of CST and BVA in limited-early response groups revealed significant improvement between every time point not just a very high improvement between baseline and others as noted in early response groups. This result indicates that the limited-early responders may continue to improve CST and BVA after the 12-months or remain constant. Piermaci et al.’s study found that limited-early responders continued to improve CST and BVA outcomes at about 100 weeks after initiating anti-VEGF treatment [11]. However, current long-term CST and BVA outcomes between limited-early and early responders have varied between multiple studies. Further study into CST and BVA changes past 12 months of initiating anti-VEGF in limited-early responders may clarify if this group displays a gradual change over time or a limited improvement overall.
Retinal fluid outcome findings in this study varied by fluid location. While 12-month outcomes for all retinal fluid outcomes did not vary LER status in any group, SRF 3-month outcomes marginally varied by LER status for all limited-early and early response definitions. By 3 months, all early responder groups had reduced SRF volume to around 5 nL while limited-early responders reduced to around 20 nL as shown in Table 3. This finding correlates with early responder groups showing the greatest CST reduction between baseline and 3 months. Since CST is used to assess retinal fluid and monitor macular oedema, retinal fluid reductions may mirror the CST reductions. Time variance analysis revealed vLER and LER groups showed SRF outcomes significantly varied between baseline and 12 months. The aLER demonstrated an improvement in the mean SRF volume between baseline and 12 months though not significant. Since the mean SRF volumes decrease over time in these two groups, SRF improvement may indicate gradual improvement mirroring CST outcomes and its gradual improvement noted in the respective limited-early response groups. However, the VIVID/VISTA Phase III studies found that SRF volume had decreased to nearly 0 within the first 12 weeks of treatment which is inconsistent with our findings [21]. Majority of studies have evaluated the impact of baseline SRF on DMO treatment outcomes, though not many have explored how SRF outcomes change throughout anti-VEGF treatment in DMO patients and require further study.
IRF and TRF outcomes showed significant improvement for all early response groups at month 3 but had limited improvement after while all limited-early responder groups showed no significant improvement after baseline indicating limited to no improvement. This result mimics CST and BVA outcomes in early responders showing most improvement between baseline and 3 months. This trend is consistent with studies demonstrating higher levels of IRF, SRF, and TRF correlate with worse BCVA outcomes at 12 months after initiation of anti-VEGF injections in DMO patients [17]. The relationship between retinal fluid, CST, and BVA results can be explained by the negative impact of sustained retinal fluid on the ellipsoid zone (EZ), disruption of which is directly correlated to the severity of DR [22]. Additionally, increased CST has been shown to increase the odds of EZ disruption [23]. 12-month outcomes for all retinal fluid demonstrated no affect by limited-early response status which mirrors the 12-month outcomes seen with BVA and CST. Since baseline retinal fluid values were worse for all early response groups with significant improvement compared to their respective limited-early response groups, the trend can also be attributed to the floor/ceiling effect as mentioned above, mirroring CST and BVA outcomes.
The study found no variance between the demographics and all LER definitions; however, some variance was found with the anti-VEGF injection type. Bevacizumab showed a significant difference between the aLER and aER groups indicating that bevacizumab may be associated with gradual anatomic changes in the aLER group as noted above. The Protocol T Extension study confirms this finding by demonstrating bevacizumab injections were associated with worse anatomical outcomes as compared to aflibercept and ranibizumab [24]. Additionally, ranibizumab showed significant difference between the vLER and vER groups indicating its possible impact on VA outcomes. However, no full conclusions on ranibizumab’s VA outcomes can be measured because only 2 limited-early response patients received only ranibizumab injections and no early response patients received any ranibizumab with or without the other injection types. Additionally, Protocol T did not discover worse VA outcomes with ranibizumab compared to the other injections which is inconsistent with our data [24]. Further study of anatomic and visual outcomes of DMO patients with an analysis of anti-VEGF type would clarify current findings on impact of injections on LER status.
This study contains some limitations that should be noted. Of the 220 patients collected in the retrospective analysis, most participants identified as White and Not Hispanic. With significantly smaller groups in other races and ethnicities, no conclusions could be drawn on limited-early/early response status relative to these baseline characteristics. Furthermore, no demographic baseline characteristics were statistically significant between groups, which allowed us to assess data while controlling for factors but may not be representative of all DMO patients. Future studies should investigate the possible effect of baseline characteristics and demographics on limited-early response status. Furthermore, while our analysis revealed the impact of the floor and ceiling effects on all limited early response groups due to better VA and CST at baseline, further study into LER patients with worse baseline CST and VA values may indicate demographic characteristics that affect LER status. No data following the 12-month outcome was available for analysis, therefore, analysis of long-term outcomes past 1 year cannot be concluded. Additionally, the data from OCTs are from the NOA and anatomic characteristics such as disorganization of retinal inner layers were not used and thus no analysis was done. Another subject of note is the unequal sizes of the LER and ER populations. This study found 162 patients (73.6%) classified as limited early responders, whereas most studies reported 40–50% LER, such as Piermaci et al. with 43.5%, 14.8%, and 11.5% of each group satisfied the limited early responder criteria [11]. The variation may be accounted for by the differing study inclusion and exclusion criteria such as Piermaci et al. only including patients with CST values ≥ 300 μm at baseline [11]. As a result, the mean baseline CST is higher for both the limited-early and early responders in Piermaci et al.’s study, and therefore, the smaller percentage of limited-early responders is likely due to the floor effect. Our analysis has accounted for the significant variance in population size, but the large difference in two groups should be noted.
Altogether, all ER groups showed significant improvement in CST, BVA, retinal fluids between baseline and 3 months and remained relatively constant to 12 months while all LER groups showed limited improvement between baseline and 3 months and gradually improved by 12 months. These results indicate that limited-early/early response status determined at 3 months after initiating anti-VEGF treatment can predict long-term outcomes. Baseline CST, BVA, and retinal fluid in LER groups may explain the limited improvement relative to ER groups due to the floor/ceiling effect. Furthermore, EZ disruption is negatively affected by CST and retinal fluids which helps explain the BVA outcomes. These conclusions will help physicians understand and utilize trends in retinal fluid, VA, and CST in limited-early and early responders for DMO treatment. Further studies exploring the effect of SRF throughout DMO treatment period and analysis of long-term outcomes beyond 12-months are necessary to draw further conclusions to the findings.
What was known before
Patients with diabetic macular oedema have various treatment response to anti-VEGF injections. Current studies demonstrate that the treatment response can be characterized as limited-early or early response at 3 months in regard to CST and VA improvement at this time point. Some studies have also explored the impact of the limited-early and early responders on long-term treatment outcomes, but requires additional studies.
What this study adds
This study investigates the impact of intraretinal, subretinal, and total retinal fluid on limited-early response status to determine the role of fluid in DMO. Additionally, the study divides the groups into anatomical (CST) and visual (VA) limited-early responders to determine additional factors that may affect their treatment outcome and the effect of their status on long-term outcomes.




留言 (0)