
記住我






Endovascular therapy (EVT) is the current standard treatment in patients with acute ischemic stroke and large vessel occlusion (LVO).1 2 In the HERMES meta-analysis, approximately one in five of the study patients were treated for an occlusion of the internal carotid artery (ICA).3 However, ICA occlusions are not a homogeneous group. They can be distinguished as (1) ICA-T occlusions—that is, thrombi extending from the ICA to the middle cerebral artery and anterior cerebral artery and (2) ICA occlusions with patent carotid-T.4 5 In the studies contributing to HERMES, most individuals had an ICA-T occlusion.3 Impeding collateral flow through the circle of Willis, ICA-T occlusions have been associated with a poor outcome in comparison with isolated, further proximal ICA occlusions, in previous observational thrombectomy studies.6 7 In contrast, an occlusion pattern with patent carotid-T seems to be associated with better clinical outcomes after EVT in comparison with ICA-T occlusions.4–6 To date, there are no randomized controlled trials (RCTs) proving efficacy or safety of EVT in patients with isolated, non-tandem ICA occlusion and open carotid-T. Herein, we aimed to characterize these patients by comparing them with patients suffering from ICA-T occlusion.
MethodsStudy populationPatients were identified from the German Stroke Registry (GSR), a national, prospective, multicenter observational registry that has been described previously.8 The GSR includes all individuals admitted to its participating centers with LVO, aged ≥18 years, in whom EVT is initiated. A systematic follow-up of functional status/degree of disability 3 months after stroke via the modified Rankin Scale (mRS) is regularly performed.
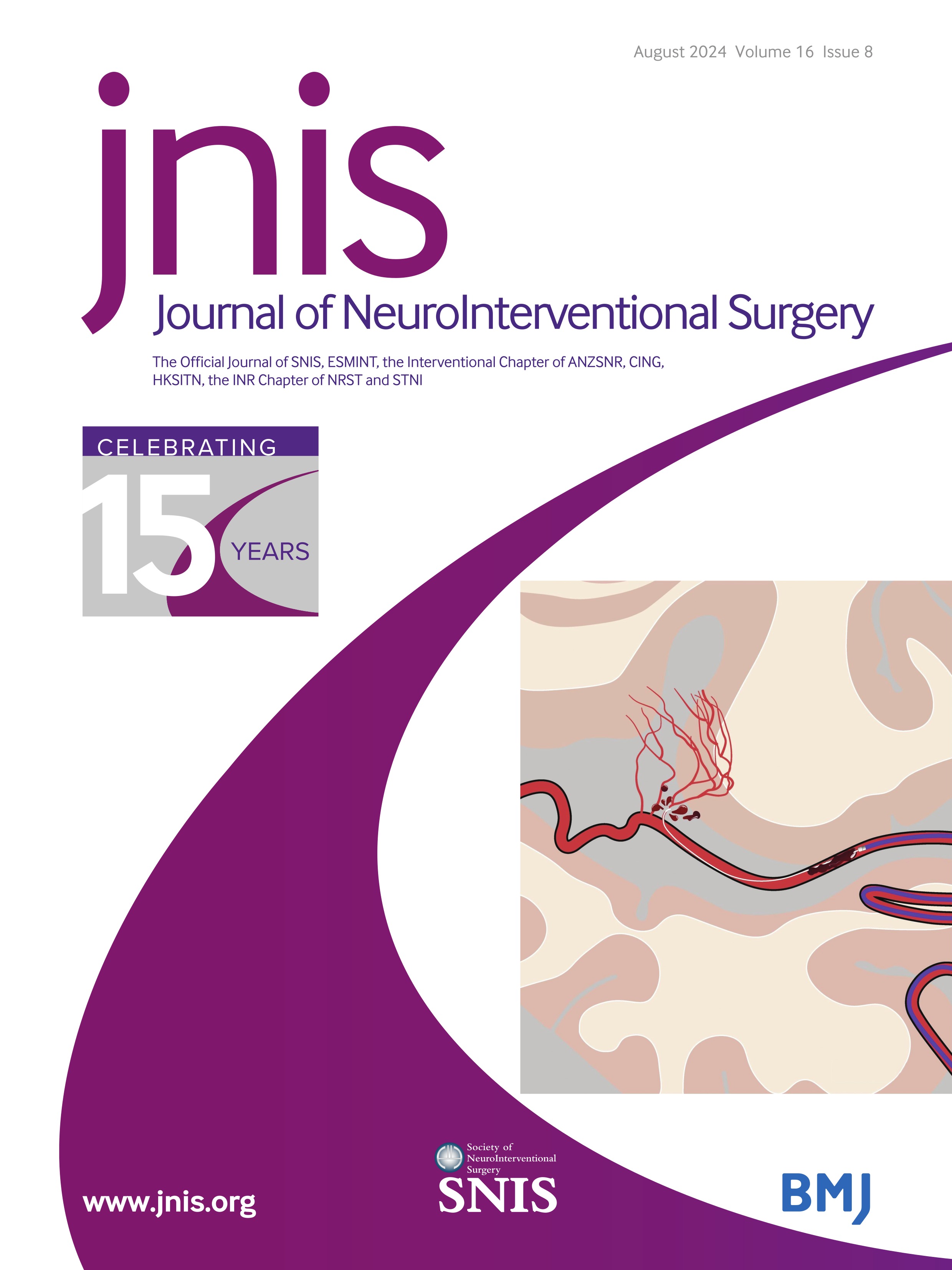
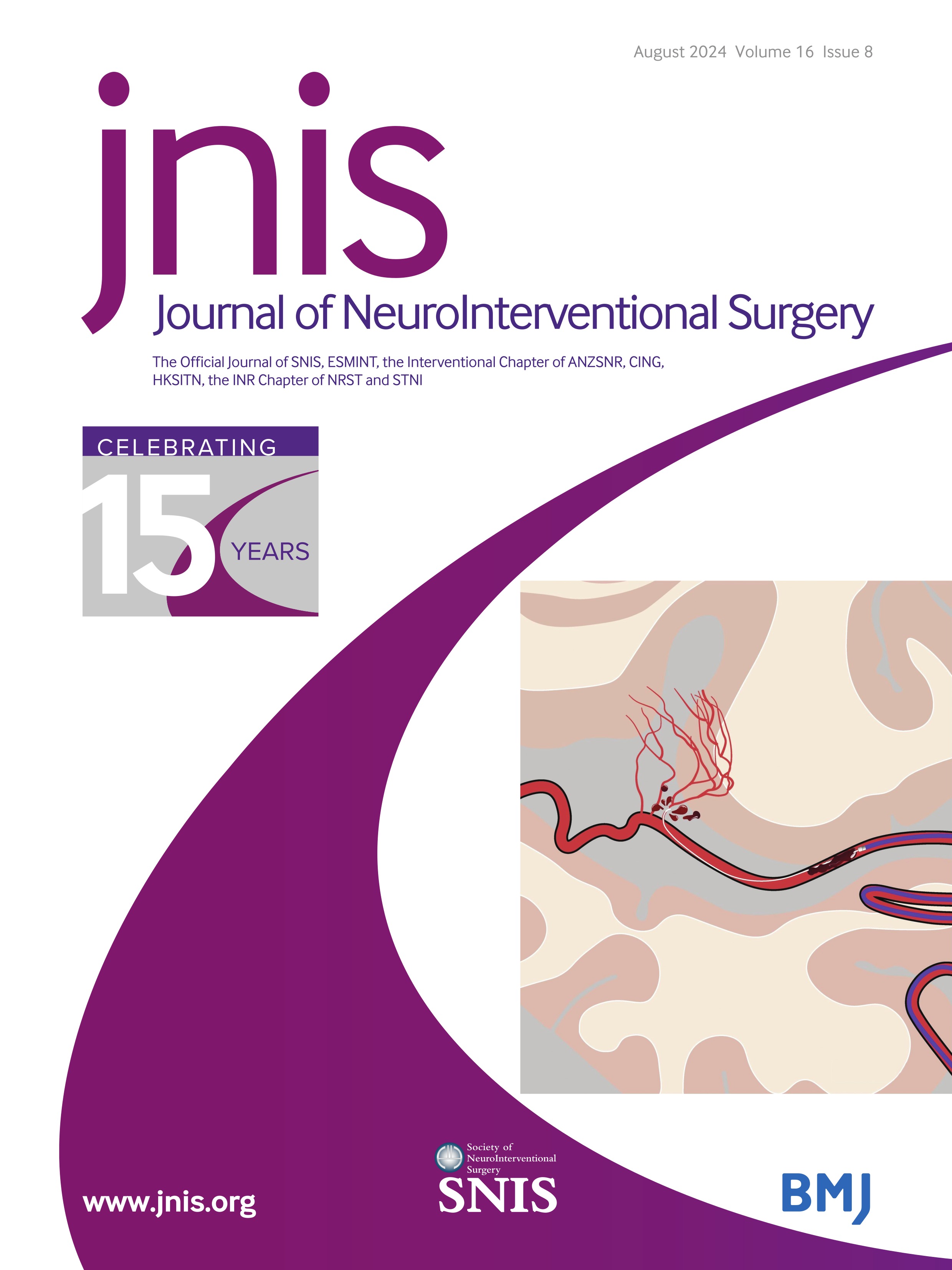
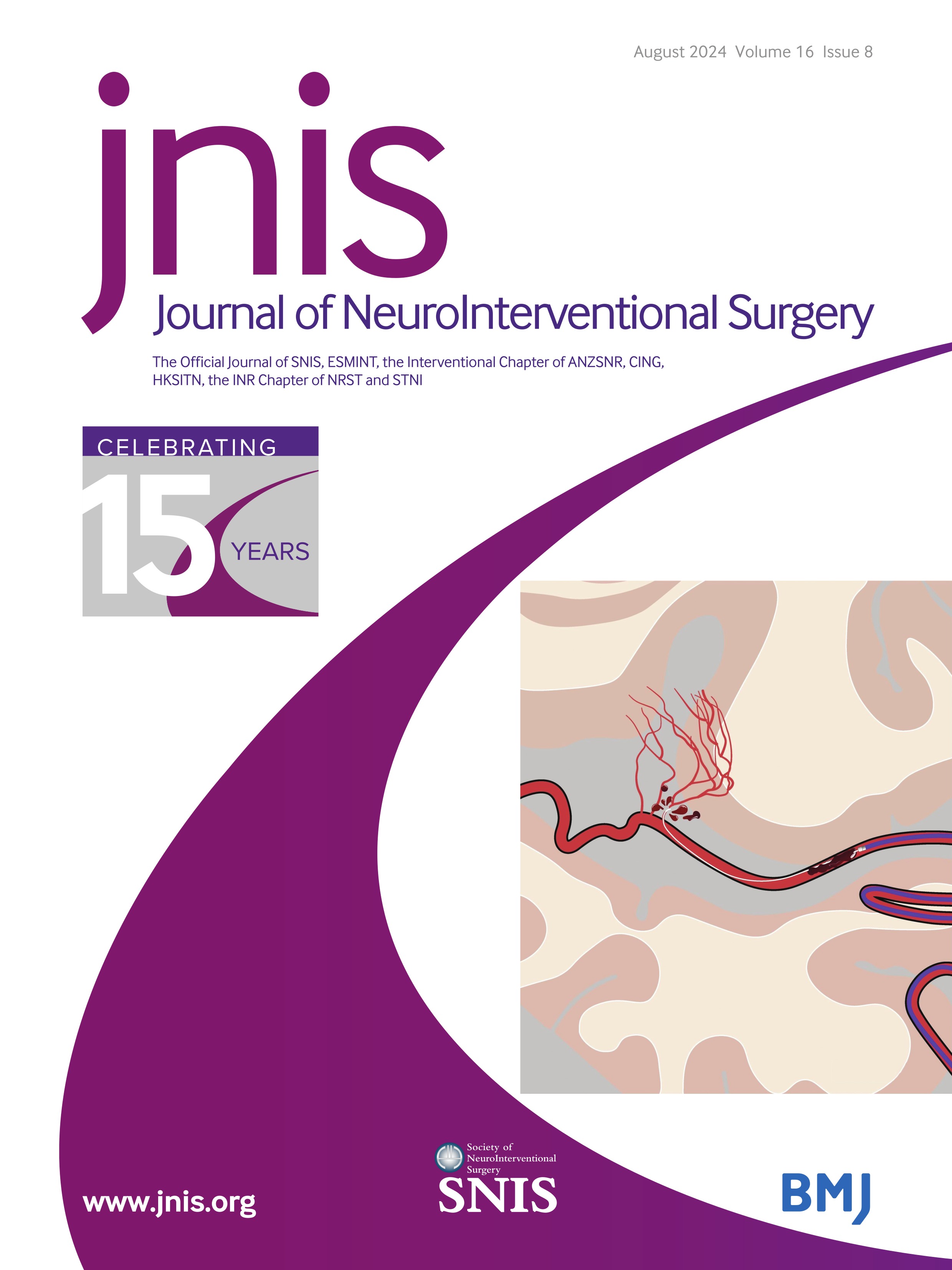
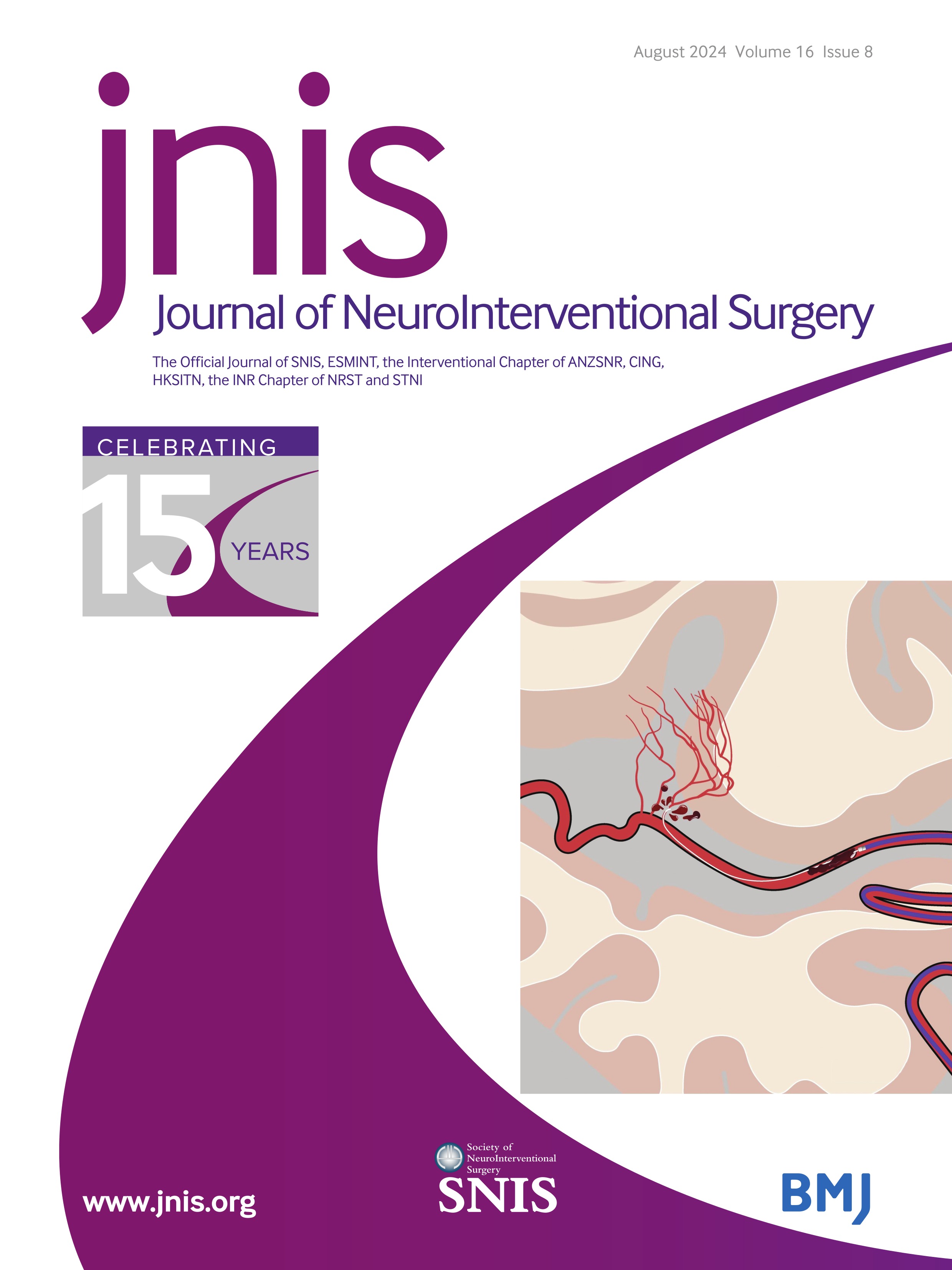
We identified all patients in the registry who were treated for an ICA occlusion between June 2015 and December 2021. In the GSR database the occlusion pattern was classified, based on the most proximal visible thrombus on CT angiography or MR angiography and patency of the circle of Willis (figure 1), as documented in routine clinical data of each participating center. Whenever the exact occlusion site was not documented in the center’s routine medical findings (ie, ‘occlusion of the carotid artery’), local board-certified neuroradiologists reassessed source imaging data and classified the patient’s exact occlusion site.
The study sample was divided into three groups of patients—namely, ICA-T occlusion (with or without occlusion of further proximal ICA segments), ICA-I occlusion (intracranial ICA occlusion with patent extracranial ICA and patent carotid-T), and ICA-E occlusion (extracranial ICA without occlusion of the ipsilateral carotid-T). Patients with multiple or tandem occlusions (ie, ICA occlusions with documented additional blockage in any segment of the middle or anterior cerebral artery or vertebrobasilar circulation) were excluded from the analysis. For the three groups of patients, we compared baseline variables, differences in treatment modality, procedure times, technical and functional outcomes.
 Figure 1
Figure 1 Occlusion patterns of the internal carotid artery. ACA, anterior cerebral artery; AChA, anterior choroidal artery; ICA-E, occlusion of the extracranial segment of the internal carotid artery; ICA-I, occlusion of the non-terminal internal segment of the internal carotid artery; ICA-T, occlusion of the terminal segment of the internal carotid artery (involving the proximal segments of the ACA and MCA); MCA, middle cerebral artery; OphtA, ophthalmic artery; PComA, posterior communicating artery.
VariablesStroke severity was assessed using the National Institutes of Health Stroke Scale (NIHSS). The mRS score 3 months after the index event served as primary clinical outcome. As secondary clinical outcomes, we chose early neurological improvement (that is, improvement of at least 4 points on the NIHSS or reaching a NIHSS score of 0 points 24 hours after admission) and early neurological deterioration (that is, worsening of at least 4 points on the NIHSS 24 hours after admission). Technical success of the EVT was assessed using the modified Thrombolysis in Cerebral Infarction scale (mTICI) at the end of the procedure. We analyzed clot migration/embolization as well as dissection/perforation of cerebral vessels as treatment adverse events. As safety variables, we chose in-hospital death, death within 3 months after stroke, any intracranial hemorrhage (ICH) and symptomatic ICH (that is, ICH with NIHSS score worsening of ≥4 points).
Statistical analysisContinuous baseline variables and treatment times are presented as median (IQR), dichotomous variables as absolute numbers and percentage. Comparisons of the distribution between groups were performed by the Kruskal-Wallis test (P)/Jonckheere-Terpstra test (P for trend) for linear and ordinal variables, and Χ2 test (P)/Cochran-Armitage test (P for trend) for dichotomous variables.9 10 Binary logistic regression analyses were conducted to assess the impact of occlusion site on clinical and technical outcomes. ORs for clinical and safety outcomes were adjusted for age, sex, stroke severity (NIHSS score at admission), intravenous thrombolysis, pre-event dependency (mRS score pre-stroke), witnessed onset of stroke symptoms, and Alberta Stroke Program Early CT Score (ASPECTS). Anticoagulation (use of dabigatran, rivaroxaban, edoxaban, apixaban, heparin (therapeutic dose), warfarin) was included in the model for ICH and symptomatic ICH only.
For technical outcomes and treatment adverse events, adjustments were made for stroke etiology (large artery atherosclerosis (LAA) vs other etiologies) and thrombolysis status. Functional disability at 3 months was calculated by ordinal regression (mRS score shift), adjusting for the above-mentioned factors. Since less than 60% of the study patients presented with a witnessed onset of stroke, symptom onset to groin puncture was not included in the main multivariable analyses. However, to adjust for possible imbalances in time to treatment between different ICA occlusion sites, we conducted a sensitivity analysis in which we replaced the variable witnessed onset of stroke symptoms by a proxy variable called time to endovascular treatment (time to EVT), which was calculated as follows: For patients with witnessed onset of symptoms, the time from symptom onset to groin puncture was used as time to EVT. For unwitnessed onset stroke, we followed a suggestion of the EXTEND investigators and considered the time of onset to be the midpoint between last seen well and time of recognition.11 All analyses were conducted using IBM SPSS Statistics for Windows, version 28.0.0.0, (Armonk, New York, USA: IBM Corp).
Informed consent and ethics approvalThe GSR was centrally approved by the ethics committee of the Ludwig-Maximilians University, Munich (689-15) as the lead ethics committee.8 Informed consent was not mandatory in accordance with local rules and regulations. Data sampling from patients undergoing EVT is mandated by federal law. Thus, selection bias through lack of informed consent could be minimized.12
ResultsBetween June 2015 and December 2021, 13 082 patients were included in the GSR and 2588 (19.8%) of them presented with an isolated ICA occlusion. Of these, 1946 patients (75.2%) had an ICA-T occlusion, 366 patients (14.1%) an ICA-I occlusion, and 276 patients (10.7%) an ICA-E occlusion. There were differences between patients with ICA-T, ICA-I, and ICA-E occlusion in age (77 (66–83) vs 76 (65–82) vs 74 (63–82) years, Ptrend=0.02), sex (female: 53.4% vs 48.9% vs 43.1%, Ptrend<0.001), and functional independence before the index event (pre-stroke mRS score ≤2: 80.4% vs 85.7% vs 86.3%, Ptrend=0.04), respectively. Patients differed in stroke severity (NIHSS score at admission: 17 (13–20) vs 14 (9–19) vs 13 (8–18) points, Ptrend<0.001), and frequency of vascular risk factors. In concordance with the observed distribution of vascular risk factors, diagnosed LAA stroke etiology was lowest in ICA-T and highest in ICA-E occlusions (30.4 vs 34.4 vs 45.7%, P<0.001, respectively). There was no difference in the rates of a witnessed onset of stroke, and about 40% of all three groups were transferred to EVT centers from external hospitals. Other baseline demographics are presented in table 1.
Table 1Baseline variables, stroke etiology, and treatment procedures
Differences were seen in imaging modality, baseline ASPECTS, time-to-care metrics, and modality of anesthesia. Although, the rate of MRI as initial imaging was low in general (<5%), it was more frequent in patients with ICA-I occlusion (6.4%) than in patients with ICA-T and ICA-E occlusions (3.1% and 3.8%, respectively; P<0.01. Rates of perfusion-based imaging (CTP/MRP) were lowest in ICA-T occlusion (48.9%), mid-range in ICA-I occlusion (53.5%) and highest in ICA-E occlusion patients (64.2%), (Ptrend<0.001). ASPECTS was lowest in patients with ICA-T occlusion (8 (7–10) vs 9 (8–10) vs 9 (8–10) points, Ptrend<0.001). Time between symptom onset and arrival at the interventional hospital differed between the three groups with ICA-T occlusion patients having the shortest prehospital delay (120 (60–200) vs 150 (65–213) vs 156 (67–243) minutes, Ptrend<0.001). Time between arrival and groin puncture differed, with ICA-T patients having the shortest delay (67 (45–95) vs 81 (54–130) vs 75 (47–111) minutes, Ptrend<0.001). The rate of bridging thrombolysis was highest in patients with ICA-T and lowest in patients with ICA-E occlusion (46.9% vs 42.9% vs 41.3%, Ptrend=0.04). In comparison with ICA-T and ICA-I occlusion, door-to-needle times were slightly longer in patients with ICA-E occlusion (29 (21–40) vs 29 (23–46) vs 33 (24–49) minutes, respectively, Ptrend=0.02). Use of general anesthesia differed with patients with ICA-E showing lowest general anesthesia rates (78.3% (ICA-T) vs 80.6% (ICA-I) vs 68.0% (ICA-E), p<0.001). The time from groin to reperfusion did not differ between groups (about 50 min for ICA-T, ICA-I, and ICA-E occlusions, P=0.88). An ICA-stent was deployed in one of four patients with ICA-T and ICA-I occlusion, but in every other patient with ICA-E occlusion (24.3% vs 24.9% vs 48.9%, ptrend<0.001). All procedural variables and treatment times are depicted in table 1.
In comparison with ICA-T occlusions, the rate of successful recanalization (TICI 2b/3) was lower in patients with ICA-I or ICA-E occlusion (85.4% vs 80.4% vs 76.3%; aOR (95% CI) for ICA-I vs ICA-T 0.71 (0.53 to 0.95), p=0.02; aOR (95% CI) for ICA-E vs ICA-T 0.57 (0.42 to 0.78), p<0.001). After adjusting for confounders, ICA-E occlusions had a higher odds for in-hospital death (aOR=1.94 (1.37 to 2.74), p<0.001), death at 90 days (1.59 (1.11 to 2.28), p=0.01), early neurological deterioration (aOR=1.70 (1.23 to 2.36), p<0.01), and clot migration/embolization during endovascular treatment (aOR=2.44 (1.55 to 3.92), p<0.001) than ICA-T occlusions. The rates of any ICH or symptomatic ICH did not differ between groups. Despite a numerically higher rate of patients with good clinical outcome (mRS score ≤2), an ICA-I occlusion pattern (vs ICA-T) was not associated with reduced disability in adjusted logistic, or ordinal regression analysis (adjusted cOR mRS shift: 0.95 (0.74 to 1.22), p=0.70). For ICA-E occlusions, however, an adjusted mRS shift analysis showed worse clinical outcome in comparison with patients with ICA-T occlusion (adjusted cOR=0.70 (0.52 to 0.93), p<0.01). All clinical and technical outcomes are presented in table 2. The distribution of mRS scores 3 months after stroke for each ICA occlusion site is depicted in figure 2.
 Figure 2
Figure 2 Distribution of clinical outcome 3 months after stroke stratified by internal carotid artery occlusion pattern. ICA-E, occlusion of the extracranial segment of the internal carotid artery; ICA-I, occlusion of the non-terminal internal segment of the internal carotid artery; ICA-T, occlusion of the terminal segment of the internal carotid artery (involving the proximal segments of the anterior cerebral artery and middle cerebral artery).
Table 2Clinical, technical, and safety outcomes
All results for outcomes proved to be robust in a sensitivity analysis including time to endovascular treatment (for details, see online supplemental file 1).
DiscussionIn our study, we found that patients with ICA occlusion and patent intracranial vessels differ from patients with ICA-T occlusion in several aspects, including baseline factors, procedural variables, technical, and functional outcomes. First, differences are evident with respect to age, sex, stroke severity, and stroke etiology. Patients with ICA-E occlusion were youngest, most often male, least severely affected and were diagnosed with the highest rate of LAA as stroke etiology. Second, we found differences in time-to-care metrics with longer treatment delay in patients with ICA-I and ICA-E occlusions. Third, patients with ICA-E occlusion had lower odds for successful recanalization and higher odds for early neurological deterioration as well as in-hospital mortality. Most importantly, after adjustment for baseline variables, ICA-E occlusion site was associated with worse clinical outcome 3 months after stroke.
PrevalenceIn the HERMES meta-analysis, 21% of patients were treated for an ICA occlusion.3 However, in two of the five RCTs contributing to this meta-analysis, the prevalence of ICA-I occlusions was very low (0.8% in MR CLEAN, 0.5% in REVASCAT).13 14 Two other trials did not distinguish between ICA-T and ICA-I occlusion (SWIFT-PRIME, EXTEND-IA)15 16 and the fifth trial (ESCAPE)17 did not include patients with an ICA-I occlusion pattern. Patients with isolated ICA-E occlusion did not fulfill the inclusion criteria of any of the above-mentioned RCTs.13–17 Nevertheless, in real-life practice, individuals with ICA occlusion and patent intracranial vessels represent a relevant group of patients with LVO stroke. About 1 in 20 patients undergoing EVT in the GSR had an ICA-non-T occlusion pattern (2.8% ICA-I and 2.1% ICA-E). In the Society of Vascular and Interventional Neurology prospective registry in the United States, 2.5% of patients with LVO were treated for an isolated extracranial ICA occlusion.18 In an Italian multicenter registry, 7.8% of the patients undergoing EVT were treated for an ICA-I (with or without ICA-E) occlusion.19 On the other hand, in a Dutch multicenter registry only 1.0% of EVT-treated patients had an ICA-I occlusion.4 This heterogeneity across different countries may be seen as a proxy for the current lack of evidence, leading to individual, rather than, guideline-based treatment decisions.
Time-to-care metricsOf interest, we found longer times from symptom onset to arrival at the thrombectomy center in patients with ICA-I and ICA-E occlusion. Possible reasons may be intact collateralization over the circle of Willis, resulting in less severe stroke symptoms, stuttering symptom progression, or symptom fluctuation. Treatment delay, however, was present in the prehospital phase, and also after hospital arrival with significantly longer door-to-groin times in patients with ICA-I and ICA-E occlusion. Similar observations on treatment times have been described in the MR CLEAN registry.4 In patients with ICA-I occlusion, the higher rate of MRI diagnostics might have contributed to the longer treatment times. On the other hand, longer treatment times might also reflect uncertainty about the best therapeutic approach and underscore the need for guiding data.
In ICA-non-T occlusion patients, we found a twofold (ICA-E) or even threefold (ICA-I) higher rate of patients with a door-to-groin time of more than 3 hours. In some of these cases technical or logistical problems might explain the delay, but it can be hypothesized that a substantial number of patients might have been assigned to a first-line conservative approach. Patients with ICA-E and ICA-I occlusion might then have experienced hemodynamic instability or thrombus migration, leading to clinical deterioration and a decision for rescue thrombectomy. In patients with ICA-I and ICA-E occlusions, a relatively high rate of thrombus migration has been described previously.20 In most of these patients, thrombus migration occurred relatively late during stroke unit monitoring after a conservative treatment regimen had been conducted initially.20 The high rate of early neurological deterioration that we report for patients with ICA-E in our study may support this notion.
Technical outcomeWe found lower rates of successful recanalization (TICI 2b/3) in patients with ICA-I (80%) as well as ICA-E (76%) occlusions both in comparison with ICA-T (85%). These results are concordant with data from the Italian registry IRETAS, which reported TICI 2b/3 in only 75% of all patients with ICA-I occlusions.19 Even in the MR CLEAN Registry, the rate of successful recanalization was lower in patients with ICA-I (56%) than in the whole registry (62%).4 However, a comparison of absolute recanalization rates is limited by the fact that MR CLEAN and IRETAS report patient data from 2015 to 2018 and from 2010 to 2017, respectively. Rates of successful recanalization were lower during these years, and EVT has since seen improvements in technique and devices.4 19
The higher rates of failed recanalization for ICA-I and ICA-E occlusions in our study are most probably due to the higher prevalence of LAA stroke etiology (ie, intracranial and extracranial ICA stenosis). LAA etiology is associated with high rates of early reocclusion as well as unsuccessful passage of an ICA stenosis/occlusion.21 With LAA as the predominant etiology in patients with ICA-E occlusion, lower rates of TICI 2b/3 can be expected with regard to previously published evidence on the effects of stroke etiology on technical thrombectomy outcomes.22 Moreover, the high rates of periprocedural clot migration and embolization in patients with ICA-E (9.4% vs 4.3% in ICA-T) might have added to this finding. Our results are corroborated by a multicenter analysis from the French ETIS Registry, which also reported high rates of periprocedural complications such as intracranial embolism in patients receiving EVT for isolated ICA-E occlusion.23 Here, recanalization was successful in 82% at the end of the procedure but declined to 70% in control imaging after 24 hours.23 Similar to our study, about half of the patients received stenting in the ETIS Registry.23
Clinical outcomeFor clinical endpoints, we found no significant differences between ICA-I and ICA-T occlusion patterns in adjusted analyses. This is surprising, since the preserved collateral flow across the anterior communicating artery would be expected to lower infarct volume and increase the odds for better clinical outcome, which was reported in a study on ICA occlusion patterns in 2015.5 We propose two possible reasons for this discrepancy: first, we suppose a selection bias, since a substantial number of patients with ICA-I occlusion and persistent, stable collateralization might not have received EVT because of minor symptoms or stable clinical course, and these patients were not covered by our registry. Second, more than 10% of patients with ICA-I and ICA-E occlusion received EVT more than 3 hours after hospital arrival, probably due to worsening of clinical symptoms. This deterioration might not have been detected early, but rather after a substantial delay, resulting in increased infarct cores, death, and disability. In patients with isolated cervical or intracranial ICA occlusion with patent circle of Willis, early neurological deterioration has been reported to occur in up to 30% of patients.24 In a large cohort study aiming to predict early neurological deterioration in patients with minor stroke, which excluded patients with isolated ICA-non-T occlusion, the incidence of early neurological deterioration was about 13%25 This discrepancy—together with our data—shows that patients with isolated non-terminal ICA occlusion should be closely monitored and rescue thrombectomy should be considered in cases of early neurological deterioration.
Most interestingly, an ICA-E occlusion pattern, was associated with worse clinical outcomes after adjusting for baseline parameters, both during the acute hospital stay and in the follow-up period. Despite a younger age, lower stroke severity at admission, and less pre-stroke disability, the absolute rates of death and disability 3 months after stroke were very similar in patients with ICA-E in comparison with those with ICA-T. Supporting this notion, tandem lesions (ie, simultaneous occlusion or stenosis of the extracranial ICA and intracranial vessels) were an independent predictor of poor clinical outcome in patients with LVO stroke in a study from the pre-thrombectomy era.26 However, a more recent subgroup analysis of the ESCAPE-NA-1 trial found no significant differences in clinical outcomes when comparing EVT-treated patients with tandem carotid occlusions with patients with non-tandem intracranial LVO.27
Several registry studies on the optimal management of LVO with tandem lesion have been published,28 29 but evidence on the treatment of isolated extracranial ICA occlusions remains scarce.30 31 To our knowledge, only one large retrospective multicenter case–control study on cervical ICA occlusions has been published—the ICARO-3 study, which did not find an association of EVT with better clinical outcome when compared with intravenous thrombolysis.32 Considering that ICARO-3 reports data from patients with ICA-E occlusion treated between 2010 and 2013, it becomes evident that further trials are needed to assess the safety and efficacy of EVT in this population.
It is of note, that in our study, patients with ICA-E had a higher rate of in-hospital mortality than patients with ICA-T –despite being substantially younger. Possibly, the high rates of early neurological deterioration might have affected physicians’ and relatives’ decision about therapy limitations and thus indirectly influenced mortality rates.
LimitationsThis is an analysis of a large multicenter population allowing adjustment for confounders. Nevertheless, limitations have to be considered. Selection bias applies because patients not undergoing EVT were not included in the GSR. Consequently, decisions on whether, or under which circumstances, EVT should be performed in ICA-I or ICA-E occlusions cannot be deduced from our data.
The GSR does not hold a central imaging database. Thus, we were not able to reassess all source imaging of patients with ICA-I and ICA-E for signs of carotid pseudo-occlusion, such as gradual contrast decline.33 34 This might have led to some patients in the ICA-I and ICA-E group being misclassified, potentially limiting our results. In the GSR, there is no standardized assessment of patency of the anterior choroidal artery or anatomical configuration of the circle of Willis relevant to collateral capacity. Clot burden scores were not recorded. Given that periprocedural clot migration occurred in nearly every tenth of our study patients with ICA-E, a large clot burden could be of high relevance for both clinical and technical outcomes regarding EVT in patients with ICA-E occlusion and might have influenced our study results. With patent circle of Willis in ICA-I and ICA-E occlusion patterns, collateral capacity may be of major prognostic relevance. However, we did not gather data on collateral scores, which limits our findings. While all large and medium vessel occlusions (up to middle cerebral artery M2 segment) are documented in the GSR, we cannot exclude the possibility that some of the patients with ICA-I and ICA-E had small distal branch occlusions, potentially influencing clinical and technical outcomes. Clear discrimination between acute and chronic ICA-E occlusion is a frequent challenge in the emergency setting. Only 3.8% of the patients with ICA-E in our study had MRI as initial imaging modality, but more than 60% received CT perfusion, which contributed to the treatment decision. However, assessment of acuteness of ICA-E occlusion and exact mediating mechanism remain an inherent challenge in these patients.
留言 (0)