
記住我








In this prospective, parallel two-armed randomized controlled study, we compared the standard coagulation tests and thromboelastography parameters, postoperative waking time, and shivering occurrence in active vs. passive cutaneous warming patients with the core body temperature as the primary endpoint. It was an open-label study due to the nature of intervention. To be eligible for enrollment, patients must be ≥ 18 years of age, scheduled for elective radical resection of pulmonary cancer/esophagus cancer (operation duration > 2 h), and with core body temperature between 36 and 37.5 ℃ prior to surgeries. Exclusion criteria included the following: patients under 18 years of age, hemoglobin level (HB) ≤ 10.0 g/dl, platelet count < 100 × 109/l or > 400 × 109/l, prothrombin time (PT) prolongation > 3 s, activated partial thromboplastin time (APTT) prolongation > 10 s, international normalized ratio (INR) > 1.5, history of thyroid dysfunction, coagulopathy, intake of anticoagulants/NSAIDs within 14 days prior to surgery, or fever with infectious causes in the preceding 4 weeks. Demographic data and clinical data were prospectively collected since enrollment.
Enrolled patients were randomized into the passive cutaneous warming system (Control) and active cutaneous warming systems (Intervention) groups. Randomized numbers were generated by SAS 9.0 (SAS Institute, Cary, NC, USA) and sealed in envelopes. Anesthesia was induced by intravenous infusion of 1–2 mg/kg of propofol, 0.25–0.3 µg of sufentanil, and 0.6 mg/kg of rocuronium and was maintained by continuous intravenous infusion of 3–6 mg/kg/h of propofol, 0.1–0.3 µg/kg/min of remifentanil, and 0.75–0.1 mg/kg of rocuronium. Bispectral index (BIS) level was monitored between 40 and 60 during the surgeries. Patients in the Control group were intraoperatively covered with unwarmed surgical draping, while patients in the Intervention group were preoperatively and intraoperatively warmed to 37.5 °C core body temperature with the Bair Hugger warming unit (Bair-Hugger Patient Warmer, 3 M, St. Paul, MN, USA) (Alparslan et al. 2018). Tympanic membrane temperature was measured as core temperature at 5 min (min) before anesthesia induction (T1). Nasopharyngeal temperature was measured as core temperature 1 h after operation initiation (T2) and until the completion of surgery (T3). Once a core temperature below 36 °C was detected in the Control group, a forced-air patient warming system (WarmTouch Patient Warming System, Covidien LLC, USA) would be applied as rescue remedy, to restore the core temperature above 36 °C. One heparin-free arterial catheter was inserted into a radial artery for invasive blood pressure monitoring and blood sampling in each patient.
This study was approved by the scientific ethical committee of Peking Union Medical College Hospital (PUMCH) and registered at ClinicalTrials.gov (NCT03878901). Written informed consent was obtained from all patients before enrollment.
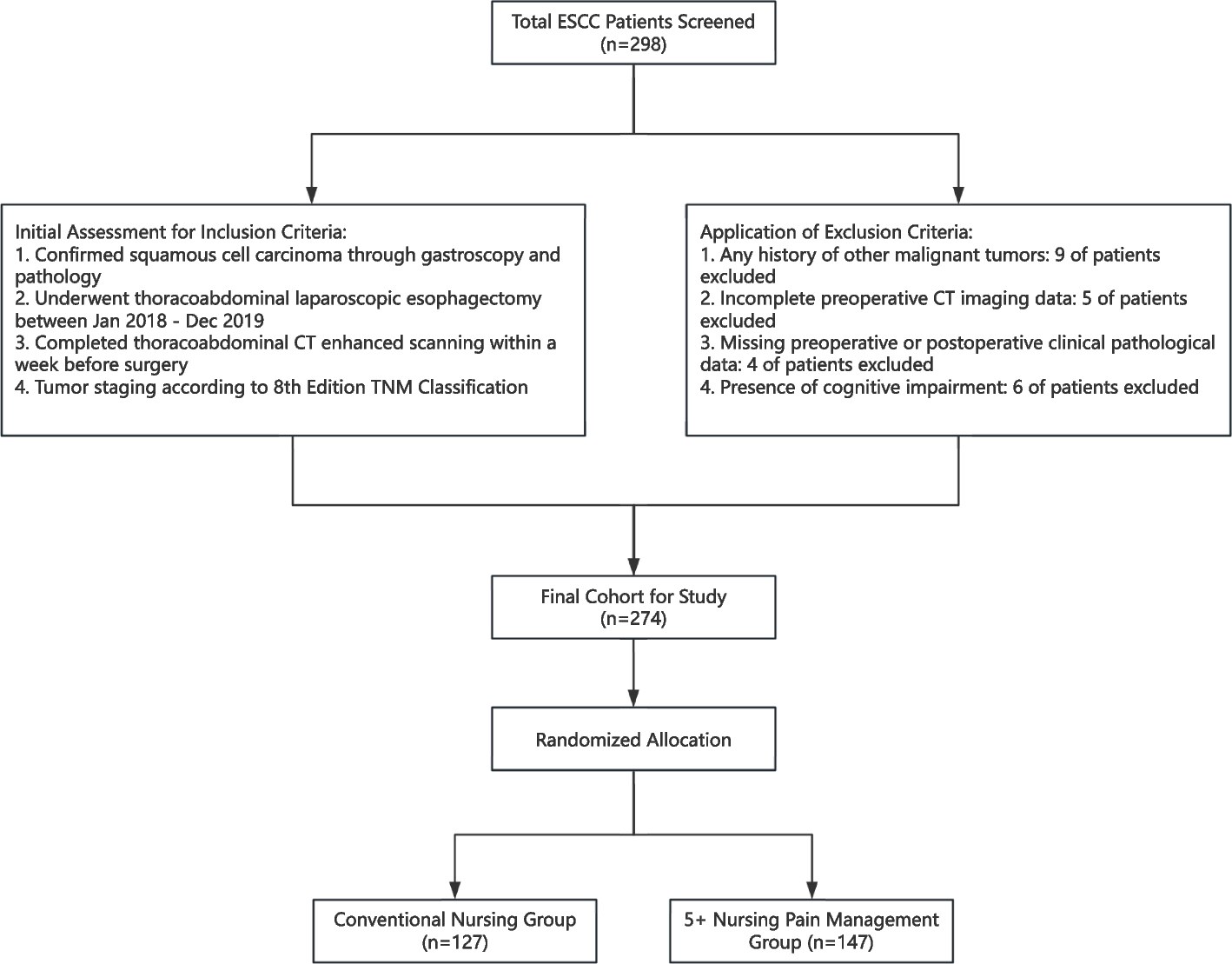
Standard coagulation testsBaseline coagulation function was examined using standard tests at enrollment. At surgical closure, 4 ml (ml) of arterial blood samples was collected in silicone-coated tubes containing 0.129-M buffered sodium citrate and sent for examination at the institutional lab. Five quantitative measures (PT, APTT, INR, FBG, PLT count) were recorded and compared between the two groups (Fig. 1).
Fig. 1
Flow diagram of the trial progress through the phases of enrollment, intervention allocation, and data analysis
ThromboelastographyCoagulation functions at baseline and surgical closure were tested using TEG. Two temperature-adaptable TEGs® were used in this investigation. One was adjusted to 37 °C, while the other was adjusted to the actual core body temperature measured in the Control group. The temperature accuracy was verified by measuring the temperature of the thromboelastography cuvettes filled with normal saline and was within a deviation of ± 0.2 °C. Measurements were performed with disposable plastic pins and cups (Haemoscope), inserted at least 20 min before measurements to confirm the exact temperature of the cup. Immediately after sample extractions, 360-µl blood samples from the Intervention group were tested at 37 °C. Dual 360-µl samples from the Control group were concurrently tested at 37 °C and adjusted temperatures.
Statistical analysesStandard coagulation tests, TEG parameters, and waking time after anesthesia were presented as mean ± standard deviation (SD) and compared between groups using one-way ANOVA analysis. Incidence of postoperative shivering was enumerated and compared between groups using the chi-square test. Statistical analyses were performed using SPSS 19.0 software, and a p-value ≤ 0.05 was considered statistically significant.
留言 (0)