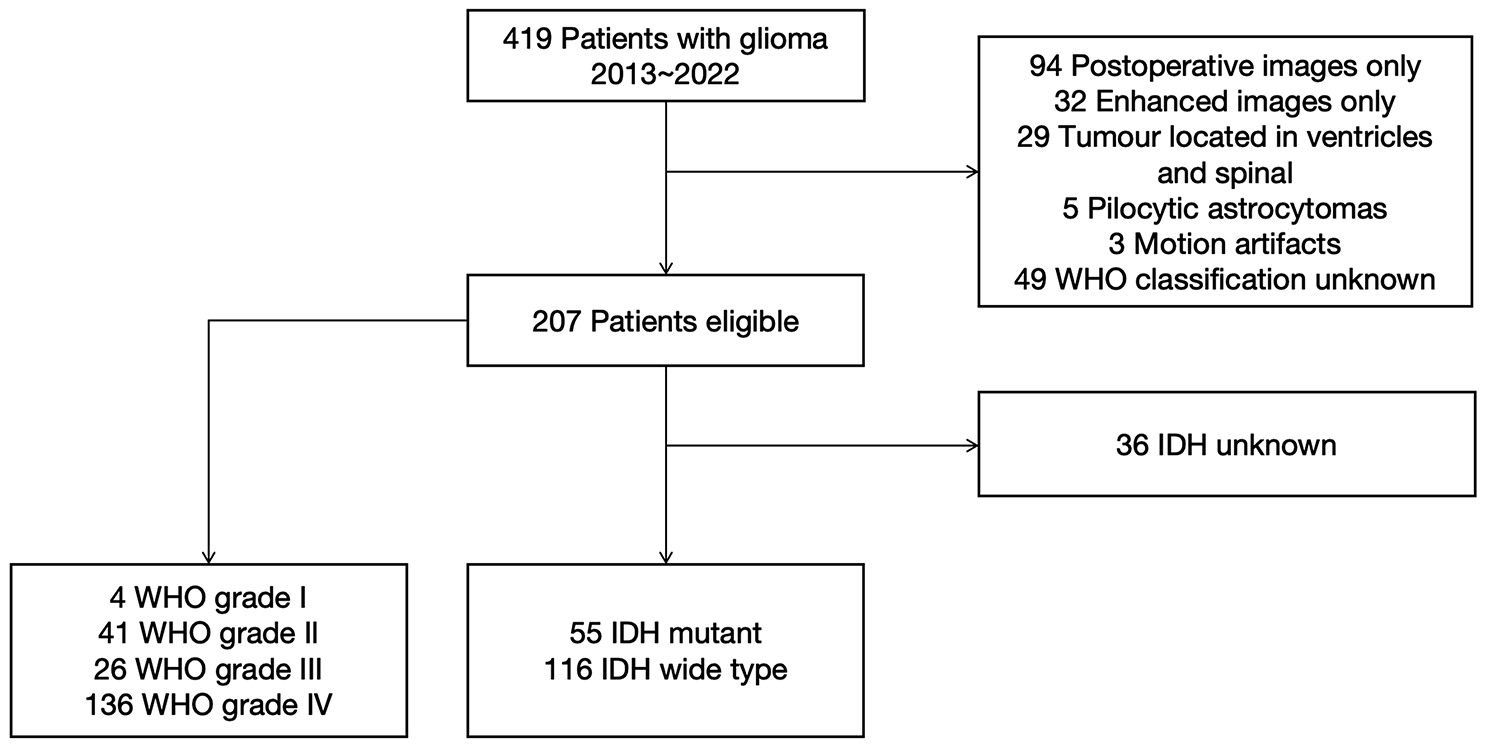
This study was conducted prospectively in accordance with the Declaration of Helsinki and approved by the local institutional review board (number: 1991/2018). For spectroscopic imaging, we included clinically and radiologically suspected low- or high-grade glioma patients prior to the planned surgical resection. Written, informed consent was obtained from all participants. Exclusion criteria were claustrophobia, ferromagnetic implants, non-ferromagnetic metal head implants > 12 mm, pregnancy, and a Karnofsky performance status < 70. The authors of this work had complete control of the study procedures, data analysis, and content of this report. Post-surgical histological diagnosis according to the latest 2021 WHO guidelines [6] provided the gold standard reference for the analysis.
MRI protocols
We imaged with a concentric ring trajectory-based MRSI sequence on a 7 T Magnetom scanner (Siemens Healthcare, Erlangen, Germany) with a 32-channel receive array coil (Nova Medical, Wilmington, MA, USA), featuring a 64 × 64 × 39 matrix with 3.4 mm3 isotropic resolution [15]. The acquisition took 15 min with 450 ms TR and 1.3 ms acquisition delay, covering a manually placed 220 × 220 × 133 mm3 field of view (FOV) [10, 15]. More details are found in Supplementary Table 2, which reports MRS parameters in the MRSinMRS standard [16]. We additionally obtained 7 T 0.8 mm3 isotropic T1-weighted MP2RAGE in 8:02 min and 0.8 mm3 isotropic fluid-attenuated inversion recovery (FLAIR) in 8:10 min.
Clinical 3 T MRI consisted of FLAIR, T2-weighted MRI, and pre- and post-contrast T1-weighted MRI (Gadoteridol, 0.1 mmol/kg).
Post-processing
In-house-developed software postprocessing [15, 17] of MRSI data included gridding, lipid removal by regularization [18], and Hamming filtering. LCModel (v6.3–1, LCMODEL Inc, ONT, CA) spectral fitting included a basis set of N-acetyl-aspartate and NAA-glutamate (tNAA), creatine and phosphocreatine (tCr), tCho, myo-inositol (Ins), scyllo-inositol, γ-aminobutyric acid (GABA), glutathione (GSH), glutamate (Glu), Gln, Gly, taurine (Tau), serine (Ser), cysteine, 2HG and a single macromolecular baseline [17] with an evaluation range of 1.8–4.1 ppm. These formed all the features considered for analysis. A neuro-radiologist with 15 years of specialist experience segmented clinical image-derived tumor regions (i.e., edema or non-contrast enhancing (NCE), CE, and necrosis (NEC)) based on T1, FLAIR and contrast images only, blinded to additional information. We included all spectroscopic voxels within the CE + NCE tumor segmentation that had passed spectral quality filtering [10] (e.g., tCr SNR > 5; tCr FWHM < 0.15 ppm; metabolite Cramér–Rao lower bounds (CRLB) < 40%).
We assessed MRSI quality visually. If most of the tumor focus (i.e. CE and most of NCE) was located in the caudal brain regions with poor spectral coverage, we excluded the whole dataset from further analysis.. Ratio maps of each unique feature denominated by tCr, tCho, and tNAA were established for statistical evaluation and labeled with histologically derived IDH status and tumor grade. We eliminated one in two ratios with a correlation coefficient greater than 0.95. We defined tumor hotspots from which the voxels for the following classifier would be drawn by using lower thresholds based on values obtained from a previous MRSI study in healthy volunteers [19] (i.e., min, mean, and max ratios out of a range of segmented brain ROIs; using three different thresholds to determine how reliant classification was on specific thresholds). Only voxels which were above the threshold for both tCho/tNAA and Gln/tNAA were selected. We eliminated voxels with either tCho/tNAA and Gln/tNAA ratios above 10 as well in order to reduce distortion by very low tNAA fits. Only the remaining of the (all patients) total 55,106 tumour voxels would be used for the RF and SVM.Statistical testing.
We used a Wilcoxon-Mann–Whitney-Test (WMW) to compare key metabolic ratio values of all grade 3 and grade 4 tumor voxels for statistical significant differences in IDHmutation (mt) vs. wildtype (wt).
Classifier design
Random forest (RF) and SVM-based IDH classification and grading were performed by wrapper-type recursive feature elimination with cross-validation (RFECV) [20] feature selection with area under the curve (AUC) as scoring method. We used an initial set of 33 features, consisting of the tumor voxels’ metabolic ratios (i.e., tNAA, tCr, tCho, Ins, GABA, GSH, Glu, Gln, Gly, Tau, and Ser denominated by (tCr, tCho, and tNAA)). The classification problem was defined as the binomial of each voxels’ IDH and high-grade probability. RF with 10 decision trees, a verbosity of 2, and five-fold cross-validation was used. Training and testing were performed iteratively with leave-one-out cross-validation. In addition, as a reference for comparison, we trained an RF and SVM classifier, based on the in previous studies most discriminably reported single feature tCho/tNAA [8].
The classifier’s prediction probabilities for the labels (IDH or grade) were calculated voxel-wise and then aggregated to arrive at a patient's prediction (e.g., IDH-mt or wt). We explored three different aggregation methods, choosing the dataset's mean (1) and median (2) of IDH-mt and high-grade probabilities. The percentage of a dataset's IDH-positive or high-grade voxel was calculated as the patient's binomial (3) aggregation. RF and SVM prediction was performed over CE + NCE ROIs. For each voxel, a RF and SVM based IDH and HG predictive value was calculated. In each patient dataset, the min/median/mean/max values for these predictions were processed to form the one aggregated patient-based value. Binomial aggregation was an aggregation method, in which each voxels’ predictory IDH and grade values (e.g., 0.2 and 0.7, respectively) were transformed towards binomial representation (in that example, 0 and 1 respectively). There was a negligible impact on the statistical outcomes in binomial versus exact voxel value aggregation (to whole patient value).


留言 (0)