Acute pancreatitis can progress to necrosis of the pancreatic tissue and/or peripancreatic tissue which will require intervention if the necrosis becomes infected.
1 Alternatively, a feared adverse event of performing a distal pancreatectomy is the development of a pancreatic leak, which can lead to pancreatic fluid collections.
2 While traditional management entailed utilization of percutaneous drains or re-operation, endoscopic transmural drainage offers another treatment option for these collections.
3 We describe a case of utilizing endoscopic powered debridement devices to treat a large post-operative collection with primarily fatty contents. Consent was obtained from the patient for submission of this case report.
A 71-year-old man with a history of pancreatic neuroendocrine tumor status post distal pancreatectomy developed a large walled-off pancreatic necrosis (WOPN) collection. He initially underwent dual-modality drainage via endoscopic ultrasound-guided cystogastrostomy with a lumen-apposing metal stent (LAMS) and percutaneous drain placement. Due to the increasing size of the collection, we performed direct endoscopic necrosectomy (DEN).
The entrance through the LAMS revealed a large cavity filled with fatty necrotic tissue and copious amounts of oil droplets (
Fig. 1,
Supplementary Video 1). Necrosectomy using a snare proved unsuccessful as the snare could not grasp sufficiently large pieces. A 3.2-mm powered debridement device (EndoRotor; Interscope Inc.) was then used to perform necrosectomy (
Fig. 2), which was partially successful in clearing the cavity. In the subsequent procedure, a 6.0-mm debridement device (
Fig. 3) was utilized (
Supplementary Video 1), which led to the significant removal of large amounts of necrotic tissue from the cavity. Using a percutaneous drain as a guide, the necrosectomy was successful in clearing the cavity down the left paracolic gutter and into the pelvis. At the conclusion of the procedure, a small amount of necrotic tissue and a large amount of pink viable tissue were observed within the cavity (
Fig. 1D).
DEN has emerged as a standard treatment for WOPN that does not respond to drainage alone.
1 Technical challenges in DEN include the lack of effective tools for removing or grasping necrotic tissue. The powered debridement device acts as a morcellator, simultaneously cutting and suctioning necrotic debris. Preliminary studies examining the 3.2-mm catheter have demonstrated its safety and efficacy, suggesting that its use may result in fewer procedures than conventional treatment.
4,
5 In an international, multicenter prospective study involving 30 patients with symptomatic WOPN with at least 30% necrosis, DEN with this device led to successful clearance of all necrotic contents in 97% of the participants.
4 Half of the patients had complete clearance within one session with 73% having complete clearance within two sessions. Importantly, this study found no device-related adverse events, although the primary concern with using this device was bleeding, given the possibility of damaging a vessel hidden within the necrotic debris.
Furthermore, larger studies are needed to determine the optimal indications for the use of this debridement device, highlighting the utility of using 3.2- and 6.0-mm catheters to perform DEN in fatty pancreatic necrosis refractory to conventional techniques. We postulate that the lipolytic activity of the ongoing pancreatic leak likely leads to high amounts of fatty necrosis, providing an ideal scenario for the use of a morcellating system.
Supplementary Material

Supplementary materials related to this article can be found online at
https://doi.org/10.5946/ce.2023.120.
NOTES
Conflicts of Interest
The authors have no potential conflicts of interest.
Funding
None.
Author Contributions
Conceptualization: all authors; Data curation: JD, SM; Formal analysis: all authors; Investigation: JD, SM, PJL, SH; Methodology: SH; Project administration: PJL, SH; Resources: ACA, WKH, SH; Software: SH; Supervision: SH; Validation: PJL, SH; Visualization: SH; Writing–original draft: JD, SM, SH; Writing–review & editing: all authors.
Fig. 1.Pancreatic necrosis with strands of fatty tissue (A) with unearthing of percutaneous drain during necrosectomy (B), with further clearance of necrosis alongside the drain (C), and large amounts of necrotic tissue removed at the completion of two necrosectomy sessions (D).
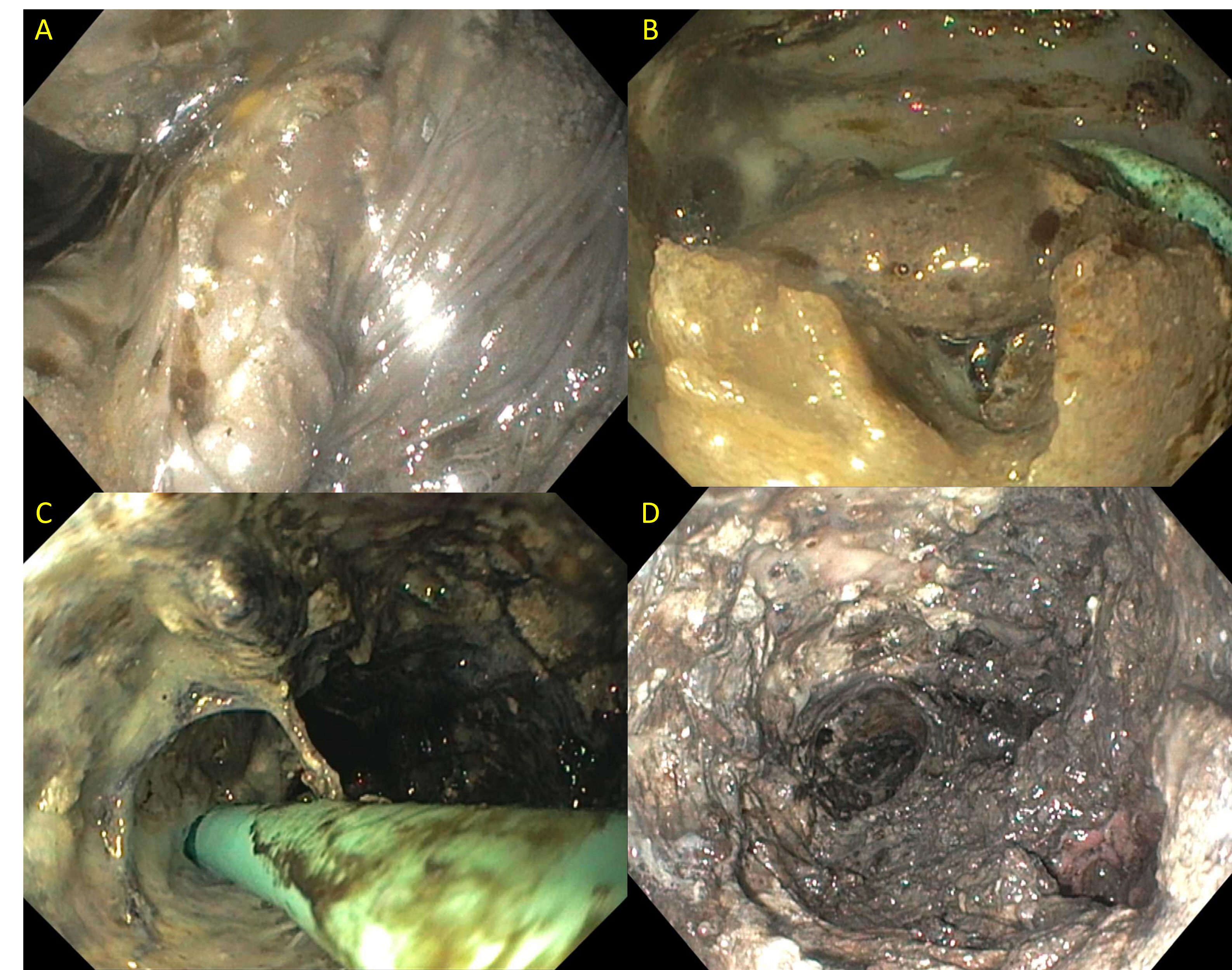 Fig. 2.
Fig. 2.Debridement of necrotic tissue using the powered debridement device.
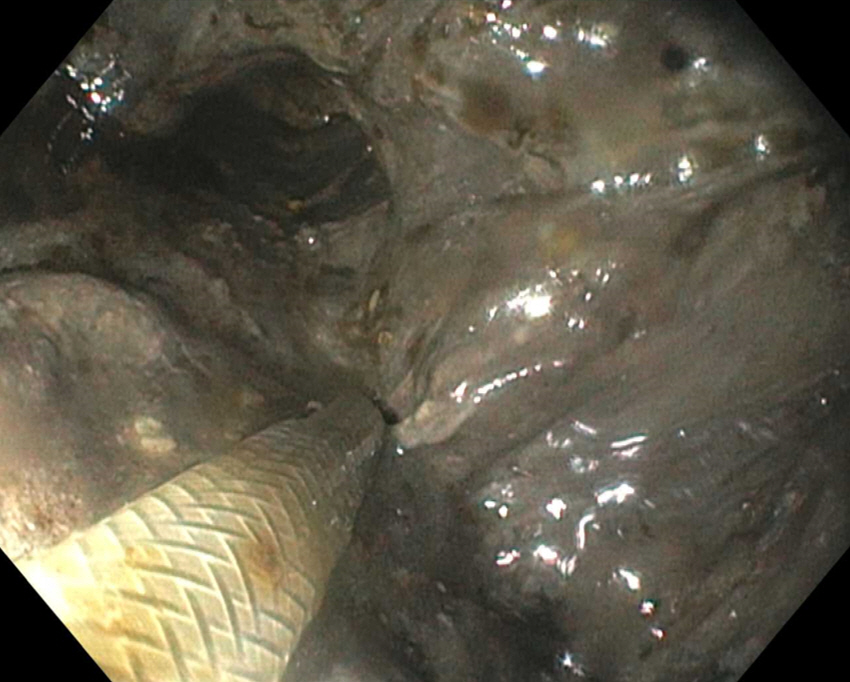 Fig. 3.
Fig. 3.Side by side comparison of the two sizes of the powered debridement device with the 3.2-mm catheter on top and 6.0-mm catheter below (provided courtesy of Interscope Inc.).

REFERENCES
1. Baron TH, DiMaio CJ, Wang AY, et al. American Gastroenterological Association clinical practice update: management of pancreatic necrosis. Gastroenterology 2020;158:67–75.
ArticlePubMed
2. Ciprani D, Bannone E, Marchegiani G, et al. Progression from biochemical leak to pancreatic fistula after distal pancreatectomy. Don't cry over spilt amylase. Pancreatology 2022;22:817–822.
ArticlePubMed
3. Oh CH, Lee JK, Song TJ, et al. Clinical practice guidelines for the endoscopic management of peripancreatic fluid collections. Clin Endosc 2021;54:505–521.
ArticlePubMedPMCPDF
4. Stassen PM, de Jonge PJ, Bruno MJ, et al. Safety and efficacy of a novel resection system for direct endoscopic necrosectomy of walled-off pancreas necrosis: a prospective, international, multicenter trial. Gastrointest Endosc 2022;95:471–479.
ArticlePubMed
5. van der Wiel SE, Poley JW, Grubben MJ, et al. The EndoRotor, a novel tool for the endoscopic management of pancreatic necrosis. Endoscopy 2018;50:E240–E241.
ArticlePubMed
Citations
Citations to this article as recorded by


留言 (0)