
記住我






The study was conducted in the First Affiliated Hospital of Chongqing Medical University from March 1, 2023 to May 31, 2023. This manuscript adheres to the Consolidated Standards of Reporting Trials (CONSORT) guidelines. This clinical trial research received approval of the Ethics Committee of the First Affiliated Hospital, Chongqing Medical University (Ethics Number: 2023-050). It was registered with the China Clinical Trial Registration Center on 28/02/2023 (Registration Number: ChiCTR2300068765), with the registration completed prior to the enrollment of any patients.
Inclusion criteria: (1) elective surgery for knee arthroscopy; (2) ASA grade I-III; (3) age 15–70 years; (4) patients under general anesthesia, signed informed consent and refused to use postoperative analgesia pump.
Exclusion criteria: (1) patients with NYHA ≥ III; COPD and lung function ≥ III grade; liver function Child-Pugh B and C grade; eGFR < 60 ml/min); (2) prolonged use of opioid analgesics or non-steroidal anti-inflammatory drugs for over one year; (3) patients with abnormal coagulation function; (4) patients with contraindications to local anesthetic drugs. (5) patients who cannot cooperate.
Eliminate criteria: (1) subjects withdrew informed consent without any reason; (2) loss of follow-up. (3) patients with postoperative neuropsychiatric disorders who could not cooperate.
All patients signed the informed consent before surgery with refused to use the postoperative analgesia pump. According to the SPSS25 software pre-generated random number table, this table contains the sequence of 1-100 and corresponding groups. Patients included in the trial were randomly divided into FTB group and ACB group according to the order of operation and corresponding random number table. Prior to grouping, the researcher informed the group operator of grouping assignments by using consecutively numbered, opaque, sealed envelopes. Group FTB or Group ACB had a preoperative ultrasound-guided single-injection with 20 ml of 0.2% ropivacaine.
Blindingaside from the regional anesthesiologist and the investigator, surgeons, theatre anesthesiologists, physiotherapists, nurses, caregivers, the data recorder, and data analysis were blinded to group allocation. Unmasking did not occur until statistical analysis was complete. Surgeons, operating room anesthesiologists, physical therapists, nurses, caregivers, cannot use the body surface after surgery to determine what type of block was performed. In our study, which was a single injection and no obvious covering to indicate where the procedure was performed.
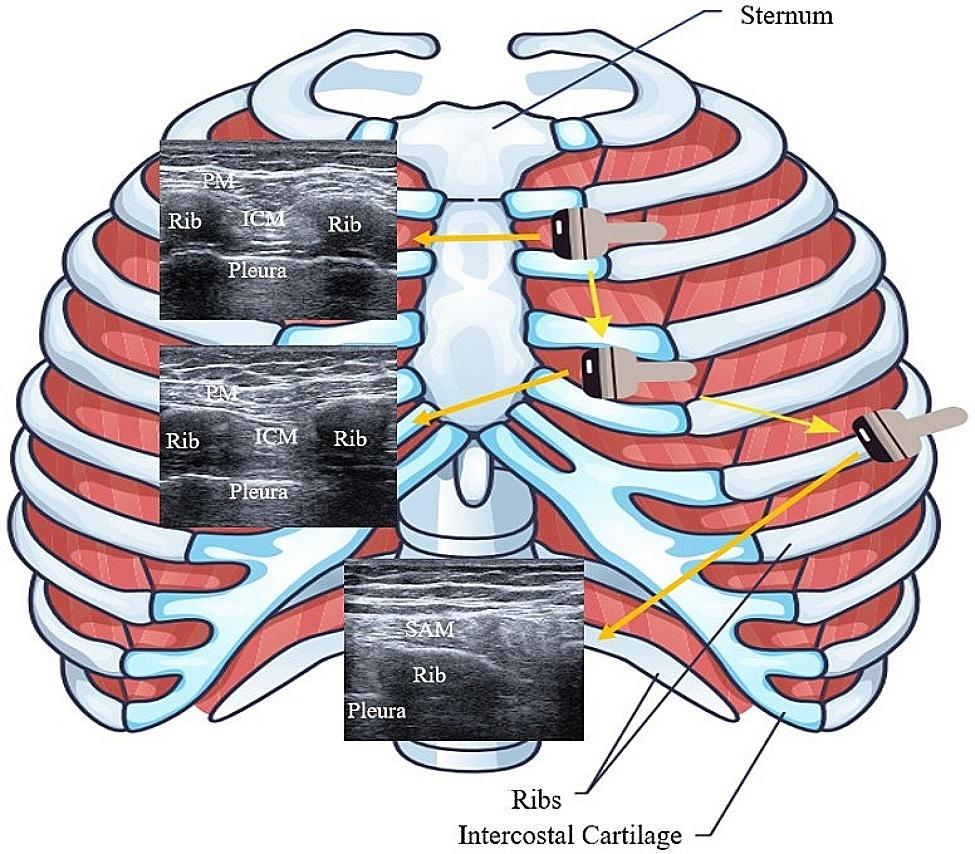
Preoperative FTB or ACBAll patients entered the preparation room in advance, routine ECG monitoring, intravenous access and mask oxygen inhalation were established. During the nerve block, the patient was placed in the supine position, the knee joint was slightly abduction, the leg was slightly external rotation. high-frequency linear array probe 12 L-RS (4.2–13 MHZ, array element 192, GE Healthcare) was used to find the apex of the FT as the distal end of the FT, the inguinal ligament as the proximal end of the FT. A suitable puncture plane was found along the midpoint of the distal and proximal lines toward the medial thigh, which was used as the puncture point of the FTB. In the same way, the apex of the FT is found as the entrance of the AC, then the femoral artery is extended down to explore the inside of the AC. When the femoral artery passes through the adductor canal hiatus, it is the exit of the AC. The midpoint of the exit-entry lines was used as the puncture point for AC. Aseptic and in-plane techniques were used, a 0.7*80 mm (22G) enhanced developing needle (F type, LEAPMED, CHN) was used to inject. regardless of whether the saphenous nerve was visualized or not, 2–3 ml of normal saline was injected via the needle for hydro-dissection, and proper needle tip placement within the FT or AC was confirmed. The local anesthetic drugs were prevented from misrunning into the blood vessels by intermittent withdrawal. The injectate was seen peri-arterially spreading around the femoral artery. Nerve blocks in all patients were performed by the same experienced anesthesiologist. The loss of pinprick sensation over the knee joint area within 15 min after the injection was deemed a successful block. Figure 1.
Fig. 1
Ultrasound image of the plane of the puncture site
Intraoperative periodAfter the block, the patient was transferred to the operating room. Midazolam 0.03 mg/kg, sufentanil 0.3 µg/kg, propofol 1.5-2.0 mg/kg, vecuronium 0.1 mg/kg or rocuronium 1 mg/kg were intravenously injected for induction of general anesthesia. The depth of anesthesia was maintained by continuous pumping of remifentanil, propofol, and inhalation of sevoflurane, the fluctuation of circulation was maintained less than 30% of the basal level. After surgery, the patient was extubated through PACU and returned to the ward.
Postoperative periodAll patients received intravenous infusion of flurbiprofen axetil for postoperative analgesia (50 mg, q12h.ivdrip).
Remedial analgesic solutionIf the NRS at rest was ≥ 5, Acetaminophen tramadol (37.5 mg, st.po) or tramadol injection (100 mg, st.ivdrip) was used as rescue analgesia within 24 h after surgery. If the pain was not significantly relieved or continued to worsen, acetaminophen tramadol (37.5 mg, st.po) could be re-administered within 6 h until the NRS at rest was < 5.
Outcome measures The primary outcomeThe primary outcome was the numeric rating score (NRS) at 12 h after surgery at rest and during movement. The NRS is an 11-point scale ranging from 0 to 10. 0 is no pain, 10 is the worst pain, the NRS at rest was defined as the pain score measured while the patient was resting in bed, and the NRS during movement was the pain score measured while the patient was performing the Manual Muscle Testing (MMT) for muscle strength.
Secondary outcomes: (1) The NRS at post anesthesia care unit (PACU) and 2, 24 h after surgery at rest and during movement; (2) The quadriceps muscle strength at PACU and 2, 12, 24 h after surgery; (3) Consumption of Rescue analgesia; (4) Incidence of adverse reactions. The quadriceps strength is assessed using MMT method as follows: Grade 0, no muscle contraction; Grade 1, slight contraction but unable to move the joint; Grade 2, the joint can move horizontally but cannot resist the gravity of the lower limbs; Grade 3, can resist lower limb gravity, but not resistance; Grade 4, can resist lower limb gravity and can resist certain resistance; Grade 5, able to exercise against large resistance. The NRS and quadriceps muscle strength at rest and during movement were recorded by the data recorder (Data recording time can fluctuate ± 30 min, outcomes measures from 0 to 6 am were not recorded, patients who discharged within 24 h after surgery obtain NRS and quadriceps muscle strength through WeChat video call). Rescue analgesic consumption during the first 24 h after surgery was transformed by the oral morphine equivalent (OME). The consumption of anesthetic drugs, vasoactive agents during the perioperative period, the consumption of rescue analgesics within 24 h after surgery and the incidence of adverse events were recorded.
Sample size calculationIn our pilot study of 8 arthroscopic surgery patients with the ACB or FTB, the standard deviation of NRS was 1.65 after 12 h postoperatively. In our study the minimal clinically important difference (MCID) of the mean difference of NRS was 1.33 [14]. The sample size calculation for this study was based on two independent samples nonparametric tests with PASS15 software. According to the loss rate of follow-up of 20% in each group, 45 cases were needed to be included in each group.
Statistical analysisThe investigator used SPSS25 software (IBM SPSS Statistics version 25.0, IBM©, Armonk, NY, USA) to analyze the data. The Shapiro-Wilk tests were used to confirm normality of the data distribution. Independent sample T test was used to analyze the data with normal distribution, Mann-Whitney U test was used to compare other data between the two groups. multiple linear regression models (Stata/MP17.0, Stata©, LLC4905 Lakeway Drive College Station, TX77845, USA) were used to examine the influence of independent variables such as gender, age, BMI, duration of surgery, and type of surgery on NRS. Continuous variables were presented as mean ± standard deviation (SD) or median with interquartile range (IQR). Categorical variables were expressed as numbers (percentages). Adjusted NRS were also presented as mean differences. two-sided tests with p < 0.05 were considered statistically significant.
留言 (0)