
記住我
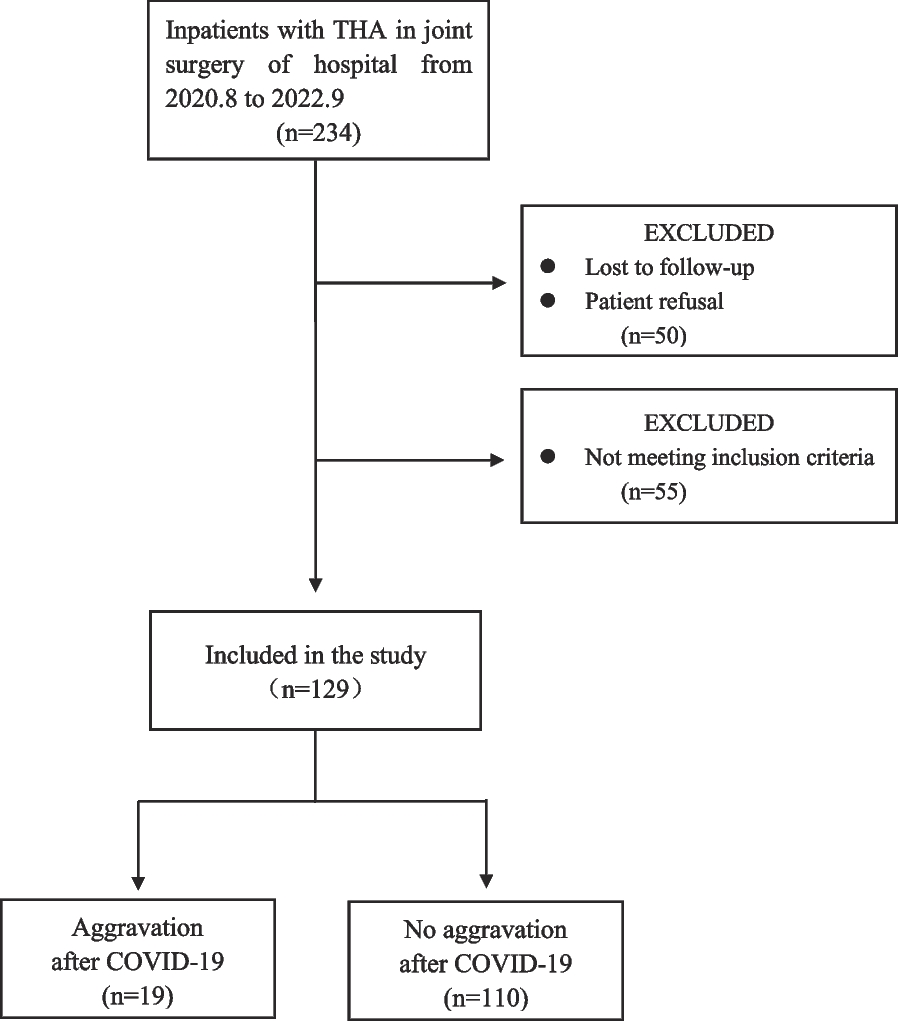



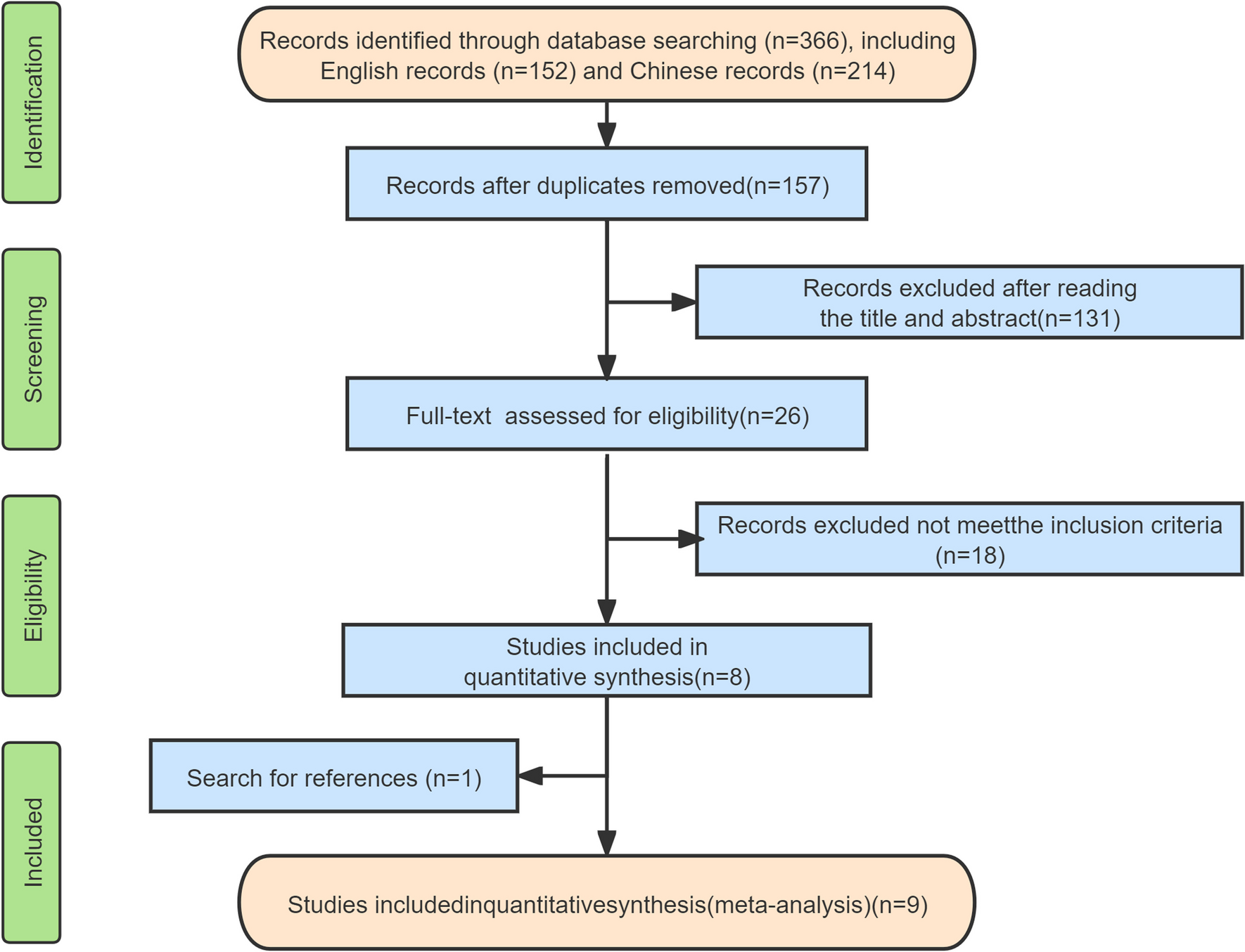
A total of 554 articles were retrieved by searching each database; 135 articles were eliminated by EndNoteX9 software, 398 were deleted after reading titles and abstracts, and the remaining 21 were retained. After reading the full text, 10 articles were excluded, of which 1 was not an RCT, 2 were not available for full text, 1 did not have the correct intervention, 6 data could not be integrated, and were finally included in 11 articles. The flowchart of the literature selection process is shown in Fig. 1.
Fig. 1
Flowchart of study selection
A total of 940 patients were included in the 11 articles [11,12,13,14,15, 18,19,20,21,22,23]. Nine of the studies were from China, while the other two were from Turkey and Japan. The studies, published between 2008 and 2022, ranged in sample size from 30 to 168 people. Except for one study [14] in which the massage method was self-massaged under the guidance of a professional therapist, the massage method in other studies was administered by a professional therapist. And except for one study [20] that used the “massage vs. other treatments” model, the remaining studies used the “massage + other treatments vs. other treatments” model.
In addition, four studies [19, 21,22,23] did not report the occurrence of adverse events. Table 1 summarizes the characteristics of the included studies.
Table 1 Characteristics of the included RCTSRisk of biasAll included studies randomized the allocation of subjects. Nine studies [12,13,14,15, 18,19,20, 22, 23] documented the randomization method in detail, and three [12, 13, 18] of them detailed the allocation concealment process. Two studies [12, 13] were blinded to the outcome assessor. Moreover, only one study [18] described the blinding of subjects and therapists. The detailed results are shown in Fig. 2.
Fig. 2 Meta-analysisPostoperative pain
Meta-analysisPostoperative painThree studies [11, 12, 23], including 226, 140, and 110 patients, reported pain at 7 days after TKA, three [11, 18, 23] at 14 days after TKA, and two [11, 20] at 21 days after TKA, respectively. A random effects model was used for the meta-analysis. The results showed that the degree of pain in the massage group (MG) was significantly lower than that in the control group (CG) at 7 [MD = -1.21 (95%: − 1.76, − 0.65), p < 0.0001, I2 = 68%];14 [MD = − 5.32 (95%: − 8.74, − 1.90), p = 0.02, I2 = 96%]; and 21 days [MD = − 2.14 (95%: − 3.10, − 1.17), p < 0.0001, I2 = 74%] after surgery (Fig. 3).
Fig. 3
Meta-analysis and forest plot for postoperative pain at different time points. a–c Pain on postoperative days 7, 14, and 21, respectively
Knee ROMTwo studies [11, 12] reported knee ROM at 7 days after TKA, including 84 patients in the MG and 82 in the CG. A fixed effects model was used for the meta-analysis. The results showed that the MG improved the knee ROM more than did the CG at 7 days after surgery, and the difference was statistically significant [MD = 6.39 (95%: 4.26,8.51), p < 0.00001, I2 = 38%]. Two studies [11, 18] reported knee ROM at 14 days after TKA, including 40 patients in the MG and 40 in the CG. A random effects model was used for the meta-analysis. The results showed that the MG improved the knee ROM more than did the CG at 14 days after surgery, and the difference was statistically significant [MD = 11.98 (95%: 4.65, 19.31), p = 0.001, I2 = 80%] (Fig. 4).
Fig. 4
Meta-analysis and forest plot for knee ROM at different periods. a Knee ROM on the 7th day after surgery; b knee ROM on the 14th day after surgery
Postoperative D-dimer levelsThree studies [13, 19, 23] reported D-dimer levels at 14 days after TKA, including 105 patients in the MG and 106 in the CG. A random effects model was used for the meta-analysis. The results showed that the D-dimer level in the MG decreased more significantly than that in the CG at 14 days after surgery, and the difference was statistically significant [MD = -0.40 (95%: -0.75, -0.04), p = 0.03, I2 = 97%]. Two studies [15, 21] reported D-dimer levels 15 days after TKA, including 58 patients in the MG and 58 in the CG. A random effects model was used for the meta-analysis. However, there was no significant difference in D-dimer levels between the massage and control groups at 15 days after surgery [MD = 0.02 (95%: − 0.12,0.15), p = 0.80, I2 = 96%] (Fig. 5).
Fig. 5
Postoperative D-dimer levels at different time points. a D-dimer level on the 14th day after surgery. b D-dimer level on the 15th day after surgery
Length of hospital stayFive studies [11, 14, 15, 18, 22] reported the length of hospital stay after TKA, including 220 patients in the MG and 223 in the CG. A random effects model was used for the meta-analysis. The results showed that the length of hospital stay was significantly shorter in the MG than in the CG [MD = − 5.32 (95%: − 8.74, − 1.90), p = 0.002, I2 = 96%] (Fig. 6).
Fig. 6 Subgroup analyses
Subgroup analysesDue to the small number of studies included for the remaining outcomes, we performed subgroup analyses only for the outcome of length of hospital stay. To explore the sources of heterogeneity, we divided the analysis into two subgroups, China and other countries, according to country type. The results showed that massage treatment shortened the length of hospital stay for TKA patients in China [MD = − 3.79 (95%: − 4.36, 3.22), p < 0.00001, I2 = 0%] but not for TKA patients in other countries [MD = 0.08 (95%: − 0.17, 0.33), p = 0.53, I2 = 0%], and the heterogeneity between the two subgroups was significantly lower, confirming the country type as a source of heterogeneity (Fig. 7).
Fig. 7
Subgroup analysis of length of hospital stay
In addition, according to the Cochrane Handbook [24], sensitivity analysis was not performed in this study due to the small amount of literature included for each outcome.
Publication biasIn this study, we examined publication bias using Begg's and Egger's tests. The results showed potential publication bias in the outcome of postoperative day 14 pain according to Egger's test (p = 0.049), and no evidence of significant publication bias was found in the remaining included studies. (p > 0.05). In addition, Egger's test could not be performed for pain at postoperative day 21, knee ROM at postoperative day 7, knee ROM at postoperative day 14, or D-dimer level at postoperative day 15 because only two studies were included for each outcome. (Supplementary Table S2).
Adverse eventsSeven studies [11,12,13,14,15, 18, 20] reported adverse events. In one study [11], one patient in the CG was reported to have DVT, and another study [15] reported adverse events in three patients in the CG, but the details were not available. No adverse events were reported in the remaining studies.
留言 (0)