
記住我










A gastrointestinal stromal tumor (GIST) is a common mesenchymal tumor (1), with an annual incidence of 1–2 per 100,000 people (2). GISTs can be found in any part of the digestive tract, including the stomach (40%–50%) and small intestine (20%–40%) (3). Surgical removal is the preferred treatment for gastric stromal tumors (4), and negative surgical margins of pathological specimens are considered a mandatory requirement (5). Due to the low rate of lymph node metastasis, routine prophylactic lymph node dissection is not recommended (6, 7).
In 2000, Kimata et al. (8) reported the first laparoscopic surgery for GISTs. Since then, laparoscopic surgery has been widely accepted for the treatment of GISTs. Many retrospective studies have demonstrated the feasibility and safety of laparoscopic resection of gastric GISTs (9–12). However, for tumors located in challenging locations, such as the GEJ, lesser curvature, posterior gastric wall and antrum, the difficulty of radical resection of the tumor by laparoscopic surgery is greatly increased. According to the National Comprehensive Cancer Network (NCCN) guidelines (13), laparoscopic surgery is recommended to be performed by experienced surgeons for patients with GISTs in easily accessible anatomical locations. We believe that laparoscopic treatment of gastric gists in challenging anatomical locations has not been recommended mainly because of the flexibility limitations of laparoscopic surgery.
Previous studies have also shown that minimizing the amount of tumor-free tissue resected and maximizing the amount of gastric remnant improve patient quality of life (14). For gastric GISTs located in challenging locations, especially the GEJ or pylorus, surgeons often perform laparoscopic-assisted esophagectomy or subtotal gastrectomy (15, 16), which poses a challenge for preserving gastric function. Currently, the safety and feasibility of robotic surgical resection of gastric GISTs have been demonstrated (17–19). Robot-assisted surgery allows more precise tumor resection and preserves as much gastric tissue as possible. Recent studies have shown that robotic surgery has certain advantages in preserving gastric pylorus and cardia function (20). In this study, we performed robot-assisted surgical endoscopic localization and manually sutured the remnant stomach to treat gastric GISTs in challenging anatomical locations. There is no channel deformity or stenosis caused by excessive resection of tumor-free gastric tissue with this technique.
Methods Patients and study designIn the design of this study, we collected and retrospectively analyzed the clinical data of patients who had undergone robot-assisted surgery combined with upper gastrointestinal endoscopic localization for the treatment of all patients with gastric GISTs located in challenging locations gastric GIST. The data included: The demographic data, clinical manifestations, surgical methods, histopathology, postoperative and oncological outcomes from August 2021 to April 2023. Inclusion criteria: (1) Postoperative pathological diagnosis was gastric stromal tumor. (2) Robot-assisted surgery combined with upper gastrointestinal endoscopic localization was performed. (3) Age ≥18 years old. Exclusion criteria: (1) Gastric stromal tumors located in easily dissected locations. (2) Patients with gastric stromal tumors treated with standard laparoscopic or open surgery. All patients were diagnosed by gastroscopy, EUS or CT before surgery and pathological examination after surgery. All procedures were performed at our center by a single experienced laparoscopic surgeon. All patients provided written informed consent.
Challenging tumor location definitionAccording to the National Comprehensive Cancer Network (NCCN) guidelines (13), tumors located in the gastroesophageal junction (GEJ), lesser curvature, posterior gastric wall, or antrum were classified as challenging.
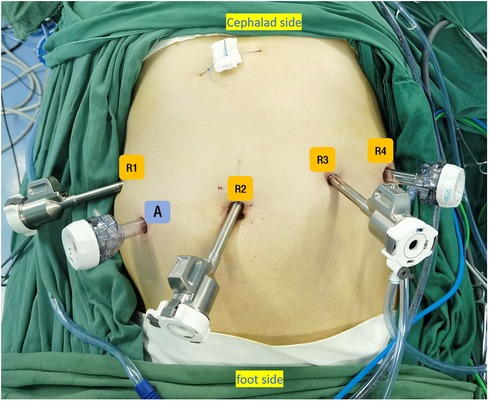
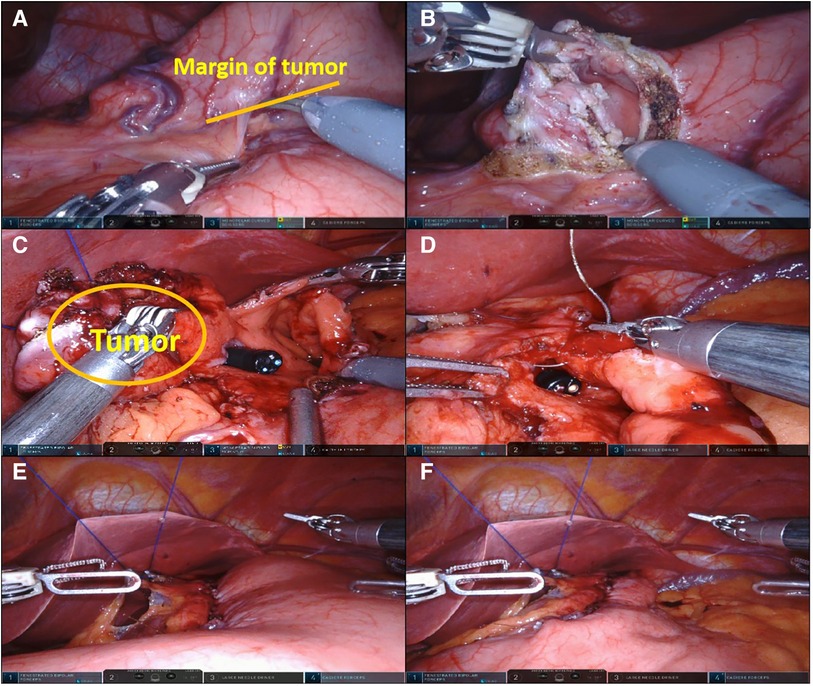
Surgical procedureAfter entering the operating room, the patient was placed in the supine position and intubated for anesthesia induction (Figure 1). Upper gastrointestinal endoscopy was routinely performed to provide an intraluminal view of the tumor boundaries to guide precise resection. A parachute suspension technique was used to expose the left subhepatic space (Figure 2). After dissection of the hepatogastric ligaments or gastrocolic ligament, endoscopy was performed to localize the tumor. After removal of the tumor with an ultrasonic scalpel or electric scissors, the gastric wall was repaired by continuous inverted suture with 3-0 barbed suture. Endoscope-guided suturing ensured patency of the gastroesophageal junction or pylorus. The specimen was loaded into a pouch and removed through a periumbilical incision.
Figure 1. Trocar placement for RALE-PG. (A) 12-mm trocar (R2) was placed at the lower umbilical margin, two 8-mm trocars were placed under the costal margin on the left anterior axillary line (R4) and at the intersection of left midclavicular line and a horizontal line 1 cm above the umbilicus (R3), One 8-mm trocar was placed under the costal margin on the right anterior axillary line (R1) and one 12-mm trocar was placed at the intersection of right midclavicular line and a horizontal line 1 cm above the umbilicus (Auxiliary port A).
Figure 2. RALE-PG. (A) The tumor was localized by upper gastrointestinal endoscopy and robotic laparoscopy; (B, C). The tumor was accurately removed under the supervision of upper endoscopy; (D). Under endoscopic guidance, the remnant stomach was sutured manually; (E). Inflation experiments were performed to check for anastomotic condition; (F). Key surgical procedures were completed.
Perioperative managementAll patients followed the ERAS protocol as much as possible after performing RALE-PG. Prophylactic intravenous antibiotics (2 g of ceftazidime) were administered half an hour before surgery. A small amount of water was consumed by mouth 12 h after surgery, and when the patient was asymptomatic or could tolerate it, a liquid diet or semiliquid diet was undertaken in sequence. Upper gastrointestinal radiography was performed before removal of the nasogastric tube to assess the function of the residual stomach. At the same time, patients were encouraged to ambulate from bed early to promote the recovery of gastrointestinal function.
Follow-upThe patients were routinely followed up after surgery by specially trained investigators. Endoscopy was performed in all patients 6–8 weeks after surgery. The last follow-up date for the study was December 2023. The median follow-up time was 19 (10–25) months.
Statistical analysisStatistical analysis was performed with SPSS 25.0. Dichotomous data and counts are presented as frequencies, whereas continuous data are presented as X ± SD and/or median (range).
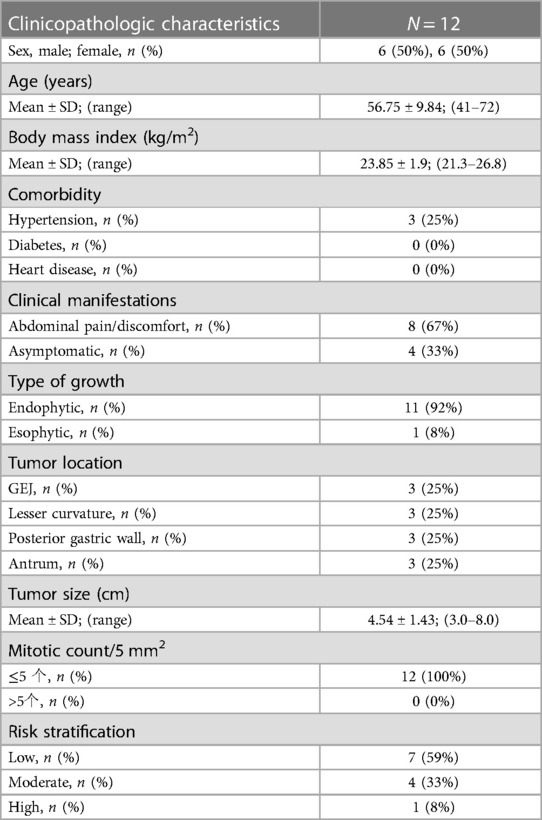
Results Clinicopathologic characteristicsThe clinicopathologic characteristics are summarized in Table 1. This study included 12 patients (6 females and 6 males) with a mean age of 56.8 ± 9.8 years and a mean BMI of 23.9 ± 1.9 kg/m2. The main clinical manifestations of the patients included abdominal pain/discomfort (n = 8, 67%) and no symptoms (n = 4, 33%). One of the tumors located in the stomach antrum exhibited exophytic growth, and the other 11 tumors exhibited endoluminal growth. Tumors were located in the GEJ (n = 3), lesser curvature (n = 3), posterior gastric wall (n = 3) and antrum (n = 3). The cardia and pylorus were successfully preserved in all patients regardless of the tumor location. The mean tumor size was 4.5 ± 1.4 cm. The mitotic-count/50 mm2 was less than 5 in all patients (100%). Pathologic diagnosis was confirmed by immunohistochemistry, revealing gastric GISTs in 12 patients, including 7 at low risk (59%), 4 at moderate risk (33%) and 1 at high risk (8%), according to the Fletcher criteria (21).
Table 1. Clinicopathologic characteristics of patients.
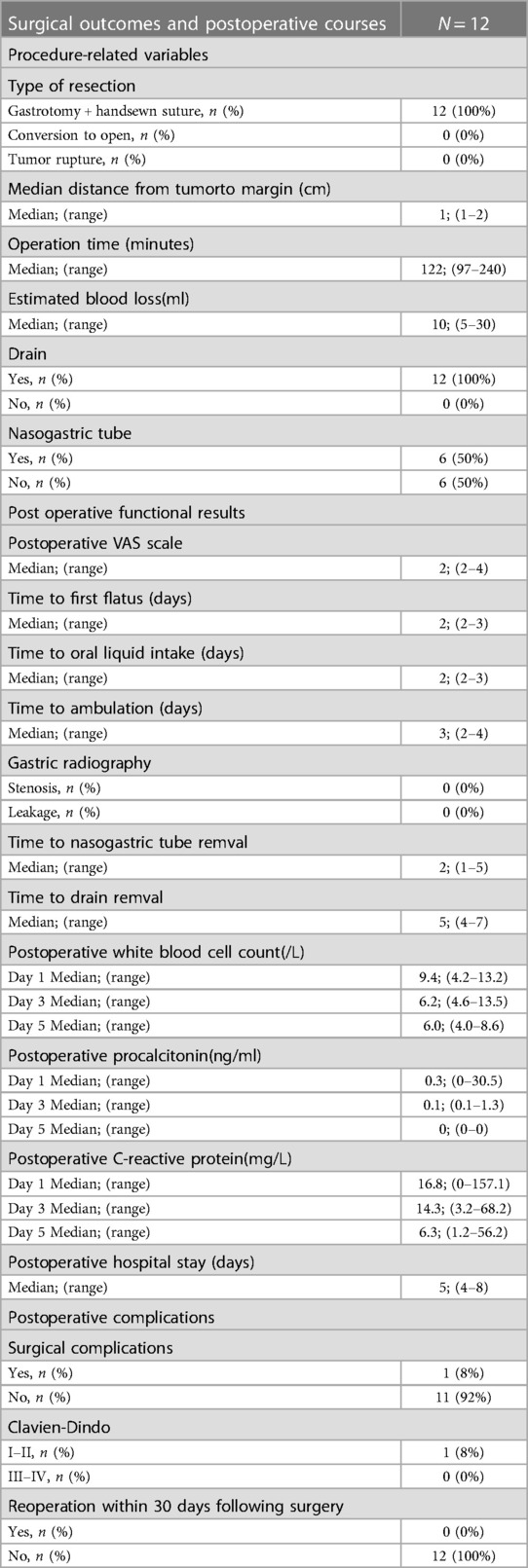
Surgical and postoperative outcomesThe surgical and postoperative outcomes are shown in Table 2. Twelve gastric GIST patients underwent upper gastrointestinal endoscopic localization combined with robot-assisted partial gastrectomy. There was no intraoperative tumor rupture (0%) and no conversion to open surgery (0%). The median operation time was 122 (97–240) min, and the median blood loss volume was 10 (5–30) ml. A nasogastric tube was placed in all patients, and an abdominal drainage tube was placed in 6 patients. At 6 h after surgery, the visual analog scale (VAS) score (22) was used to evaluate postoperative pain. The median postoperative VAS score was 2 (2–4). The median time to first flatus was 2 (2–3) days. The median time to first fluid intake was 2 (2–3) days. The median time to first ambulation after the operation was 3 (2–4) days. All patients were routinely examined by postoperative radioscopy before the nasogastric tubes were removed, and no cases of anastomotic stenosis or leakage were found. The median time to drain removal for 6 patients was 5 (4–7) days. The median time to nasogastric tube removal for all patients was 2 (1–5) days. Inflammatory markers (including white blood cell count, procalcitonin and C-reactive protein) were evaluated on the 1st, 3rd, and 5th days after the operation, and we found that the median concentration of inflammatory markers in the blood of patients tended to decrease. The median postoperative hospital stay was 5 (4–8) days. There was no postoperative leakage, abdominal infection, or gastrointestinal dysfunction. One patient (female/41 year) developed moderate anemia (Clavien-Dindo grade II complication), was treated with blood transfusion and was discharged on postoperative day 7. There was no unplanned readmission within 30 days after the operation. The median distance from the tumor to the resection margin was 1 (1–2) cm.
Table 2. Surgical and postoperative outcomes of patients.
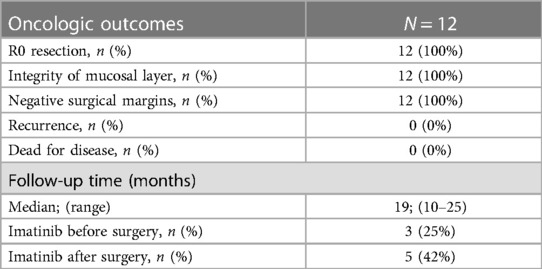
Oncologic outcomesThe oncological outcomes are shown in Table 3. R0 resection was achieved in all patients, and the integrity of the mucosal layer was maintained in all patients. The median follow-up period was 19 (10–25) months, and all patients survived with no recurrence or metastasis. Three patients received imatinib as preoperative treatment, and 5 patients received imatinib treatment after surgery (42%).
Table 3. Oncologic outcomes of patients.
DiscussionOur case series focused specifically on gastric function protection in gastric GIST patients with tumors in challenging anatomic locations, including the GEJ (n = 3), lesser curvature (n = 3), posterior gastric wall (n = 3), and antrum (n = 3). Compared to patients in the literature, patients in our case series had larger tumors (median size 4.5 cm). In addition, the tumor growth pattern in 11 patients was inward. However, for gastric GISTs in challenging locations, these tumors are not suitable for standard laparoscopic procedures. Based on the experience of Privette (16) and Al-Thani (23), using standard laparoscopic approaches in these areas could lead to excess torque on the lesion and increase the risk of tumor rupture. Because of the unique histopathological features of gastric GISTs, the rate of recurrence in patients with tumor rupture is close to 100% (7, 24). Clearly, RALE-PG overcomes the challenges of standard laparoscopy surgery.
After resection of a gastric stromal tumor in robot-assisted surgery, the remnant gastric wall was sutured by hand instead of using instruments, which benefited from the high flexibility and clear vision of the robotic arm. In terms of surgical safety, there was no conversion to laparotomy or tumor rupture, and our results were better than those of previous studies (RG: 4.2%; LG: 6.3%) (25). Similar to previous studies, no intraoperative tumor rupture occurred in our study [RG: 0% (18); LG: 0% (26)]. The estimated median blood loss volume was 10 (5–30) ml in our study, which is better than that reported in previous studies [RG: 20.0 ml (18); LG: 27.7 ml (11)]. The reason for this may be that the flexible robotic arm and high magnification of the surgical field in robot-assisted surgery allow surgeons to operate more precisely. For the purpose of observing the presence or absence of gastric leakage, abdominal drainage tubes were placed in 6 patients (3 in the GEJ and 3 in the posterior gastric wall), which was a number of patients that was similar to or less than that reported in previous literature (RG: 87.5%; Lg: 53.9%) (25). We prefer to place an abdominal drainage tube in patients with a relatively large remnant gastric anastomosis to observe anastomotic healing and can be used for drainage and decompression if needed. The median operative time in our study was slightly shorter than that in a recent retrospective study (122 vs. 151 min), although it was slightly longer than that in a study with laparoscopic surgery (100 min). This may be related to our experience in performing more than 100 robot-assisted gastrointestinal procedures before we performed this procedure. According to a study by Song et al. (27), the adaptability of robotic surgery increases after 30 operations.
The median postoperative VAS score was 2, and patients experienced only mild postoperative pain. Although few similar studies have focused on these data, in the future, studies with larger sample sizes are needed to confirm these advantages.
The median time to first flatus was 2 days, which was consistent with the findings of a previous study (RG: 2.0 days; LG: 2.0 days). Compared with previous reports (RG: 2.9 days; LG: 3.3 days) (28), the median ambulation time was 3 days, which was not much different. The median time to nasogastric tube removal was 2 days, which was consistent with previous reports (RG: 2 days; LG: 2 days) (25). The median time to abdominal drainage tube removal was 5 days, which was slightly longer than that reported in previous literature (RG: 4 days; LG: 3 days) (25), possibly because of the more conservative drainage tube observation strategy adopted by the surgeon, which generally does not affect the postoperative recovery of patients. Several previous studies have suggested that retaining more gastric tissue is important for gastric function (26) and that traditional gastric wedge resection is more likely to lead to postoperative anastomotic stenosis (14, 25). In our study, manual closure was performed in all patients. Intraoperative upper gastrointestinal endoscopy revealed that the cardia and pylorus were successfully preserved intact without excessive gastric tissue removal. Partial gastrectomy was performed 1 cm from the edge of the tumor, and the gastric wall was repaired with manual sutures. The tissue margin was negative in all patients. Compared with traditional gastric wedge resection, our procedure preserved more normal gastric tissue (1.0 cm vs. 2.5 cm) (20). This suggests that this method has some advantages, but these advantages need to be confirmed in studies with larger sample sizes. All patients underwent upper gastrointestinal radiography before removal of the gastric tube, and no patient experienced stenosis or leakage. A comparative study (25) of different surgical procedures for GIST from Italy showed that robotic surgery appeared to have a lower rate of surgical complications (RG: 4.2%; LG: 6.3%), although there was no statistically significant difference between the groups. All patients underwent upper gastrointestinal endoscopy at 6 months after surgery, and the gastric wall of all patients healed well without ulcers or obvious scar erosion. A report of the modified laparoscopic-endoscopic technique (CLEAN-NET) (26) in Japan showed that there was more irregular scar erosion or ulcers in patients with manual full-thickness sutures. However, this phenomenon did not appear in our study, probably because the greater flexibility and greater lens magnification of the robotic arm in robot-assisted surgery allow the surgeon to easily suture the gastric wall without excessive traction. Of course, the CLEAN-NET has great advantages in preserving gastric function because they only strip the serosa and retain the gastric mucosa and submucosa. However, this technique is difficult to perform for tumors located in challenging anatomical locations, and it is not suitable for tumors that invade the mucosal layer.
Overall, the follow-up period in this study was short, which limited our assessment of long-term oncologic outcomes. Postoperative pathological examination revealed that all patients experienced R0 resection and had negative surgical margins. The blood supply and pseudocapsules of GISTs can easily cause tumor rupture and implantation metastasis during surgery. Therefore, whether R0 resection had been achieved had a great impact on patient prognosis. No recurrence occurred in this cohort at a median follow-up of 19 months. Our results are similar to or better than those of previous studies [100% vs. 95% (29), 100% vs. 87% (24)].
Our study demonstrated the safety and efficacy of this procedure and its advantages in preserving gastric function. However, our study has several limitations. First, the sample size was small, the study was retrospective, and there was no control group. Second, patients included in the present study were mostly assessed as having a low risk of tumor recurrence, which may have biased the assessment of medium- and long-term survival. Finally, the follow-up period in our study was relatively short, so a longer follow-up period is needed to assess the true value and long-term outcome of this technique.
ConclusionsRALE-PG is a safe, feasible and advantageous technique for treating GISTs in challenging anatomical locations. It can be performed to accurately remove the tumor while preserving gastric function to the greatest extent. None of the patients in this study experienced surgical complications or tumor recurrence during the follow-up period, but oncologic outcomes need to be evaluated in studies with a larger sample size and longer follow-up period.
Data availability statementThe original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding authors.
Ethics statementThis study was approved by the ethics committee of Fujian Cancer Hospital and Fujian Provincial Hospital, Fuzhou, People's Republic of China (No. K2024-003-01), and all patients provided informed consent for participation. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent from the patients/participants or patients/participants’ legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributionsCJ: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Visualization, Writing – original draft, Writing – review & editing. XH: Data curation, Formal Analysis, Investigation, Writing – original draft. RL: Conceptualization, Methodology, Writing – review & editing. WY: Conceptualization, Investigation, Methodology, Writing – review & editing. SZ: Conceptualization, Formal Analysis, Investigation, Methodology, Writing – review & editing. HH: Data curation, Investigation, Methodology, Writing – review & editing. SJ: Data curation, Formal Analysis, Investigation, Writing – review & editing. CY: Conceptualization, Investigation, Project administration, Supervision, Validation, Writing – review & editing. SG: Conceptualization, Investigation, Methodology, Project administration, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
FundingThe author(s) declare financial support was received for the research, authorship, and/or publication of this article.
This study was supported by the Natural Science Foundation of Fujian Province, China (Grant number: 2021J011371 and 2023J011289).
Conflict of interestThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's noteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References1. Lim KT, Tan KY. Current research and treatment for gastrointestinal stromal tumors. World J Gastroentero. (2017) 23(27):4856–66. doi: 10.3748/wjg.v23.i27.4856
Crossref Full Text | Google Scholar
2. Song H, Xiao X, Liu G, Zhou J. Sarcopenia as a novel prognostic factor in the patients of primary localized gastrointestinal stromal tumor. BMC Cancer. (2022) 22(1):179. doi: 10.1186/s12885-022-09278-w
PubMed Abstract | Crossref Full Text | Google Scholar
3. DeMatteo RP, Lewis JJ, Leung D, Mudan SS, Woodruff JM, Brennan MF. Two hundred gastrointestinal stromal tumors: recurrence patterns and prognostic factors for survival. Ann Surg. (2000) 231(1):51–8. doi: 10.1097/00000658-200001000-00008
PubMed Abstract | Crossref Full Text | Google Scholar
4. Nagano S, Miyoshi N, Takahashi T, Itakura H, Fujino S, Ogino T, et al. Preoperative imatinib and laparoscopic intersphincteric resection for large rectal gastrointestinal stromal tumor: a case report. Int J Surg Case Rep. (2020) 71:235–9. doi: 10.1016/j.ijscr.2020.05.031
PubMed Abstract | Crossref Full Text | Google Scholar
5. Xiong Z, Wan W, Zeng X, Liu W, Wang T, Zhang R, et al. Laparoscopic versus open surgery for gastric gastrointestinal stromal tumors: a propensity score matching analysis. J Gastrointest Surg. (2020) 24(8):1785–94. doi: 10.1007/s11605-019-04318-6
PubMed Abstract | Crossref Full Text | Google Scholar
6. Demetri GD, Benjamin RS, Blanke CD, Blay JY, Casali P, Choi H, et al. NCCN task force report: management of patients with gastrointestinal stromal tumor (GIST)–update of the NCCN clinical practice guidelines. J Natl Compr Canc Ne. (2007) 5(Suppl 2):S1–29, quiz S30. PMID: 17624289.
PubMed Abstract | Google Scholar
7. Demetri GD, von Mehren M, Antonescu CR, DeMatteo RP, Ganjoo KN, Maki RG, et al. NCCN task force report: update on the management of patients with gastrointestinal stromal tumors. J Natl Compr Canc Ne. (2010) 8(Suppl 2):S1–41, quiz S42–4. doi: 10.6004/jnccn.2010.0116
Crossref Full Text | Google Scholar
8. Kimata M, Kubota T, Otani Y, Ohgami M, Ishikawa Y, Yokoyama T, et al. Gastrointestinal stromal tumors treated by laparoscopic surgery: report of three cases. Surg Today. (2000) 30(2):177–80. doi: 10.1007/s005950050038
PubMed Abstract | Crossref Full Text | Google Scholar
9. Xiong W, Zhu J, Zheng Y, Luo L, He Y, Li H, et al. Laparoscopic resection for gastrointestinal stromal tumors in esophagogastric junction (EGJ): how to protect the EGJ. Surg Endosc. (2018) 32(2):983–9. doi: 10.1007/s00464-017-5776-6
PubMed Abstract | Crossref Full Text | Google Scholar
10. Badic B, Gancel CH, Thereaux J, Joumond A, Bail JP, Meunier B, et al. Surgical and oncological long term outcomes of gastrointestinal stromal tumors (GIST) resection- retrospective cohort study. Int J Surg. (2018) 53:257–61. doi: 10.1016/j.ijsu.2018.03.074
PubMed Abstract | Crossref Full Text | Google Scholar
11. Liao GQ, Chen T, Qi XL, Hu YF, Liu H, Yu J, et al. Laparoscopic management of gastric gastrointestinal stromal tumors: a retrospective 10-year single-center experience. World J Gastroentero. (2017) 23(19):3522–9. doi: 10.3748/wjg.v23.i19.3522
Crossref Full Text | Google Scholar
12. Piessen G, Lefevre JH, Cabau M, Duhamel A, Behal H, Perniceni T, et al. Laparoscopic versus open surgery for gastric gastrointestinal stromal tumors: what is the impact on postoperative outcome and oncologic results? Ann Surg. (2015) 262(5):831–9, 829–40. doi: 10.1097/SLA.0000000000001488
PubMed Abstract | Crossref Full Text | Google Scholar
13. von Mehren M, Randall RL, Benjamin RS, Boles S, Bui MM, Ganjoo KN, et al. Soft tissue sarcoma, version 2.2018, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Ne. (2018) 16(5):536–63. doi: 10.6004/jnccn.2018.0025
Crossref Full Text | Google Scholar
14. Ozcan O, Kaplan M, Yalcin HC. Laparoscopic organ-preserving gastric resection improves the quality of life in stromal tumor patients an observational study with 23 patients. Ann Ital Chir. (2019) 90:41–51. PMID: 30638185.30638185
PubMed Abstract | Google Scholar
15. Briggler AM, Graham RP, Westin GF, Folpe AL, Jaroszewski DE, Okuno SH, et al. Clinicopathologic features and outcomes of gastrointestinal stromal tumors arising from the esophagus and gastroesophageal junction. J Gastrointest Oncol. (2018) 9(4):718–27. doi: 10.21037/jgo.2018.04.06
PubMed Abstract | Crossref Full Text | Google Scholar
16. Privette A, McCahill L, Borrazzo E, Single RM, Zubarik R. Laparoscopic approaches to resection of suspected gastric gastrointestinal stromal tumors based on tumor location. Surg Endosc. (2008) 22(2):487–94. doi: 10.1007/s00464-007-9493-4
PubMed Abstract | Crossref Full Text | Google Scholar
17. Maggioni C, Shida A, Mancini R, Ioni L, Pernazza G. Safety profile and oncological outcomes of gastric gastrointestinal stromal tumors (GISTs) robotic resection: single center experience. Int J Med Robot Comp. (2019) 15(6):e2031. doi: 10.1002/rcs.2031
Crossref Full Text | Google Scholar
18. Shi F, Li Y, Pan Y, Sun Q, Wang G, Yu T, et al. Clinical feasibility and safety of third space robotic and endoscopic cooperative surgery for gastric gastrointestinal stromal tumors dissection: a new surgical technique for treating gastric GISTs. Surg Endosc. (2019) 33(12):4192–200. doi: 10.1007/s00464-019-07223-w
PubMed Abstract | Crossref Full Text | Google Scholar
19. Desiderio J, Trastulli S, Cirocchi R, Boselli C, Noya G, Parisi A, et al. Robotic gastric resection of large gastrointestinal stromal tumors. Int J Surg. (2013) 11(2):191–6. doi: 10.1016/j.ijsu.2013.01.002
PubMed Abstract | Crossref Full Text | Google Scholar
20. Lwin TM, Fong ZV, Narayan RR, Wang SJ, Wang J. Robotic function-preserving resection of gastric gastrointestinal stromal tumor. J Surg Res. (2023) 290:164–70. doi: 10.1016/j.jss.2023.04.021
PubMed Abstract | Crossref Full Text | Google Scholar
21. Fletcher CD, Berman JJ, Corless C, Gorstein F, Lasota J, Longley BJ, et al. Diagnosis of gastrointestinal stromal tumors: a consensus approach. Hum Pathol. (2002) 33(5):459–65. doi: 10.1053/hupa.2002.123545
PubMed Abstract | Crossref Full Text | Google Scholar
23. Al-Thani H, El-Menyar A, Mekkodathil A, Elgohary H, Tabeb AH. Robotic management of gastric stromal tumors (GIST): a single middle eastern center experience. Int J Med Robot Comp. (2017) 13(1). doi: 10.1002/rcs.1729
Crossref Full Text | Google Scholar
24. Yeh CN, Hwang TL, Huang CS, Lee PH, Wu CW, Chen-Guo K, et al. Clinical practice guidelines for patients with gastrointestinal stromal tumor in Taiwan. World J Surg Oncol. (2012) 10:246. doi: 10.1186/1477-7819-10-246
PubMed Abstract | Crossref Full Text | Google Scholar
25. Solaini L, Cavaliere D, Fico V, Milone M, De Pascale S, Desiderio J, et al. Open versus laparoscopic versus robotic gastric gastrointestinal stromal tumour resections: a multicentre cohort study. Int J Med Robot Comp. (2021) 17(2):e2198. doi: 10.1002/rcs.2198
Crossref Full Text | Google Scholar
26. Kanehira E, Kanehira AK, Tanida T, Takahashi K, Obana Y, Sasaki K. CLEAN-NET: a modified laparoendoscopic wedge resection of the stomach to minimize the sacrifice of innocent gastric wall. Surg Endosc. (2020) 34(1):290–7. doi: 10.1007/s00464-019-06765-3
PubMed Abstract | Crossref Full Text | Google Scholar
27. Song J, Oh SJ, Kang WH, Hyung WJ, Choi SH, Noh SH. Robot-assisted gastrectomy with lymph node dissection for gastric cancer: lessons learned from an initial 100 consecutive procedures. Ann Surg. (2009) 249(6):927–32. doi: 10.1097/01.sla.0000351688.64999.73
PubMed Abstract | Crossref Full Text | Google Scholar
28. Ceccarelli G, Costa G, De Rosa M, Codacci PM, Frezza B, De Prizio M, et al. Minimally invasive approach to gastric GISTs: analysis of a multicenter robotic and laparoscopic experience with literature review. Cancers (Basel). (2021) 13(17). doi: 10.3390/cancers13174351
Crossref Full Text | Google Scholar
29. Otani Y, Furukawa T, Yoshida M, Saikawa Y, Wada N, Ueda M, et al. Operative indications for relatively small (2–5 cm) gastrointestinal stromal tumor of the stomach based on analysis of 60 operated cases. Surgery. (2006) 139(4):484–92. doi: 10.1016/j.surg.2005.08.011
留言 (0)