
記住我









Viral myocarditis is an important cause of acute cardiomyopathy resulting from inflammatory destruction of the myocardium (1). Enteroviruses, such as coxsackie B virus, are recognized as a common causal agent of acute myocarditis. Multiple clinical manifestations have been reported, including signs of acute heart failure, cardiogenic shock, and ventricular arrhythmias (2). The natural history of myocarditis is often unpredictable. Patients may experience an acute recovery of left ventricular systolic function, develop chronic and irreversible cardiomyopathy, or face fulminant disease resulting in acute cardiogenic shock and death. The diagnosis of clinically suspected myocarditis relies on a compatible clinical presentation with noninvasive diagnostic findings (3). Cardiac biomarkers including troponin I and troponin T may be elevated in cases of myocarditis, with increased levels associated with a worse prognosis (4). Electrocardiogram changes include sinus tachycardia, atrioventricular block, nonspecific ST-wave and T-wave abnormalities, and ST-segment elevation mimicking an acute myocardial infarction (5). Echocardiographic findings vary depending on the timing of the patient's presentation, often demonstrating new segmental or global wall motion abnormalities (3). Second-level investigations include cardiovascular magnetic resonance (CMR), coronary angiography to exclude ischemic cardiomyopathy, and endomyocardial biopsy (EMB). CMR serves as a highly specific, noninvasive diagnostic tool to characterize myocardial tissue, with the ability to detect inflammation, necrosis, fibrosis, and edema (1). Limitations of CMR include its inability to detect the degree of myocardial inflammation and cannot be used to exclude viral myocarditis (1, 3). Although EMB remains the gold standard for a definitive diagnosis, it is not routinely performed in patients with a clinical suspicion of myocarditis due to the lack of clinical value for guiding treatment or determining prognosis except in unique circumstances (6). Herein, we report a series of three cases with clinically suspected viral myocarditis.
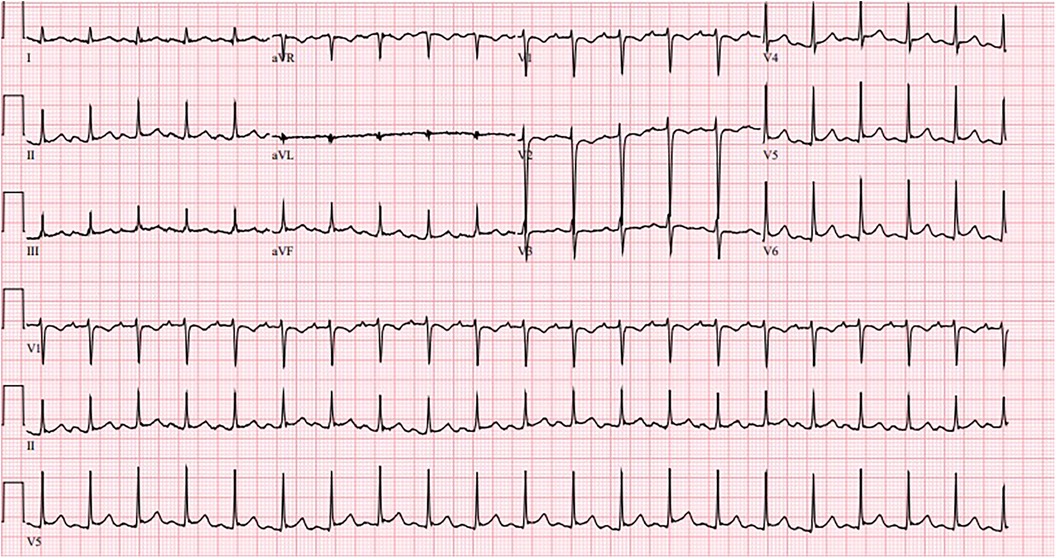
Case presentation Patient 1A 19-year-old male with no significant past medical history presented with five days of persistent nonbilious, non-bloody vomiting and worsening abdominal pain. Initial vital signs were significant for a temperature of 98.2°F, blood pressure of 80/47 mmHg, heart rate of 124/min, and oxygen saturation of 93% on room air. Electrocardiogram (EKG) showed sinus tachycardia without significant ST segment or T wave changes (Figure 1). Initial troponin was elevated at 2.15 ng/ml (N: < 0.012 ng/ml). Computed tomography (CT) of the abdomen without contrast was unremarkable. CT of the chest without contrast showed bilateral pulmonary edema. The patient was upgraded to the intensive care unit (ICU) due to suspected cardiogenic shock and started on vasopressors including norepinephrine and dobutamine. Echocardiogram showed a left ventricular ejection fraction (LVEF) of 20%–24% with severe global hypokinesis. Reverse transcription polymerase chain reaction for SARS-CoV-2 was negative. On day 3, the patient was weaned off vasopressors. Coronary angiography was deferred due to the absence of risk factors for coronary artery disease and the absence of ischemic changes on EKG. Serum coxsackievirus B (serotypes 1, 2, 5, and 6) IgG and IgM antibodies were positive. On day 6, the patient was initiated on a low dose of carvedilol and lisinopril. A repeat echocardiogram showed improvement of LVEF to 50%–54%. The patient had resolution of symptoms and he was stable for hospital discharge. Two weeks following hospitalization, the patient had achieved complete clinical recovery.
Figure 1. Sinus tachycardia without significant ST segment or T wave changes.
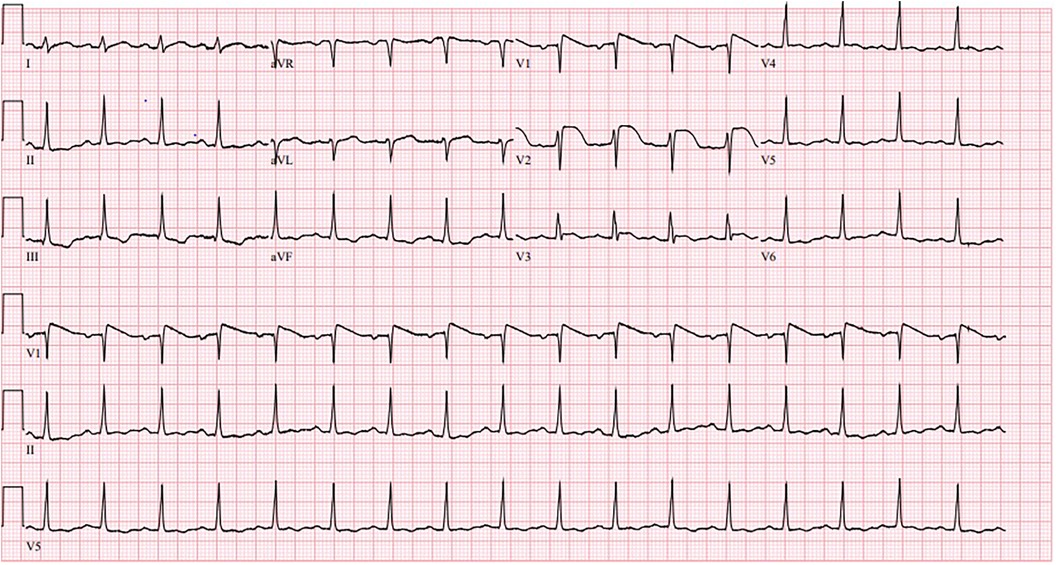
Patient 2A 20-year-old female with no significant past medical history presented with chest pain, dizziness, and epigastric pain. Initial vital signs were notable for a temperature of 98.2°F, blood pressure of 63/39 mmHg, heart rate of 106/min, and oxygen saturation of 100% on room air. Physical exam was benign except for abdominal tenderness in the epigastric region. The patient remained hypotensive and was admitted to the ICU for vasopressor support. EKG on admission showed acute ST segment elevations in leads V1 and V2 (Figure 2). Initial labs were notable for a creatinine of 4.6 mg/dl and an elevated troponin of 0.6 ng/ml (N: < 0.012 ng/ml). A transthoracic echocardiogram showed an LVEF of 25%–29% and diffuse hypokinesis with right ventricular dysfunction. The patient required dobutamine and norepinephrine for cardiogenic shock. Right and left heart catheterization with coronary angiography showed no significant coronary artery disease, normal pulmonary pressures, and normal cardiac output. On day 4, repeat EKG showed normal sinus rhythm with resolution of ST elevations, and the patient no longer required inotropic support. Serum coxsackievirus group B (serotypes 1–6) IgG and IgM antibodies was positive. Low dose sacubitril/valsartan and carvedilol was initiated on day 6 of hospitalization. Additional guideline directed medical therapy for heart failure was withheld due to low blood pressure measurements. She was stable for discharge on day 7 of hospitalization. Upon 1 month follow up, a repeat echocardiogram demonstrated a normal LVEF and no wall motion abnormalities.
Figure 2. Normal sinus rhythm with ST segment elevations in leads V1 and V2.
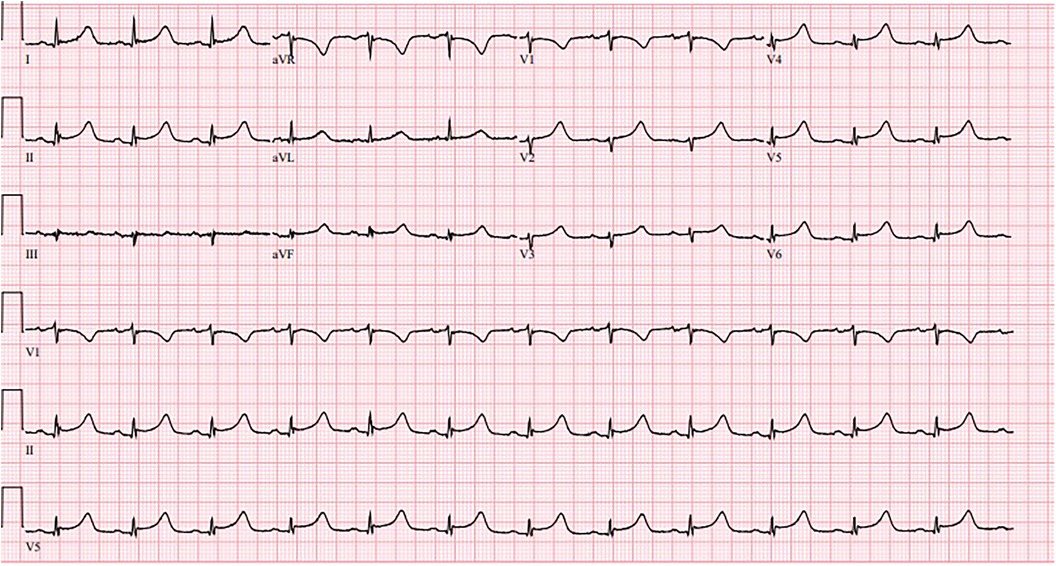
Patient 3A 78-year-old female with a history of hypertension, type 2 diabetes, and chronic hyponatremia presented with new onset dizziness and weakness. On admission, vital signs were notable for a temperature of 98.9°F, blood pressure of 70/40 mmHg, heart rate of 87 /min, and oxygen saturation of 99% on room air. Physical exam was notable for bilateral lower extremity pitting edema but otherwise unremarkable. EKG showed a normal sinus rhythm with nonspecific ST-segment changes (Figure 3). Initial troponin was 10.7 ng/ml (N: < 0.012 ng/ml). A transthoracic echocardiogram demonstrated a reduced LVEF of 40%–44% with hypokinesis of the anteroseptal and apical myocardium. A left heart catheterization showed twenty to thirty percent proximal and mid left anterior descending artery (LAD) stenosis which did not warrant intervention. Serum coxsackievirus group B (serotype 3) IgM and IgG antibody was positive. Hypotension improved with intravenous fluids. After nine days of hospitalization, the patient reported complete resolution of symptoms. She was continued on losartan and metoprolol with close outpatient follow up. Three months following admission, a repeat echocardiogram showed recovery of ventricular function with a LVEF of 60%–65%.
Figure 3. Normal sinus rhythm with nonspecific ST-segment changes.
DiscussionWe highlight three unique cases of clinically suspected myocarditis with positive coxsackievirus B antibodies. Despite an initial presentation of cardiogenic shock, there was rapid clinical recovery within a week of hospitalization. The diagnosis of myocarditis relies on clinical presentations resembling acute coronary syndrome, nonspecific ST segment and T wave changes on ECG, followed by unexplained left ventricular dysfunction with either regional or global wall motion abnormalities on echocardiogram. Our first two cases consisted of healthy, young patients with no cardiovascular risk factors who prompted an investigation for new onset non-ischemic cardiomyopathy (NICM). In our third case, an elderly patient with multiple cardiovascular comorbidities, highly elevated troponin and nonspecific ischemic changes on ECG highlighted the importance of excluding coronary artery disease.
There were several limitations in our cases. First, endomyocardial biopsy was not performed during hospitalization due to the resolution of symptoms and improvement in LVEF within days of starting heart failure medical therapy. EMB is generally reserved for patients with new-onset fulminant myocarditis refractory to pharmacologic therapy or unexplained heart failure associated with a dilated left ventricle, ventricular arrhythmias, and atrioventricular block (6). In addition, CMR was not available at our hospital, and could have served as a valuable noninvasive tool to support the diagnosis of clinically suspected myocarditis. We recognize the limitation of serum coxsackie antibodies in the diagnosis of coxsackie myocarditis and that a definite diagnosis requires viral PCR on cardiac biopsy.
Myocarditis causes an inflammatory cardiomyopathy leading to acute heart failure with risk of hemodynamic instability, often requiring temporary inotropic and vasopressor support (7). Depending on the degree of left ventricular dysfunction, patients may experience rapid resolution, chronic dilated cardiomyopathy, or end stage heart failure with risk of sudden cardiac death (3). Myocarditis can result from multiple infectious pathogens including viruses, bacteria, fungi, and protozoans (2). Parvovirus B19, human herpesvirus 6 (HHV 6), and enteroviruses, including coxsackie B virus, are common viral etiologies of acute and chronic myocarditis (2). The pathogenesis involves introduction of the virus through the respiratory or gastrointestinal tract followed by entry into the myocardium (1). Direct infection of cardiomyocytes enables viral replication and activates immune responses, resulting in myocyte necrosis and cellular degradation (8). In addition, molecular mimicry between cardiac and viral antigens triggers an autoimmune reaction in which virus specific T cells target the myocardium. Over time, a chronic inflammatory response causes myocyte fibrosis and cardiac remodeling, resulting in dilated cardiomyopathy (2). Progressive ventricular dysfunction is associated with persistent viral infection as demonstrated from an EMB based analysis of clinically suspected viral myocarditis (9).
Echocardiography is essential in the initial work-up to exclude other causes of NICM such as amyloidosis or valvular heart disease. Echocardiographic features are nonspecific and encompass a wide spectrum of findings. They often demonstrate a reduced LVEF with global hypokinesis, as seen in two of our patients. Right ventricular dysfunction, shown to be a prognostic factor for mortality and the need for transplantation, was observed in one of our cases (2). Other potential features include increased septal thickening, regional hypokinesis, diastolic dysfunction, or pericardial effusion (10). Such findings on echocardiography cannot reliably distinguish myocarditis from acute coronary syndrome. Therefore, cardiac catheterization is warranted when coronary artery disease is suspected.
Treatment recommendations for viral myocarditis are based on expert consensus centered on guideline-directed medical therapy for heart failure. No clinically approved antiviral therapies are available for coxsackie B-related myocarditis due to the absence of randomized clinical trials in the field. However, anti-viral agents such as interferon-β (IFN-β) have gained recent attention due to cardiomyocyte protection and decreased inflammatory cell infiltration, as demonstrated in an experimental animal model (11). In addition, a phase-II study from Schultheiss et al. showed effective viral clearance, reduction in viral load, and improvement in NYHA functional class among patients receiving IFN-β in addition to standard heart failure therapy (12). The role of immunomodulatory therapy remains largely exploratory. Given the role of the coxsackievirus-adenovirus receptor for myocardial viral entry, neutralization with soluble virus receptor traps can inhibit development of chronic myocarditis and preserve cardiac function, as demonstrated in an animal model (13). Further randomized clinical trials are required to determine the effect of antiviral and immunomodulatory therapy on multiple clinical endpoints.
ConclusionWe reported three cases of clinically suspected myocarditis requiring hemodynamic support. Serum coxsackie antibodies were positive in all patients. Patients hospitalized for left ventricular dysfunction secondary to acute myocarditis often have significant recovery within weeks. Clinical management for viral myocarditis centers on optimizing heart failure medical therapy. Given the possibility of progressive systolic dysfunction with viral persistence, close monitoring with long term follow up is required.
Data availability statementThe original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics statementWritten informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributionsJB: Writing – original draft, Writing – review & editing. HR: Writing – original draft, Writing – review & editing. SS: Writing – review & editing. ST: Writing – review & editing. JK: Writing – review & editing. AS: Writing – review & editing. MD: Writing – review & editing. SR: Writing – review & editing.
FundingThe author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interestThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's noteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary materialThe Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2024.1345449/full#supplementary-material
Supplementary Video 1
Echocardiogram of patient 1, short-axis view showing reduced LVEF with severe global hypokinesis.
Supplementary Video 2
Echocardiogram of patient 2, short-axis view showing reduced LVEF with diffuse hypokinesis.
Supplementary Video 3
Echocardiogram of patient 3, long-axis view showing reduced LVEF with anteroseptal hypokinesis.
1. Pollack A, Kontorovich AR, Fuster V, Dec GW. Viral myocarditis–diagnosis, treatment options, and current controversies. Nat Rev Cardiol. (2015) 12(11):670–80. doi: 10.1038/nrcardio.2015.108
PubMed Abstract | Crossref Full Text | Google Scholar
3. Caforio AL, Pankuweit S, Arbustini E, Basso C, Gimeno-Blanes J, Felix S, et al. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: a position statement of the European Society of Cardiology working group on myocardial and pericardial diseases. Eur Heart J. (2013) 34(33):2636–48. doi: 10.1093/eurheartj/eht210
PubMed Abstract | Crossref Full Text | Google Scholar
4. Smith SC, Ladenson JH, Mason JW, Jaffe AS. Elevations of cardiac troponin I associated with myocarditis. Experimental and clinical correlates. Circulation. (1997) 95(1):163–8. doi: 10.1161/01.CIR.95.1.163
PubMed Abstract | Crossref Full Text | Google Scholar
5. Dec GW Jr, Waldman H, Southern J, Fallon JT, Hutter AM Jr, Palacios I. Viral myocarditis mimicking acute myocardial infarction. J Am Coll Cardiol. (1992) 20(1):85–9. doi: 10.1016/0735-1097(92)90141-9
PubMed Abstract | Crossref Full Text | Google Scholar
6. Cooper LT, Baughman KL, Feldman AM, Andrea F, Mariell J, Uwe K, et al. The role of endomyocardial biopsy in the management of cardiovascular disease: a scientific statement from the American heart association, the American college of cardiology, and the European Society of Cardiology. Endorsed by the heart failure society of America and the heart failure association of the European Society of Cardiology. J Am Coll Cardiol. (2007) 50(19):1914–31. doi: 10.1016/j.jacc.2007.09.008
PubMed Abstract | Crossref Full Text | Google Scholar
7. Veronese G, Ammirati E, Cipriani M, Frigerio M. Fulminant myocarditis: characteristics, treatment, and outcomes. Anatol J Cardiol. (2018) 19(4):279–86. doi: 10.14744/AnatolJCardiol.2017.8170
PubMed Abstract | Crossref Full Text | Google Scholar
8. Kandolf R, Ameis D, Kirschner P, Canu A, Hofschneider PH. In situ detection of enteroviral genomes in myocardial cells by nucleic acid hybridization: an approach to the diagnosis of viral heart disease. Proc Natl Acad Sci U S A. (1987) 84(17):6272–6. doi: 10.1073/pnas.84.17.6272
PubMed Abstract | Crossref Full Text | Google Scholar
9. Kühl U, Pauschinger M, Seeberg B, Lassner D, Noutsias M, Poller W, et al. Viral persistence in the myocardium is associated with progressive cardiac dysfunction. Circulation. (2005) 112(13):1965–70. doi: 10.1161/CIRCULATIONAHA.105.548156
Crossref Full Text | Google Scholar
10. Ammirati E, Frigerio M, Adler ED, Basso C, Birnie DH, Brambattiet M, et al. Management of acute myocarditis and chronic inflammatory cardiomyopathy: an expert consensus document. Circ Heart Fail. (2020) 13(11):e007405. doi: 10.1161/CIRCHEARTFAILURE.120.007405
PubMed Abstract | Crossref Full Text | Google Scholar
11. Wang YX, da Cunha V, Vincelette J, White K, Velichko S, Xu Y, et al. Antiviral and myocyte protective effects of murine interferon-beta and -{alpha}2 in coxsackievirus B3-induced myocarditis and epicarditis in balb/c mice. Am J Physiol Heart Circ Physiol. (2007) 293(1):H69–76. doi: 10.1152/ajpheart.00154.2007
PubMed Abstract | Crossref Full Text | Google Scholar
12. Schultheiss HP, Piper C, Sowade O, Waagstein F, Kapp JF, Wegscheider K, et al. Betaferon in chronic viral cardiomyopathy (BICC) trial: effects of interferon-β treatment in patients with chronic viral cardiomyopathy. Clin Res Cardiol. (2016) 105(9):763–73. doi: 10.1007/s00392-016-0986-9
PubMed Abstract | Crossref Full Text | Google Scholar
13. Pinkert S, Dieringer B, Klopfleisch R, Savvatis K, Linthout SV, Pryshliak M, et al. Early treatment of coxsackievirus B3-infected animals with soluble coxsackievirus-adenovirus receptor inhibits development of chronic coxsackievirus B3 cardiomyopathy. Circ Heart Fail. (2019) 12(11):e005250. doi: 10.1161/CIRCHEARTFAILURE.119.005250
留言 (0)