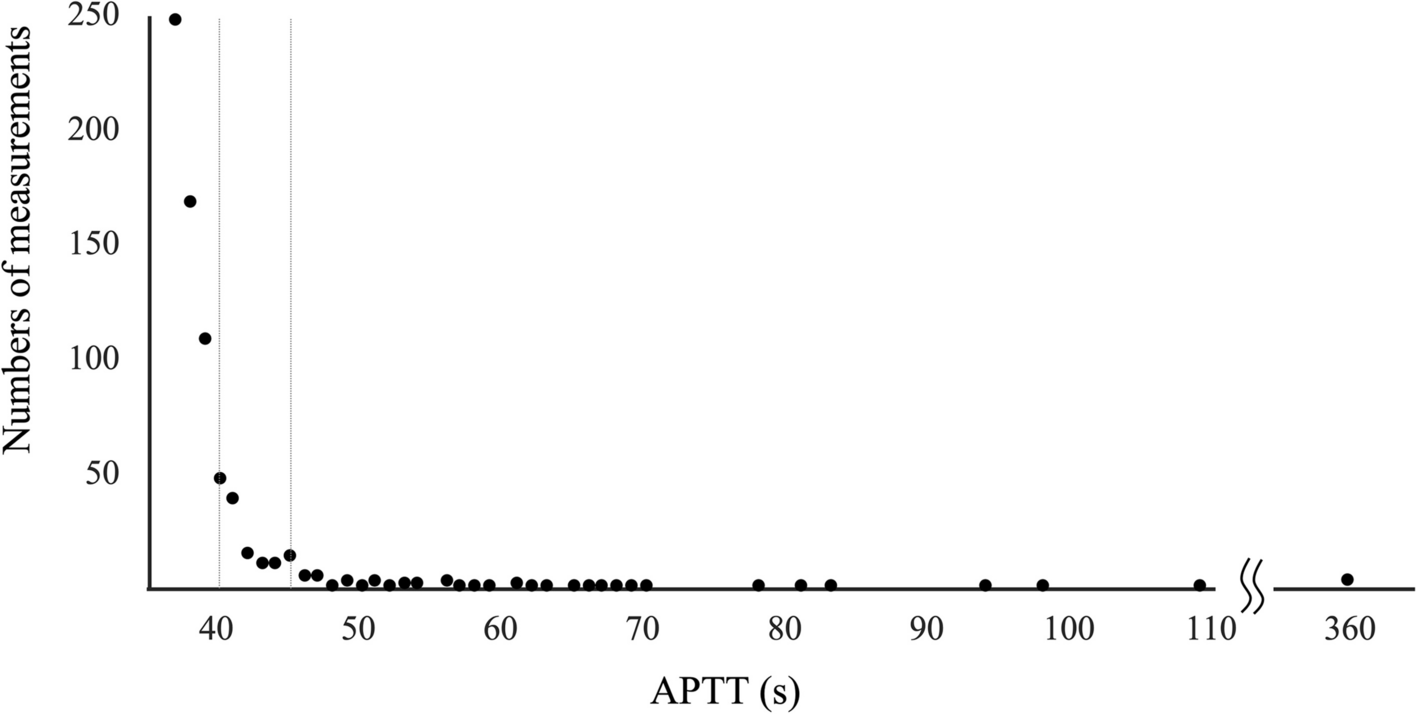
To the best of our knowledge, this is the largest retrospective study addressing the prevalence of isolated APTT prolongation in Japanese surgical patients. In our study, 725 (6.8%) of 10,684 measurements indicated isolated APTT prolongation.
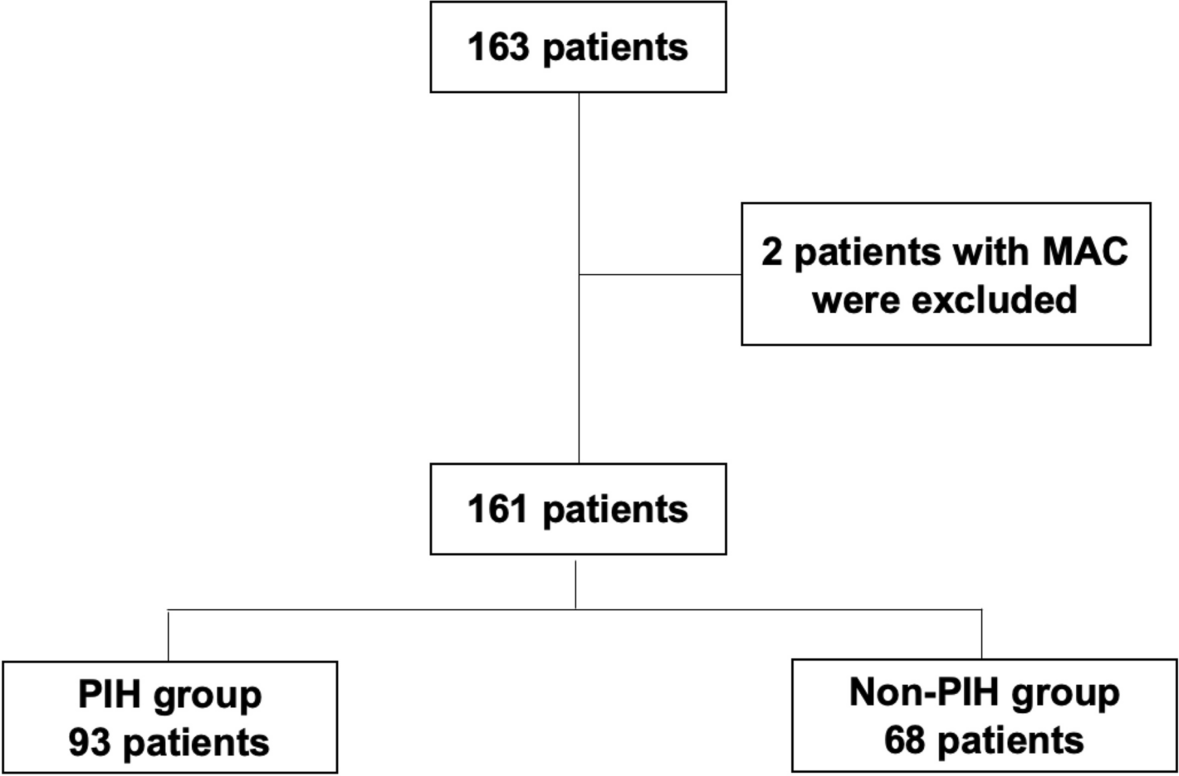
Although routine coagulation screening tests prior to surgery are not recommended, it has been suggested that preoperative history taking without hematologic evaluation may underestimate the prevalence of bleeding disorders, leading to perioperative morbidity and mortality [11]. In our practice, preoperative coagulation tests were conducted for all patients who presented to the anesthetic department, contributing to the elimination of selection bias.
The frequency of isolated prolongation of APTT in our study was considerably lower than that recently reported (i.e., isolated prolongation of APTT ≥ 38 s corresponded to 12.1% of the APTT measurements accompanied by a normal prothrombin time and/or PT-INR < 1.2) [9]. The Danish study investigated 18,642 samples from 10,697 patients (1–56 samples/patient), suggesting that multiple samples were collected from a significant number of patients. In our cohort, multiple measurements were confirmed in 2327 samples from 1056 patients (i.e., 2–8 samples from one patient), and the residual 8357 measurements were sampled from the same number of 8357 patients. It can be postulated that data collection differences may have resulted in a discrepancy with our results. In contrast, another Italian retrospective study demonstrated that 463 (5.74%) of 8069 adults undergoing elective surgery had prolonged APTT [8], which is comparable to our data. In our present study, isolated prolongation of APTT was detected more frequently in the measurements of patients undergoing elective surgery compared with those undergoing emergency surgery (657 [7.03%] of 9349 measurements vs 68 [5.09%] of 1335 measurements; p < 0.05). The exact reason is unclear; however, it is possible that emergency surgeries had been deferred or even canceled because of severe coagulation abnormalities before they were presented to the anesthetic department.
Special attention should be paid to the five cases wherein surgery was canceled due to isolated APTT prolongation. All but one patient demonstrated severely prolonged APTT. The patients with antiphospholipid antibody positivity and coagulation factor XII deficiency did not demonstrate bleeding tendencies [12]; nevertheless, surgeries were canceled entirely at the surgeon’s discretion. The others with coagulation factor VIII deficiency, hypofibrinogenemia [13], and unknown etiology exhibited a prolonged bleeding time and clinical signs of bleeding tendency. Particularly, in the case with hypofibrinogenemia, the transfusion of fresh frozen plasma minimally contributed to the increase in plasma fibrinogen levels. Thus, the decision to cancel surgery was based on a multidisciplinary evaluation of the patient.
The present study had several limitations. First, this study was a single-center study, and the measurements were mostly obtained from adult patients. Our findings should be interpreted within the context; however, we believe that our large-scale investigation provided a significant dataset regarding the isolated APTT prolongation in Japanese patients undergoing surgery. Second, due to the retrospective nature of our study, the etiology was not fully elucidated in patients with severely prolonged APTT. Practically, investigating every patient presenting with an isolated, severely prolonged APTT was challenging, as not all such patients had the time to afford scrutiny. However, our finding that the presence of antiphospholipid antibodies was the most frequently detected etiology was partly consistent with previously reported results [14,15,16], supporting the validity of our data.





留言 (0)