

記住我







Esophageal cancer is the seventh-ranked cancer in the world with an incidence of 572,034 new cases, and the sixth in overall mortality with 508,585 deaths per year (1). Esophagectomy remains the only potentially curative treatment option for patients with cancer invading more than mucosa. However, perioperative morbidity is still high with significant mortality, even in high-volume centers.
Although a multidisciplinary team is required during the perioperative treatment of esophageal cancer, adopted clinical pathways vary significantly between institutions. Changing these well-established and experience-based protocols is difficult. There is a growing interest related to the positive impact of Enhanced Recovery After Surgery (ERAS) protocol for esophagectomy on postoperative morbidity (1–4). However, ERAS is a challenging protocol requiring close work of surgeons and anesthesiologists, along with nurses and physiotherapists. The role of an anesthesiologist during the perioperative period is one of the most important factors in the proper implementation of ERAS protocol for esophagectomy. Specific elements of ERAS protocol such as opioid-sparing anesthesia, intraoperative goal-directed therapy (GDT), and postoperative „near-zero “fluid balance should be implemented by well-trained, experienced, and dedicated anesthesiologist (4–8). A few studies investigate the impact of these elements and the role of the anesthesiologist in the ERAS protocol (3, 9–11). However, the implementations of these elements in the ERAS protocol have been still fully underexplored. We wanted to show the impact of the implementation of ERAS protocol with anesthesiologists’ elements as an important role in everyday practice on clinical outcomes following esophagectomy.
The aim of this study was to assess the impact of properly conducted ERAS protocol with specific emphasis on fluid management (GDT and “near-zero” fluid balance) and opioid-sparing anesthesia on postoperative morbidity and mortality after esophagectomy, and to compare it with the usual clinical pathway.
2 Methods 2.1 Study populationThis is a single-center clinical retrospective observational study. All consecutive patients undergoing elective esophagectomy for esophageal adenocarcinoma (EAC) or squamocellular carcinoma (SCC) at Hospital for Digestive Surgery, University Clinical Center of Serbia, from December 2017 to March 2021, were assessed for eligibility. Patients between 18 and 80 years old with gastric conduit reconstruction after esophagectomy were included. Exclusion criteria were chronic renal failure with permanent hemodialysis, and loss to complete follow-up. The present study was approved by the Ethical Committee of the University Clinical Center Serbia (number 88/46). Written informed consent was obtained from all study participants. This manuscript adheres to the applicable Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.
Patients were divided into two groups according to the implementation of the ERAS protocol. Patients with completed ERAS protocol were assigned to the ERAS group, and patients with standard care after esophagectomy were assigned to the control group. Anesthesia and postoperative treatment in the ERAS group were delivered and guided by three anesthesiologists, previously trained in ERAS protocol and using goal-directed therapy monitoring, from January 2017 to November 2017. This period known as the learning and implementation curve was not included in the study. Standard of care anesthesia was performed by all other anesthesiologists, and postoperative treatment was performed by a surgeon in the control group. Patients were assigned to the ERAS group or the control group the day before planned surgery according to the schedule of attending anesthesiologist in the operating room. An anesthesiologist’s schedule for the operating room was made randomly.
A subtotal esophagectomy and gastric conduit reconstruction by intrathoracic (Ivor Lewis) or cervical esophago-gastric anastomosis (McKeown) were performed in all patients. In a few cases lower intrathoracic esophago-gastric anastomosis was created according to Garlock-Sweet, directly influenced by conduit vascularization. The surgical approach was open or minimally invasive. The minimally invasive approach included a hybrid procedure (laparoscopy followed by right thoracotomy) or total minimally invasive esophagectomy – tMIE (laparoscopy followed by thoracoscopy). Two-field standard lymphadenectomy was the standard of care. A median width of gastric conduit was preferable option, and a circular stapler was always used for performing esophago-gastric anastomosis in the upper mediastinum or a linear stapler in the neck. All surgical procedures were performed by experienced surgeons (volume over 20 esophagectomies per year per individual surgeon).
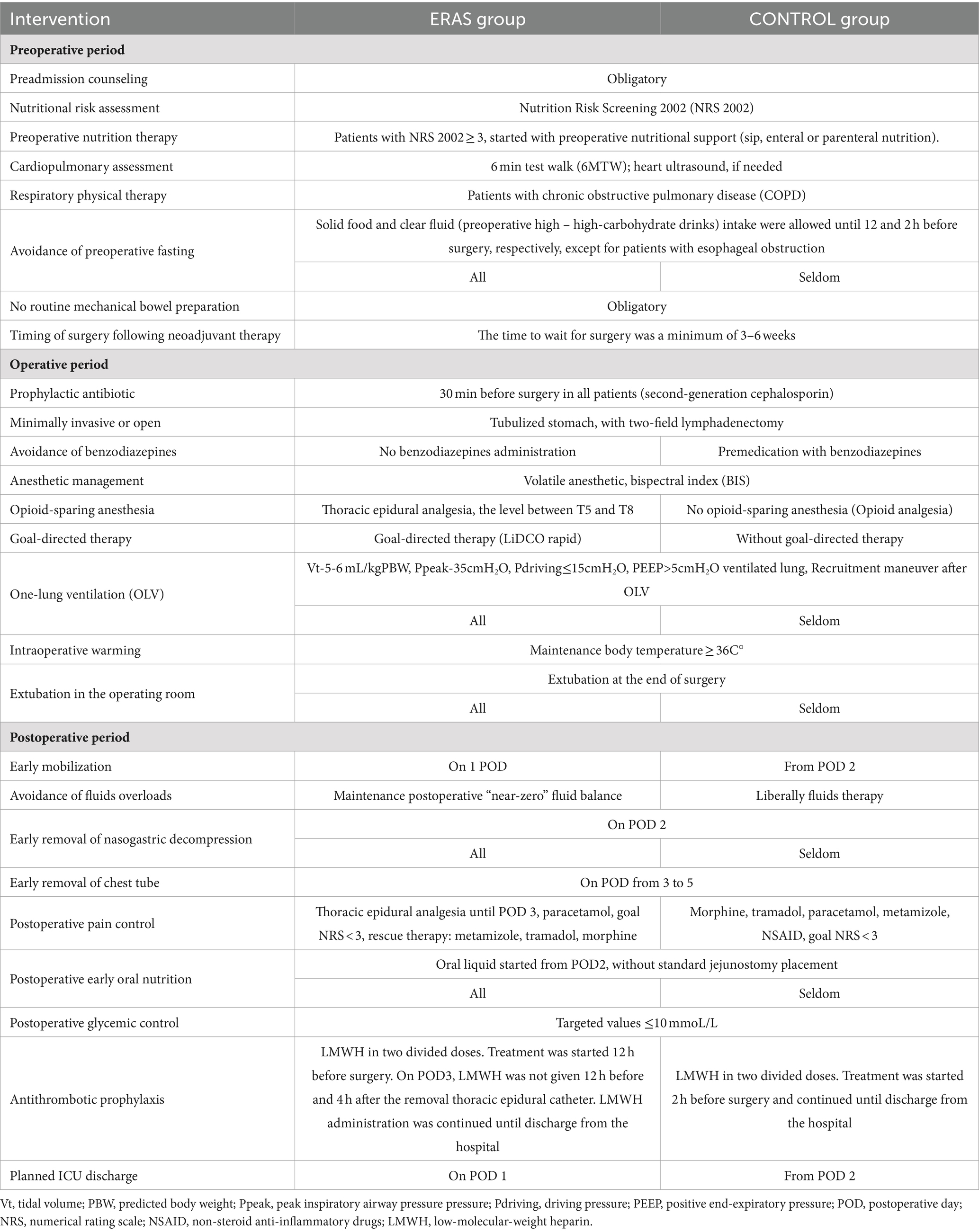
2.2 ERAS protocol and standard of care protocolIn our hospital, the ERAS protocol for esophagectomy was introduced in January 2017, but without implementation, all anesthesiologists’ elements (opioid-sparing anesthesia and fluid management) in all patients. Preadmission – evaluation by an anesthesiologist was obligatory for all patients. All preoperative, intraoperative, and postoperative components of ERAS protocol as well as our standard care are listed in Table 1. On admission, the Nutrition Risk Screening 2002 (NRS-2002) score was used for nutritional risk assessment of all patients. If the NRS-2002 score was ≥3, preoperative nutrition support was started. Oral nutrition supplements, enteral and/or parenteral nutrition were initiated depending on esophageal obstruction. Patients from both groups received 1,000 mL of Hartman solution on the day before surgery regardless of the permission to eat. In the ERAS group, thoracic epidural anesthesia was obligatory, except for those with absolute contraindication for epidural catheter placement. A thoracic epidural catheter was inserted before the induction of general anesthesia (Table 1). A test dose of 2 mL lidocaine 2% was administered for confirmation of accurate placement. In both groups of patients, general anesthesia was induced with propofol, fentanyl, and rocuronium, and maintained with sevoflurane. Depth of anesthesia was adjusted to bispectral index (BIS) to 40–60 in both groups. In ERAS group, after induction, a bolus of 5-10 mL levobupivacaine 0.25% was administered and intraoperative pain control was obtained with continuous epidural analgesia (levobupivacaine 0.125% + fentanyl 2mcg/mL), 5–12 mL/h, based on the patient’s weight and level of comfort. In control group or in case of absence of epidural catheter in patients in the ERAS group, intraoperative pain control was achieved with intravenous fentanyl boluses, based on the patient’s weight and needs for additional analgesia. Patients were ventilated with a tidal volume (Vt) of 7–8 mL/kg (ideal body weight) and PEEP≥5cmH2O. During the transthoracic procedure, one-lung ventilation (OLV) was applied whenever was tolerated by a patient. In the course of OLV, protective mechanical ventilation was provided (Table 1). The frequency of ventilation was controlled to the end-tidal carbon dioxide value of 3.5-6 kPa. An arterial line was inserted in all patients. Baseline Hartmann’s solution was administered at a rate of 3 mL/kg/h in the first hour in both groups with an intraoperative maintains fluid rate of 1 mL/kg/h. In the ERAS group, goal-directed therapy was provided by LiDCORapid™ (LiDCO Ltd., Cambridge, UK) after connection with the arterial line. Hemodynamic parameters – invasive arterial blood pressure (IABP), cardiac output (CO), cardiac index (CI), stroke volume (SV), stroke volume index (SVI), stroke volume variation (SVV), systemic vascular resistance (SVR) and systemic vascular resistance index (SVRI) were measured using LiDCORapid™. The goal was mean arterial pressure (MAP) ≥ 65 mmHg, SVV < 13% in the absence of arrhythmia or maintance SVI within 10% of baseline, respecting fluid tolerance. The fluid challenge with crystalloids (Hartmann’s solution 250 mL) was administered only MAP ≤65 mmHg and SVI decreased by 10% and more from baseline and SVV rose, without trying to achieve full fluid responsiveness. The administration algorithm for an albumin solution (5% 250 mL) was SVV > 13% in the abdominal phase of surgery or SVI < 33 mL/m2 in the thoracic phase of surgery. Fluid challenge was continued with crystalloids if SVV was still >13% after a bolus of albumin 5% or SVI was still <33 mL/m2. If MAP ≤65 mmHg, with stable baseline SVI and SVV < 10%, norepinephrine was administered. Before administration of norepinephrine, pneumothorax had to be excluded. In the control group, the goal of intraoperative hemodynamic management was maintained at MAP ≥65 mmHg while fluid administration or norepinephrine was dependent upon the attending anesthesiologist. At the end of the surgery, the patient was extubated whenever possible in both groups. In the ERAS group, postoperative care had to fulfill all elements from Table 1. In the control group, the standard of care was current practice in our hospital (Table 1). In the ERAS group, the postoperative goal was to keep the “near-zero” fluid balance, respecting MAP ≥65 mmHg, capillary refill <2 s, central venous oxygen saturation (ScvO2) ≥ 65%, and urine output ≥0.5 mL/kg/h. If needed, the vasopressor of choice was norepinephrine. In the control group, postoperative fluid therapy had been administered according to the individual judgment by the intensivist in charge in the ICU or attending surgeon in a ward, to achieve MAP ≥65 mmHg and urine output ≥0.5 mL/kg/h.
Table 1. Treatment protocol in ERAS and control group.
Postoperative fluid balance was carefully calculated taking into account fluids administered and eliminated through all routes, including blood loss and drainage. Daily fluid balance was calculated by subtracting the fluid eliminated from the total fluid administered from 05 h a.m. to 05 h a.m. the next day. The cumulative fluid balance at postoperative day (POD) 1 was calculated from induction of anesthesia to postoperative day 1 at 05 h, and the cumulative fluid balance at POD 2 was calculated from induction of anesthesia to POD 2 at 05 h.
2.3 OutcomesThe primary outcomes were a major morbidity within 30 days from surgery and 30-day and 90-day mortality.
Secondary outcomes were hospital and ICU length of stay (LOS), the incidence of interstitial pulmonary edema, major and minor postoperative pulmonary complications.
2.4 Definition of postoperative complicationsThe frequency of major morbidity, interstitial pulmonary edema, postoperative pneumonia, anastomotic leak, and other complications were followed during the first 30 days after surgery. 30-day and 90-day mortality was defined as any death relating to treatment within 30 and 90 days after surgery, respectively. Interstitial pulmonary edema was defined by chest x-ray and hypoxemia (peripheral blood saturation, SpO2 < 91%) in the absence of heart failure. Pneumonia was defined by current guidelines (12). All chest-x rays were examined and radiological diagnoses were made by the radiologist. Major postoperative pulmonary complications (PPC) were defined as pneumonia, acute respiratory distress syndrome, atelectasis, and pleural effusion, empyema or pneumothorax requiring intervention. A minor PPC were defined as atelectasis, pleural effusion or pneumothorax without requiring intervention. Surgical complications were listed as follows: anastomotic leak, gastric necrosis, bleeding, chylothorax, chylous effusion, or any need for surgery for reoperation (12). Major morbidity was presented by a number of patients with developed one or more major complications (major PPC, surgery complications, re-intubation, acute myocardial infarction, pulmonary embolism, renal failure requiring dialysis, sepsis, delirium, new-onset stroke, postoperative arrhythmia, and infection leading to prolonged hospital stay).
2.5 Statistics analysisDescriptive statistics were calculated for demographic characteristics, comorbidity, and other parameters (preoperatively and postoperatively) and were presented as frequencies and proportions. Numeric data were tested for normal distribution using the Kolmogorov–Smirnov test. The Mann–Whitney test was used to compare the nonparametric numeric data. Independent t-test was used to compare parametric numeric data. Categorical data were analyzed using the Pearson chi-square test. Univariable and multivariable logistic regression methods were used for statistical analysis of differences between groups with and without ERAS protocol. All test variables with a statistically significant p < 0.05 in the univariable model were included in the multivariable model. Statistical significance was considered at p < 0.05. Statistical analysis was performed using the IBP SPSS Statistics v28 (Statistical Package for Social Sciences, SPSS Inc., Chicago, Illinois).
3 ResultsDuring the study period, 157 patients who underwent esophagectomy for esophageal carcinoma were assessed for the current study. After excluding three patients older than 80 years, three patients with esophagectomy with colon conduit reconstruction, one patient with esophagectomy with gastric conduit reconstruction and simultaneous colon resection, and 8 patients with palliative surgery, 142 patients were included. According to predefined exclusion criteria, two patients with chronic renal failure on permanent hemodialysis and 19 patients lost from follow-up were excluded from further analysis. The remaining 121 patients were included in the final analysis and divided into two groups: the ERAS group (69 patients) and the control group (52 patients).
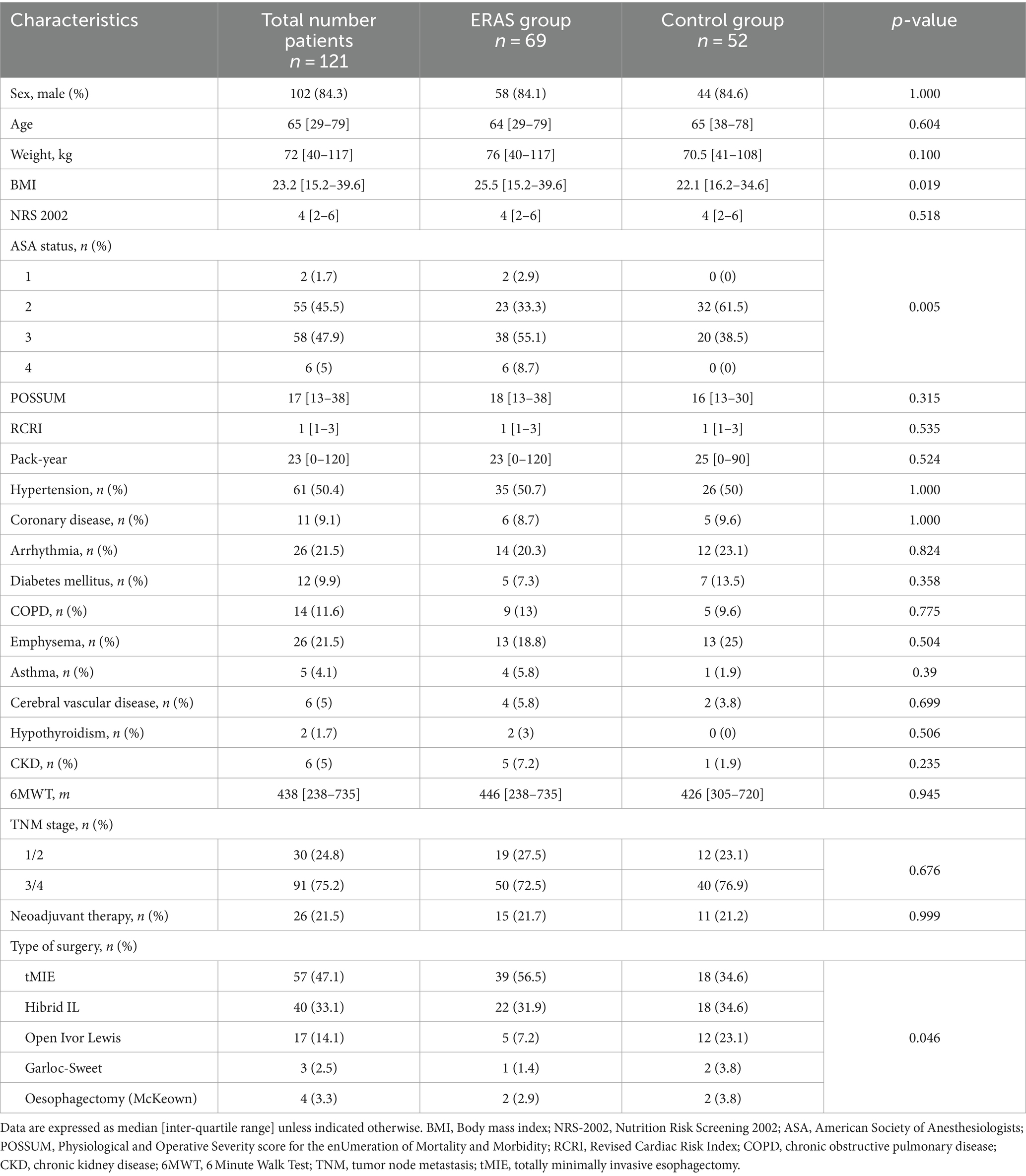
The distribution of the ASA (American Society of Anesthesiologists) score was different between groups – patients in the ERAS group were rated with a higher score (p = 0.005). BMI (Body Mass Index) was higher in the ERAS group (p = 0.019). The distribution of type of surgery (tMIE), Hybrid technics or open surgery was significantly different between groups (p = 0.046). Preoperative characteristics and the type of surgery are shown in detail in Table 2. The compliance rate to preoperative components of the ERAS protocol was 90.91%.
Table 2. Patients characteristics.
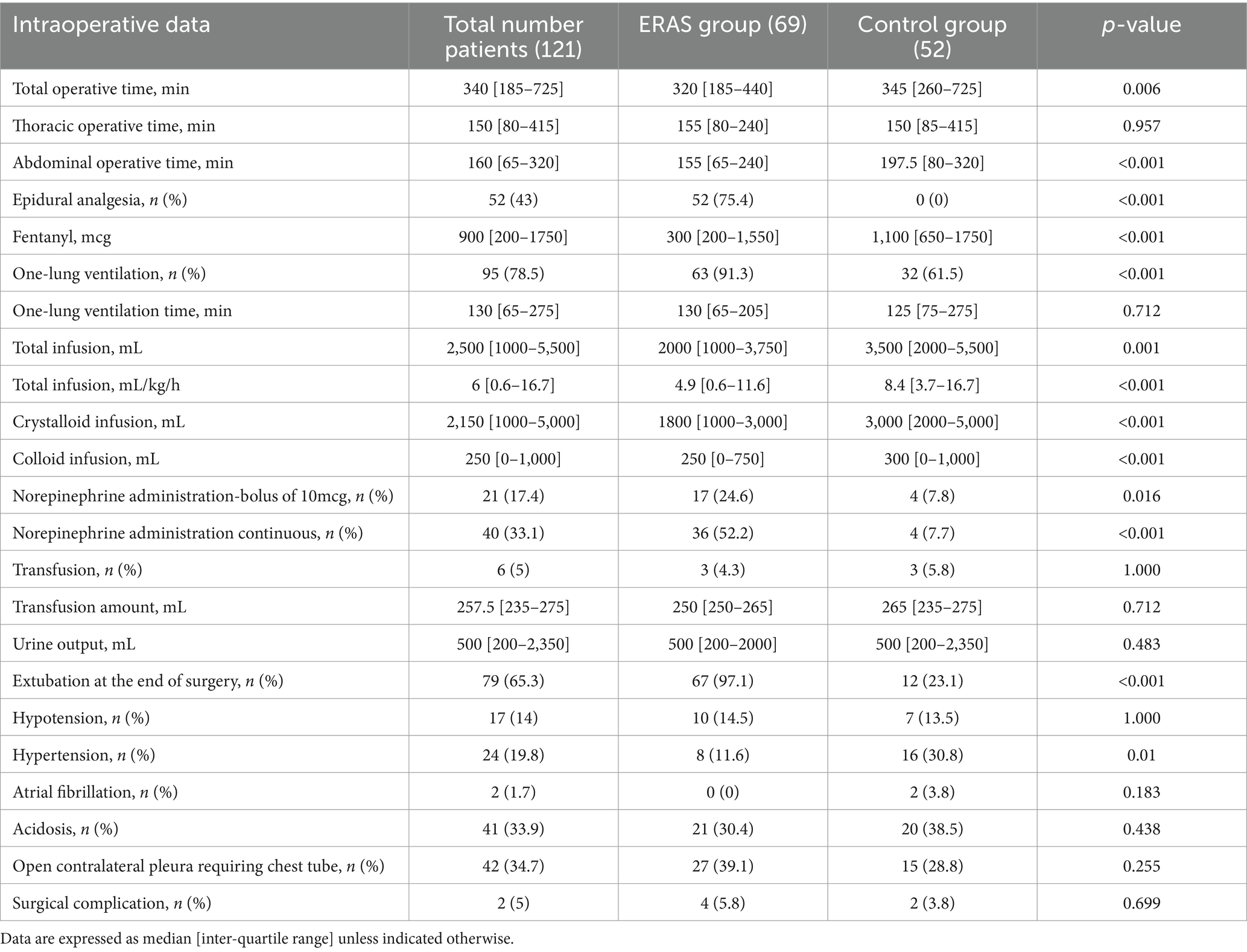
Total operative time was shorter in the ERAS group, median 320 (interquartile range, 185–440) minutes, than in the control group, median 345 (interquartile range, 260–275) minutes, p = 0.006. The median operative time of the abdominal phase was shorter in the ERAS group compared to the control group: 155 (interquartile range, 60–240) minutes vs. 197.5 (interquartile range, 80–320) minutes, p < 0.001. Thoracic epidural analgesia (TEA) was provided in 75.4% of patients in the ERAS group and no one from the control group received TEA. Intraoperative fentanyl administration was more common in the control, median 1,100 (interquartile range, 650–1750) mcg than in ERAS group, median 300 (interquartile range, 200–1,550) mcg, p < 0.001. One-lung ventilation was applied in 91.3% of patients in the ERAS group and in 61.5% in the control group (p < 0.001). Patients with fluid therapy guided by LIDCORapid (ERAS group) received lower fluids: median 2000 (interquartile range, 1,000–3,750) mL vs. median 3,500 (interquartile range, 2000–5,500) mL, p < 0.001, but intraoperative norepinephrine infusion was more administered in the patients in the ERAS group (52.2% vs. 7.7%, p < 0.001). The percentage of patients who were extubated immediately after surgical procedure was statistically higher in the ERAS group (97.1% vs. 23.1%, p < 0.001). Overall intraoperative data are presented in Table 3.
Table 3. Intraoperative data.
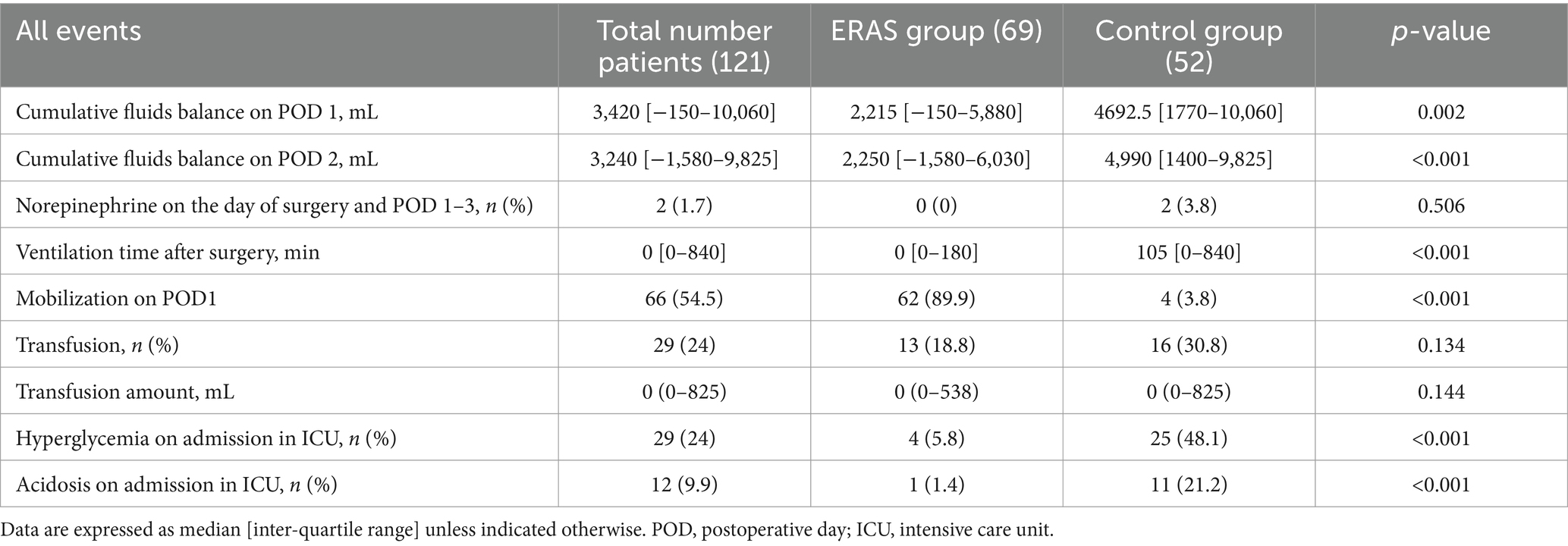
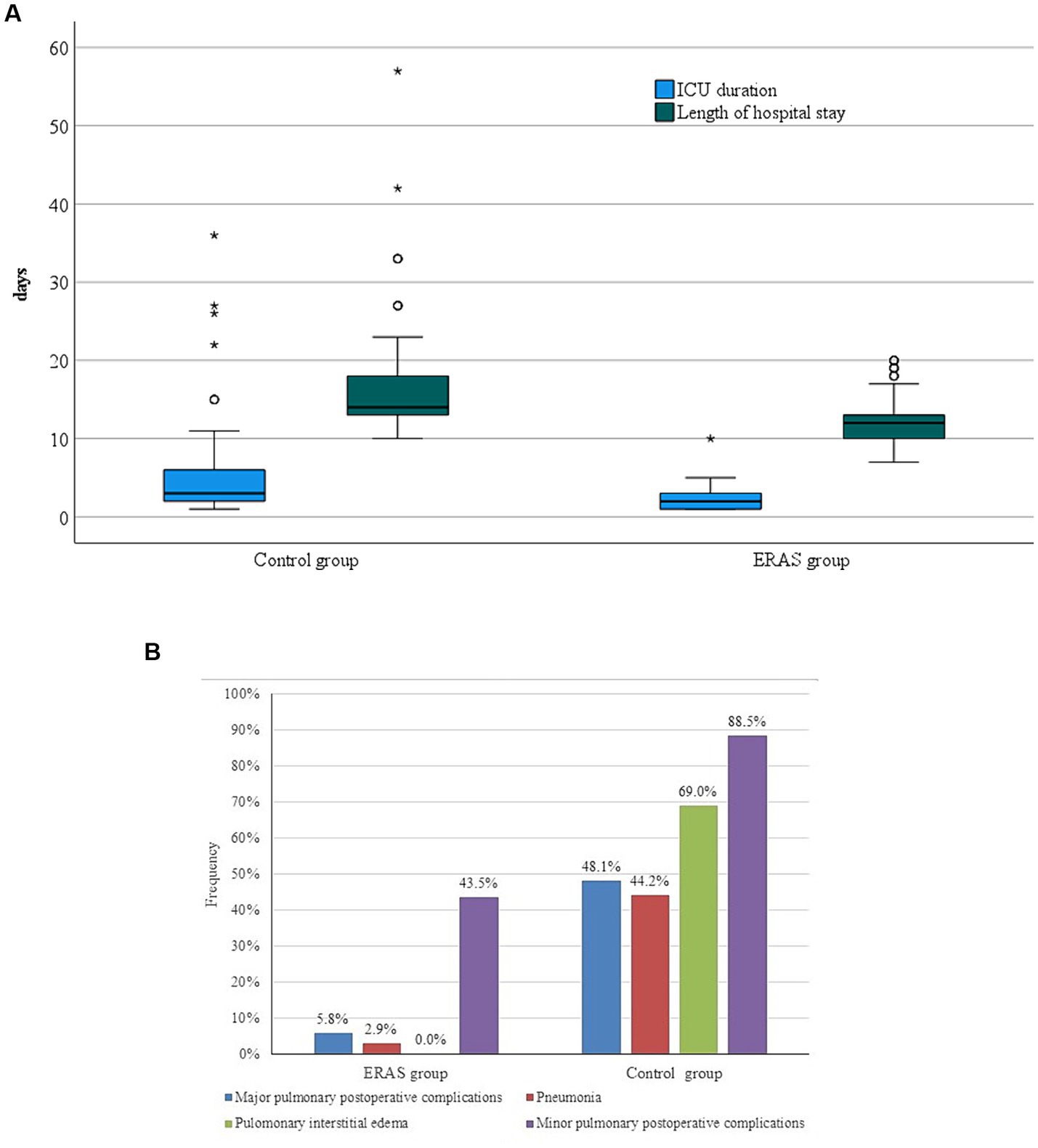
In the postoperative period, median cumulative fluid balance on POD1 was 2,215 (interquartile range, −150–5880) mL in the ERAS group vs. 4692.5 (interquartile range, 1770–10,060) mL in the control group, p = 0.002. There was a statistically significant difference in cumulative fluid balance on POD2 between groups, median 2,250 (interquartile range, −1,580–6030) mL in ERAS vs. median 4,990 (1400–9,825) mL in the control group (p < 0.001). None of patients from the ERAS group received norepinephrine postoperatively, while 2 patients received norepinephrine postoperatively in the control group. On POD1, 89.9% of patients in the ERAS group were mobilized in contrast 3.8% of patients in the control group (p < 0.001) (Table 4). Postoperative morbidity at day 30 were lower in the ERAS group than in the control group (18.8% vs. 75%, p < 0.001) (Table 5). There was no significant difference in 30-day and 90-day mortality between groups (p = 0.07 and p = 0.119, respectively). The length of hospital stay was significantly shorter in the ERAS group, median 12 (interquartile range, 7–20) days than in the control group, median 14 (interquartile range, 10–57) days, p < 0.001 (Figure 1A). Occurrence of interstitial pulmonary edema was significantly lower in the ERAS group (0%) compared to the control group (69%), p < 0.001. Pneumonia, major postoperative pulmonary complications (Figure 1B) and atrial fibrillation were lower in the ERAS group compared to the control group (2.9% vs. 44.2%, p < 0.001; 5.8% vs. 48.1%, p < 0.001; 5.8% vs. 19.2%, p = 0.041, respectively) (Table 5). Surgical complications were significantly less frequent in the ERAS group (2.9%) than in the control group (21.2%), p = 0.002. Anastomotic leakage was confirmed in 7 (13.5%) patients in the control group, while two of them were treated by surgery. There was no anastomotic leakage in the ERAS group. Postoperative bleeding requiring re-operation was registered in one patient in the control group (Table 5). Inguinal hernia incarceration treated by re-operation occurred in one patient from the ERAS group.
Table 4. Postoperative outcomes.
Table 5. Postoperative complications, mortality, ICU, and hospital stay.
Figure 1. (A) ICU duration and hospital stay between groups. (B) Postoperative pulmonary complications.
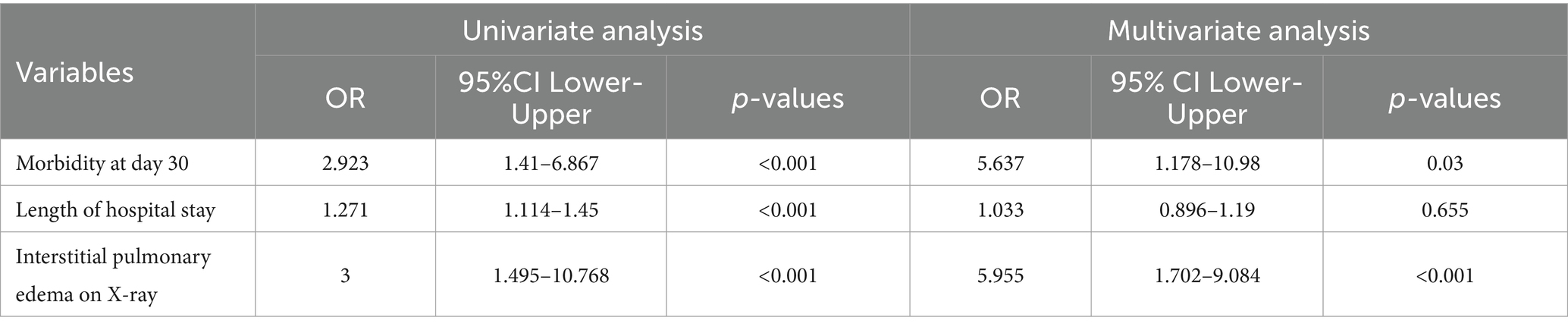
In the univariable analysis, patients from the control group were associated with a higher risk of 30-day morbidity (OR 2.923; CI95% 1.41–6.867; p < 0.001), prolonged length of hospital stay (OR 1.271; CI95% 1.114–1.45; p < 0.001) and interstitial pulmonary edema (OR 3; CI95% 1.495–10.768; p < 0.001). In the multivariable analysis, patients from the control group had about six times higher probability for 30-day morbidity (OR 5.637; CI95% 1.178–10.98; p = 0.03) and six times higher risk for interstitial pulmonary edema (OR 5.955; CI95% 1.702–9.084; p < 0.001) (Table 6).
Table 6. Univariable and multivariable analysis of complications after esophagectomy.
4 DiscussionSince the ERAS protocol for esophagectomy was introduced, many studies have proven its positive effect on postoperative outcomes. However, compliance with all the elements of this protocol for esophagectomy is difficult due to the complexity of surgery and postoperative care, and already established protocols in high-volume centers. In our study, the implementation of ERAS protocol following esophagectomy for cancer led to reduced 30-day postoperative morbidity, interstitial pulmonary edema, pneumonia, anastomotic leakage, ICU duration, and the hospital LOS in univariable analysis. However, multivariable analysis revealed a higher probability of major morbidity and interstitial pulmonary edema in patients from the control group. Tang and colleagues showed favorable short-term outcomes (hospital LOS, postoperative complications, hospitalization cost) following esophagectomy after implementation of ERAS protocol (3). However, the study comparing ERAS protocol with a modified analgesic regimen combined with perioperative GDT, and standard ERAS protocol did not affect the hospital LoS and the incidence of postoperative complications such as pneumonia and anastomotic leak (9).
The effects of intraoperative GDT are in the focus of research during the past few years. Excess fluid administration could lead to interstitial water retention and lung edema (13). In the randomized control trial by Mukai et al., the implementation of intraoperative GDT reduced overall morbidity and mortality, and shortened hospital stay, without effect on pneumonia and anastomotic leakage in patients after transthoracic esophagectomy (10). A lower incidence of pneumonia, shorter ICU stay were registered after GDT during esophagectomy in the study by Veelo et al., while length of hospital stay, overall morbidity and mortality were similar (14). In our study, ERAS protocol with intraoperative GDT and postoperative “near-zero” fluid balance reduced 30-day major morbidity and interstitial pulmonary edema, with no effect on the incidence of postoperative pneumonia. However, some studies and meta-analyses failed to show a positive impact of intraoperative GDT on the incidence of postoperative complications after surgery of the foregut (15–17). Total intraoperative infusion was significantly less in the ERAS group with intraoperative GDT. The present study showed that patients with TEA and GDT received less fluids despite epidural analgesia but more vasopressors intraoperatively than patients in the control group. Ischemic impact of vasopressors on a gastric conduit was previously described, with a strong recommendation against the application of these drugs during esophagectomy (18). Nevertheless, in more recent study, an intraoperative application of vasopressors was not associated with increased incidence of an anastomotic leak following open Ivor Lewis esophagectomy (19). Similarly, in our study, none of the patients in the ERAS group with intraoperative norepinephrine infusion developed an anastomotic leakage. At the end of the surgical procedure, norepinephrine was suspended in all patients in the ERAS group. Reasons for a good outcome may be found in intraoperative fluids optimization before starting intraoperative norepinephrine infusion due to hypotension, as a consequence of vasodilatation which is an adverse effect of TEA.
High positive cumulative postoperative balance on POD1 was found to be an independent risk factor for postoperative pulmonary complications in high-volume centers (11, 20). In the present study, the cumulative fluid balance on POD1 was significantly lower in the ERAS group than in the control group. In the study from Japan, positive fluid balance higher than 3,000 mL at POD 1 had a significantly negative impact on anastomotic leakage and postoperative pneumonia (21). Besides intraoperative GDT, this might be another explanation of why patients in the ERAS group experienced less postoperative interstitial pulmonary edema and major morbidity. Therefore, optimal perioperative fluid management including an intraoperative GDT and cumulative “near-zero” fluid balance during esophagectomy is one of the most important elements of ERAS protocol.
The fluid shift from intravascular to interstitial space due to endothelial glycocalyx damage is common during perioperative period, in particular in major surgery. The surgical stress causes release of inflammatory mediators (tumor necrosis factor α, interleukins, proteases). Moreover, during iatrogenic acute hypervolemia, atrial natriuretic peptide is released and may degrade endothelial glycocalyx further, increased vascular permeability and made fluid and protein shift from intravascular space toward the interstitium. To protect the endothelial glycocalyx, fluid should be administered carefully and only when relative hypovolemia arises. Intraoperative goal directed therapy may help anesthesiologist to administer fluid only when needed and start with vasopressors (norepinephrine) application early, but safely (22, 23). One-lung ventilation (ischemia–reperfusion injury) and two-field lymphadenectomy in combination with fluid overload could increase the risk for interstitial pulmonary edema and lung injury (24). In early postoperative period (48–72 h), neuroendocrine and metabolic effects on surgical stress are the most pronounced. Following esophagectomy, inflammatory cytokines are released which leads to vasodilatation and increased permeability of the endothelium, and resulting tissue edema, in particular lung edema. Protocol with postoperative “near-zero” fluid balance allow maintaining of euvolemia in the early postoperative period and may decrease postoperative interstitial pulmonary edema, and pneumonia. Postoperative continuous thoracic epidural analgesia up to 72 h may reduce the neuroendocrine stress response after surgery and together with optimal fluid management reduce incidence of postoperative complications (22, 23).
Interstitial pulmonary edema was presented as separately complication. We did not count interstitial pulmonary edema in major PPC, despite it should be according some guidelines, because we believe interstitial pulmonary edema is very important clinical finding, and warning sign we need to adjust current fluid management to prevent further complications (positive fluid balance has to change to zero or negative fluid balance).
In the present study, in ERAS group the postoperative pneumonia was diagnosed only in 2.9% patients with no interstitial pulmonary edema, which is very low incidence. In control group, incidence of pneumonia was 44.2 and 69% interstitial pulmonary edema. Casado et al. have been demonstrated that fluid excess during the perioperative period is a predictor of the development of respiratory complications following esophagectomy (13). However, according current guidelines, the diagnosis of pneumonia is complicated because it involves several pulmonary radiological features, hypoxemia and a high leucocyte count which may be related to postoperative inflammatory response to the surgery, not infection (25). It appears that interstitial pulmonary edema and hypoxemia in combination with postoperative leukocytosis could lead to a false positive diagnosis for pneumonia. This could be one of reason for high incidence of pneumonia in control group.
The next important step in ERAS protocol is adequate perioperative pain management with opioid-sparing anesthesia (3, 4, 26). Opioid-sparing anesthesia is supported in enhanced pathways to avoid adverse effects of opioids such as postoperative nausea and vomiting, intestinal paresis, prolonged wakening from anesthesia, and increased cancer recurrence (27). In the present study, the amount of intraoperatively administered fentanyl was significantly reduced by using thoracic epidural analgesia. TEA with tracheal extubation at the end of the surgical procedure has been proven as a safe procedure, associated with low morbidity and mortality (28). The immediate postoperative extubation rate was 97.1% in the ERAS group, with an 89.9% rate of mobilization on POD1. Postoperative “near-zero” fluid balance and thoracic epidural analgesia are very important for the early mobilization of patients on POD1 (11, 20, 28, 29). Repeatedly, studies showed that immediate extubation in patients with TEA and early mobilization may reduce the systemic inflammatory response and pulmonary complications (28, 30–32).
Implementation of the ERAS protocol in esophageal surgery is very difficult due to the complexity of esophagectomy and patients’ comorbidities. In the present study, the most difficult barrer was persuading the healthcare providers to abandon the previous protocol, start to educate, and switch to a new one, particularly in patients with a higher ASA score. During changing the perioperative routine, checklist is needed to conduct the ERAS protocol with high adherence. Everyday discussion about clinical findings need to be done between anesthesiologist, surgeon, and all team (nurses and physiotherapist) to ensure right following protocol and improve treatment. A committed healthcare team is crucial to ensure goal-directed recovery for each patient and achieve specific goals to enhance recovery after oesophagectomy (26). This study suggested that the main condition for adequate implementation of the ERAS protocol is a multidisciplinary team with very experienced and dedicated staff.
This study may be significant because reflects everyday clinical practice and real life. Moreover, the ERAS protocol is feasible even in high-risk patients (with ASA score ≥ 3).
There are a few limitations. The participants were not randomized. Furthermore, there were differences in ASA score and BMI, type of surgical approach, and surgical procedure time between the groups. However, the ASA score was higher in the ERAS group. Despite the difference in BMI, there was no statistically significant difference in NRS-2002 between groups. Modifications in operative technique and approach may impact on clinical outcomes (33, 34), although it has been shown that perioperative protocol with the emphasis on close collaboration between anesthesiologists and other members of a team is an independent factor for successful postoperative outcomes (26).
5 ConclusionThe present study showed that implementation of ERAS protocol in an experienced center for esophageal surgery with anesthesiologist elements such as GDT, opioid-sparing anesthesia, and postoperative “near-zero” fluid balance may reduce postoperative morbidity, especially pulmonary complications rate. An implementation of the ERAS protocol after esophagectomy is feasible even in high-risk patients. Evaluation of ERAS protocol through clinical practice and research can obtain more data about the advantages and drawbacks of this approach with special emphasis on fluid management.
Data availability statementThe raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statementThe studies involving humans were approved by Ethics Committee of University Clinical Centre of Serbia. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributionsMD: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Writing – original draft. OS: Conceptualization, Investigation, Writing – original draft. DS: Conceptualization, Investigation, Methodology, Writing – review & editing. NK: Writing – review & editing. BM: Data curation, Formal analysis, Methodology, Software, Writing – review & editing. PS: Writing – review & editing. AS: Writing – review & editing. MM: Data curation, Writing – review & editing. SS: Data curation, Writing – review & editing. DM: Data curation, Formal analysis, Writing – review & editing. IP: Conceptualization, Formal analysis, Investigation, Methodology, Supervision, Validation, Writing – original draft.
FundingThe author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interestThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s noteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References1. Bray, F, Ferlay, J, Soerjomataram, I, Siegel, RL, Torre, LA, and Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2018) 68:394–424. doi: 10.3322/caac.21492
PubMed Abstract | Crossref Full Text | Google Scholar
2. Raymond, DP, Seder, CW, Wright, CD, Magee, MJ, Kosinski, AS, Cassivi, SD, et al. Predictors of major morbidity or mortality after resection for esophageal cancer: a society of Thoracic Surgeons general thoracic surgery database risk adjustment model. Ann Thorac Surg. (2016) 102:207–14. doi: 10.1016/j.athoracsur.2016.04.055
PubMed Abstract | Crossref Full Text | Google Scholar
3. Tang, Z, Lu, M, Qu, C, Zhang, Y, Li, L, Li, S, et al. Enhanced recovery after surgery improves short-term outcomes in patients undergoing esophagectomy. Ann Thorac Surg. (2022) 114:1197–11204. doi: 10.1016/j.athoracsur.2021.08.073
PubMed Abstract | Crossref Full Text | Google Scholar
4. Low, DE, Allum, W, De Manzoni, G, Ferri, L, Immanuel, A, Kuppusamy, M, et al. Guidelines for perioperative care in esophagectomy: enhanced recovery after surgery ERAS. World J Surg. (2019) 43:299–330. doi: 10.1007/s00268-018-4786-4
PubMed Abstract | Crossref Full Text | Google Scholar
5. Scott, MJ, Baldini, G, Fearon, KC, Feldheiser, A, Feldman, LS, Gan, TJ, et al. Enhanced recovery after surgery (ERAS) for gastrointestinal surgery, part 1: pathophysiological considerations. Acta Anaesthesiol Scand. (2015) 59:1212–31. doi: 10.1111/aas.12601
PubMed Abstract | Crossref Full Text | Google Scholar
7. Nevo, Y, Arjah, S, Katz, A, Ramírez García Luna, JL, Spicer, J, Cools-Lartigue, J, et al. ERAS 2.0: continued refinement of an established enhanced recovery protocol for esophagectomy. Ann Surg Oncol. (2021) 28:4850–8. doi: 10.1245/s10434-021-09854-7
Crossref Full Text | Google Scholar
8. White, PF, Kehlet, H, Neal, JM, Schricker, T, Carr, DB, Carli, F, et al. The role of the anesthesiologist in fast-track surgery: from multimodal analgesia to perioperative medical care. AnesthAnalg. (2007) 104:1380–96. doi: 10.1213/01.ane.0000263034.96885.e1
PubMed Abstract | Crossref Full Text | Google Scholar
9. Taniguchi, H, Sasaki, T, Fujita, H, Kobayashi, H, Kawasaki, R, Ogata, T, et al. Effects of goal-directed fluid therapy on enhanced postoperative recovery: an interventional comparative observational study with a historical control group on oesophagectomy combined with ERAS program. Clin Nutr ESPEN. (2018) 23:184–93. doi: 10.1016/j.clnesp.2017.10.002
PubMed Abstract | Crossref Full Text | Google Scholar
10. Mukai, A, Suehiro, K, Watanabe, R, Juri, T, Hayashi, Y, Tanaka, K, et al. Impact of intraoperative goal-directed fluid therapy on major morbidity and mortality after transthoracic oesophagectomy: a multicentre, randomised controlled trial. Br J Anaesth. (2020) 125:953–61. doi: 10.1016/j.bja.2020.08.060
PubMed Abstract | Crossref Full Text | Google Scholar
11. Xing, X, Gao, Y, Wang, H, Qu, S, Huang, C, Zhang, H, et al. Correlation of fluid balance and postoperative pulmonary complications in patients after esophagectomy for cancer. J Thorac Dis. (2015) 7:1986–93. doi: 10.3978/j.issn.2072-1439.2015.11.24
PubMed Abstract | Crossref Full Text | Google Scholar
12. Low, DE, Alderson, D, Cecconello, I, Chang, AC, Darling, GE, D’Journo, XB, et al. International consensus on standardization of data collection for complications associated with esophagectomy: esophagectomy complications consensus group (ECCG). Ann Surg. (2015) 262:286–94. doi: 10.1097/SLA.0000000000001098
PubMed Abstract | Crossref Full Text | Google Scholar
13. Casado, D, López, F, and Martí, R. Perioperative fluid management and major respiratory complications in patients undergoing esophagectomy. Dis Esophagus. (2010) 23:523–8. doi: 10.1111/j.1442-2050.2010.01057.x
PubMed Abstract | Crossref Full Text | Google Scholar
14. Veelo, DP, van Berge Henegouwen, MI, Ouwehand, KS, Geerts, BF, Anderegg, MC, van Dieren, S, et al. Effect of goal-directed therapy on outcome after esophageal surgery: a quality improvement study. PLoS One. (2017) 12:e0172806. doi: 10.1371/journal.pone.0172806
PubMed Abstract | Crossref Full Text | Google Scholar
15. Bahlmann, H, Halldestam, I, and Nilsson, L. Goal-directed therapy during transthoracic oesophageal resection does not improve outcome: randomised controlled trial. Eur J Anaesthesiol. (2019) 36:153–61. doi: 10.1097/EJA.0000000000000908
Crossref Full Text | Google Scholar
16. Rollins, KE, and Lobo, DN. Intraoperative goal-directed fluid therapy in elective major abdominal surgery: a Meta-analysis of randomized controlled trials. Ann Surg. (2016) 263:465–76. doi: 10.1097/SLA.0000000000001366
Crossref Full Text | Google Scholar
17. Myles, PS, Bellomo, R, Corcoran, T, Forbes, A, Peyton, P, Story, D, et al. Restrictive versus liberal fluid therapy for major abdominal surgery. N Engl J Med. (2018) 378:2263–74. doi: 10.1056/NEJMoa1801601
PubMed Abstract | Crossref Full Text | Google Scholar
18. Theodorou, D, Drimousis, PG, Larentzakis, A, Papalois, A, Toutouzas, KG, and Katsaragakis, S. The effects of vasopressors on perfusion of gastric graft after esophagectomy. An experimental study. J Gastrointest Surg. (2008) 12:1497–501. doi: 10.1007/s11605-008-0575-y
Crossref Full Text | Google Scholar
19. Walsh, KJ, Zhang, H, Tan, KS, Pedoto, A, Desiderio, DP, Fischer, GW, et al. Use of vasopressors during esophagectomy is not associated with increased risk of anastomotic leak. Dis Esophagus. (2021) 34:doaa090. doi: 10.1093/dote/doaa090
PubMed Abstract | Crossref Full Text | Google Scholar
20. Glatz, T, Kulemann, B, Marjanovic, G, Bregenzer, S, Makowiec, F, and Hoeppner, J. Postoperative fluid overload is a risk factor for adverse surgical outcome in patients undergoing esophagectomy for esophageal cancer: a retrospective study in 335 patients. BMC Surg. (2017) 17:6. doi: 10.1186/s12893-016-0203-9
PubMed Abstract | Crossref Full Text | Google Scholar
21. Kubo, Y, Tanaka, K, Yamasaki, M, Yamashita, K, Makino, T, Saito, T, et al. The impact of perioperative fluid balance on postoperative complications after esophagectomy for esophageal cancer. J Clin Med. (2022) 11:3219. doi: 10.3390/jcm11113219
PubMed Abstract | Crossref Full Text | Google Scholar
22. Chappell, D, Jacob, M, Hofmann-Kiefer, K, Conzen, P, and Rehm, M. A rational approach to perioperative fluid management. Anesthesiology. (2008) 109:723–40. doi: 10.1097/ALN.0b013e3181863117
PubMed Abstract | Crossref Full Text | Google Scholar
24. Li, X, Zhang, Q, Zhu, Y, Yang, Y, Xu, W, Zhao, Y, et al. Effect of perioperative goal-directed fluid therapy on postoperative complications after thoracic surgery with one-lung ventilation: a systematic review and meta-analysis. World J Surg Oncol. (2023) 21:297. doi: 10.1186/s12957-023-03169-5
PubMed Abstract | Crossref Full Text | Google Scholar
25. Raftery, NB, Murphy, CF, Donohoe, CL, O'Connell, B, King, S, Ravi, N, et al. The complexity of defining postoperative pneumonia after esophageal Cancer surgery: a Spectrum of lung injury rather than a simple infective complication? Ann Surg. (2022) 276:e400–6. doi: 10.1097/SLA.0000000000004546
PubMed Abstract | Crossref Full Text | Google Scholar
26. Preston, SR, Markar, SR, Baker, CR, Soon, Y, Singh, S, and Low, DE. Impact of a multidisciplinary standardized clinical pathway on perioperative outcomes in patients with oesophageal cancer. Br J Surg. (2013) 100:105–12. doi: 10.1002/bjs.8974
PubMed Abstract | Crossref Full Text | Google Scholar
27. Shanthanna, H, Ladha, KS, Kehlet, H, and Joshi, GP. Perioperative opioid administration. Anesthesiology. (2021) 134:645–59. doi: 10.1097/ALN.0000000000003572
Crossref Full Text | Google Scholar
28. Chandrashekar, MV, Irving, M, Wayman, J, Raimes, SA, and Linsley, A. Immediate extubation and epidural analgesia allow safe management in a high-dependency unit after two-stage oesophagectomy. Results of eight years of experience in a specialized upper gastrointestinal unit in a district general hospital. Br J Anaesth. (2003) 90:474–9. doi: 10.1093/bja/aeg091
PubMed Abstract | Crossref Full Text | Google Scholar
29. Makaryus, R, Miller, TE, and Gan, TJ. Current concepts of fluid management in enhanced recovery pathways. Br J Anaesth. (2018) 120:376–83. doi: 10.1016/j.bja.2017.10.011
Crossref Full Text | Google Scholar
30. Huang, ZD, Gu, HY, Zhu, J, Luo, J, Shen, XF, Deng, QF, et al. The application of enhanced recovery after surgery for upper gastrointestinal surgery: meta-analysis. BMC Surg. (2020) 20:3. doi: 10.1186/s12893-019-0669-3
PubMed Abstract | Crossref Full Text | Google Scholar
31. Gu, CY, Zhang, J, Qian, YN, and Tang, QF. Effects of epidural anesthesia and postoperative epidural analgesia on immune function in esophageal carcinoma patients undergoing thoracic surgery. Mol Clin Oncol. (2015) 3:190–6. doi: 10.3892/mc
留言 (0)