
記住我










Safe general anesthesia is a drug-induced reversible condition that includes specific behavioral and physiological traits—unconsciousness, amnesia, analgesia, and akinesia—with concomitant stability of the autonomic, cardiovascular, respiratory, and thermoregulatory systems (1). Anesthesia delivery systems are essential intraoperative life support devices used to achieve these goals in surgical patients. Design advances in anesthesia technology have introduced complex features that enhance patient management in high-resource countries but render such devices impractical and unsafe in resource-poor locations that experience frequently interrupted electrical supply, inconsistent access to compressed oxygen (2) and consumables such as carbon dioxide (CO2)-absorbing granules (2), and little or no biomedical maintenance support. These constraints hinder the global goal to improve access to safe surgical and anesthesia care as described by the Lancet Commission on Global Surgery and the World Health Assembly in 2015 (3).
The Universal Anaesthesia Machine (UAM®) (Gradian Health Systems Inc. New York, United States) was designed to overcome these constraints by providing a source of concentrated oxygen from ambient air, low-resistance vaporizers, and one-way expulsion of CO2 in the absence of CO2-absorbing granules. The machine could thus enhance the capacity to provide safe and consistent anesthetic care for surgical patients in low-resource conditions.
The objective of this study was to examine the safety and impact of introducing the UAM® into an austere clinical environment with limited perioperative resources. Specifically, we examined the effect of the addition of the UAM® on the practice of total intravenous anesthesia (TIVA) techniques for general anesthesia in a tertiary-care hospital in Sierra Leone. We hypothesized that if local anesthesia providers had access to a reliable, safe, and effective anesthesia delivery system, we would observe a shift among general anesthesia cases from TIVA techniques to increased use of inhalational agents. We also examined the performance of the UAM® in the presence of environmental constraints and reviewed its effects on intraoperative care, postoperative sedation, and analgesic levels after its deployment.
2 Methods 2.1 Study settingThis study took place at Connaught Hospital in Freetown, Sierra Leone, West Africa. Connaught Hospital is a tertiary-level government hospital with 275 beds that serves as a national referral center, providing all health services except maternal and non-surgical pediatric healthcare. Here, 10–15 cases are performed in the operating rooms.
2.2 EthicsThe study approval was obtained from the Sierra Leone Ethics and Scientific Review Committee and our Institutional Review Board. All participants provided consent prior to enrolling in the study. The funding company did not provide any oversight with respect to data review or choice of data collection. They did not see or influence study plans or results, nor did they influence study design, or review outcomes prior to or during abstract and manuscript generation. Safeguards against research influence were incorporated within a memorandum of understanding with the company.
2.3 Study designWe conducted a prospective observational study of anesthesia practice among all anesthesia providers at Connaught Hospital (10 nurse anesthetists and 1 physician anesthetist), examining perioperative clinical parameters among a convenience sample of surgical patients. Observed procedures and enrolled patients were those scheduled to receive surgical care on weekdays (M-F) between 8:30 a.m. and 4:00 p.m. and consented to participate in the study, respectively. We designed and piloted the perioperative data collection forms among anesthesia providers at the Johns Hopkins Hospital, Baltimore, Maryland, United States, and subsequently modified these tools in-country to ensure contextually appropriate data variables and minimize data collection ambiguity. Data were collected at the study site over a period of 25 months (June 2012 to July 2014). Baseline clinical anesthesia practice was determined through direct observation of care and documentation of perioperative tasks by anesthesia providers in a preceding observational exercise from June 2012 to February 2013 (pre-UAM® deployment) (4), after which we introduced the UAM® to the hospital. Device deployment was accompanied by a 1-week training course for all anesthesia care providers and biomedical technicians. The training involved basic principles related to the provision of general anesthesia and the use of the UAM. Given the introduction of new UAMs, we worked closely with Gradian Health for a detailed step-by-step walk-through of the use of the UAMs. We continued the observation of anesthesia practice after device introduction for 18 months from February 2013 to August 2014.
We trained seven Sierra Leonean research assistants, including two research nurses, on research methodology, operating room etiquette, and other relevant tasks. These research assistants were also trained to assess clinical care, including vital sign monitoring, and clinical parameters such as pain and consciousness level of patients in the perioperative period. Intraoperative data collection took place from Monday to Friday over a period of 2 years, except on hospital-sanctioned holidays when elective surgical cases were not performed. Research nurses monitored vital signs at designated times in the postoperative period. The Johns Hopkins-based research team (consisting of US-based clinicians with public health expertise) supervised research assistant training and data collection directly until they obtained a kappa statistic of agreement ≥0.7 (5).
Postoperatively, we followed the clinical status of observed cases to hospital discharge or to postoperative day 30 through examination of hospital ward records. The research nurses conducted direct patient clinical assessments for recovery from anesthesia and surgery in the first 72 postoperative hours among a convenience sample of consented patients.
2.4 Materials 2.4.1 Anesthesia devices• The UAM® can be classified as a low-resource optimized anesthesia machine in that it is designed for environments that must contend with power interruptions, compressed oxygen shortages, and biomedical technician limitations. It is an electric anesthesia delivery system with an incorporated high-capacity oxygen concentrator capable of providing a flow of 10 L/min with 95% inspired oxygen delivery to the patient. It utilizes a low-resistance draw-over vaporizer system that permits the combination of continuous flow and/or draw-over anesthesia for varying conditions encountered in resource-challenged, austere environments. Although the UAM® can use compressed cylinder oxygen or pipeline oxygen sources to deliver oxygen and inhaled agents, the low-resistance draw-over vaporizer can function without compressed gases via egress of room air into the system, providing anesthesia delivery to the patient in the absence of compressed gases or electrical power. It is an oxygen sensor that analyzes the inspired oxygen concentration delivered to the patient and displays this on a monitor with a 10-h battery backup. The UAM® model used in this study is designed for spontaneous and/or manually assisted ventilation (with manual bellows, all UAMs® are delivered with an attached multifunction cardiac monitor from a different manufacturer). The UAM® has CE certification for safe use by the European Union, and the system was approved for use by the Sierra Leone Ministry of Health and the IRB for the country. The UAM® was already in use in the United Kingdom at the time of commencing the study. The Johns Hopkins University School of Medicine created an NGO organizational agreement with the authorities in the country and had a memorandum of understanding (MOU) with the authorities in Sierra Leone. The government authorized the UAMs to be used in-country before the study.
• The Compact-3 (manufacturer unknown) is a type of Boyle’s anesthesia machine [a continuous-flow anesthesia machine with five basic elements: (1) a high-pressure supply of gases, (2) pressure gauges on oxygen cylinders, with pressure-reducing valves, (3) flow meters, (4) metal and glass vaporizer bottle for ether, and (5) a breathing system] (6). The Compact-3 was in residence during this study although its utility was intermittent due to frequent mechanical dysfunction.
• A Glostavent® Anaesthesia Machine (Diamedica (United Kingdom) Limited, Grange Hill Industrial Estate, Bratton Fleming, Barnstaple, Devon, EX31 4UH, United Kingdom) was present but malfunctioned (oxygen concentrator and ventilator) and was retired 3 months after the deployment of the UAM®.
The Glostavent can also be classified as a low-resource optimized anesthesia machine.
Patient monitoring devices used during data collection included non-invasive blood pressure monitors, Lifebox® pulse oximeters (Lifebox, London, United Kingdom), and electronic thermometers with disposable slips.
2.5 Data collectionUsing anesthesia data records, research assistants documented anesthesia-related tasks from patient preoperative arrival to postoperative patient handoff. Surgical procedure and patient demographic data were obtained from the operation list or anesthesia/surgery records. Some variables such as American Society of Anesthesiologists (ASA) clinical status scores and elective or emergent status of the case required verbal confirmation from the anesthesia provider.
Anesthesia-related tasks (e.g., airway management), anesthesia technique, vital signs, and electrical and mechanical disturbances in the operating room were recorded. Timestamps for events such as power failures and anesthesia/surgery start and stop times were collected. Appropriate precautions were taken to avoid distracting providers from patient care by suspending questions during active delivery of care and complying with operating room etiquette. In the 30-day postoperative period, data collectors ascertained the admission status of patients using the following categories: a return to the operating theater within the 30-day period, hospital discharge, or death. Research nurses documented vital signs at the following postoperative times: 1, 2, and 4 h and 1, 2, and 3 days. The Wong–Baker Faces Pain Scale was used to assess self-reported postoperative pain scores, and the Richmond Agitation Sedation Scale was used to determine sedation level in the initial 4-h postoperative period (7, 8). We also reviewed operating room logbooks to determine anesthesia caseload and technique, including those performed outside study observation hours.
With an α-error set to 0.05, a modest treatment effect (20% reduction in ketamine TIVA-only cases), and a true failure rate for experimental subjects as 0.4, we needed to enroll 518 experimental subjects and 518 control subjects (for a minimum sample size = 1,036 cases) to be able to reject the null hypothesis that the failure rates for experimental and control subjects are equal with probability (power) of 0.9. Our sample size justification, based on an uncorrected chi-squared test, was appropriate for this study.
Anesthesia records and follow-up data were scanned into data-secure computers, and the information was abstracted for entry into a FileMaker Pro database (FileMaker, Inc., Santa Clara, CA, United States) and subsequently Microsoft Excel (Microsoft Corp., Redmond, WA, United States). Using STATA 12 software (StataCorp LP, College Station, TX, United States), data analyses included frequency distributions, chi-square test, Wilcoxon rank-sum test, two-sample test of proportions, and linear and logistic regression to compare and examine the relationship between variables, using a statistical significance set at a p-value of <0.05.
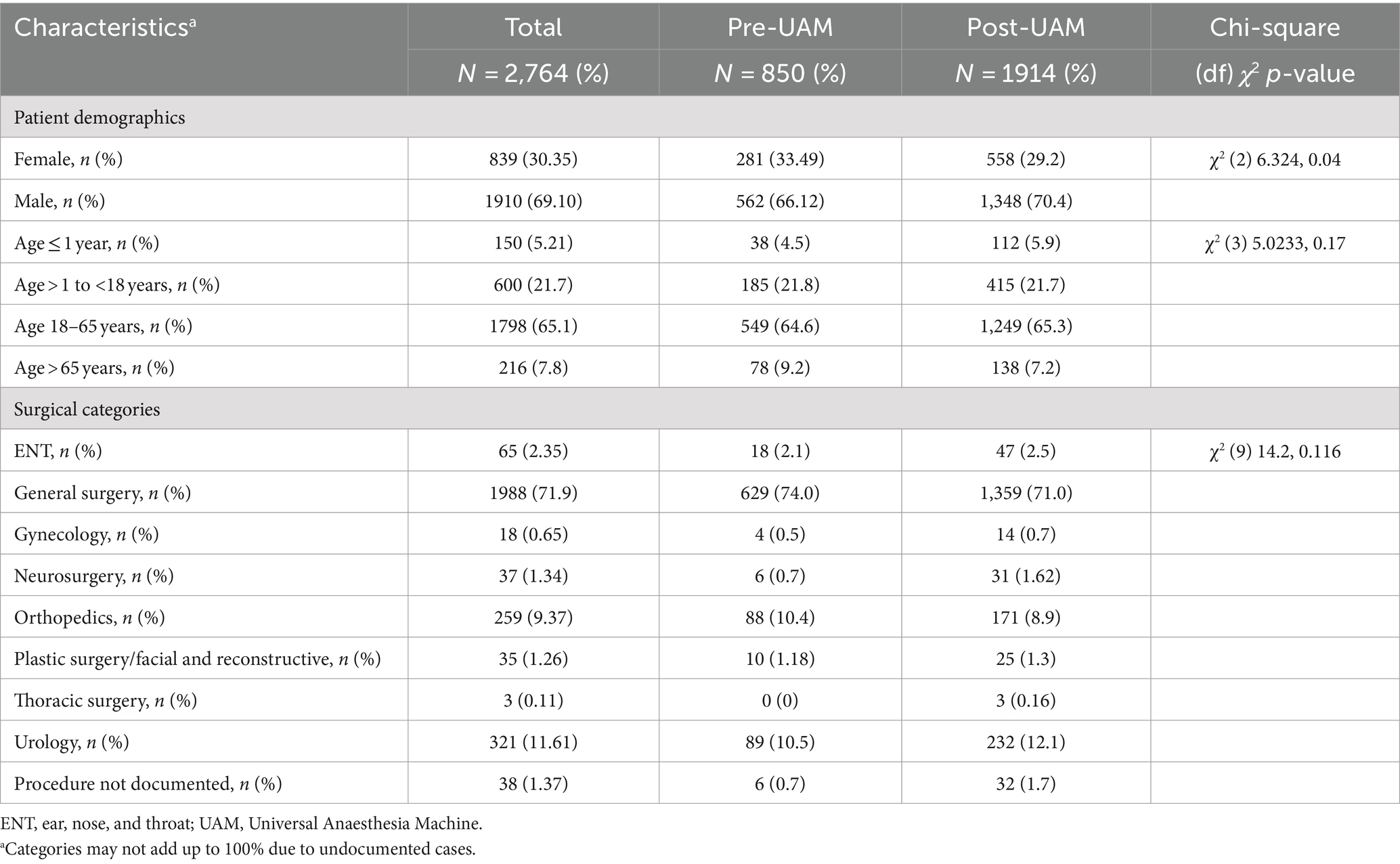
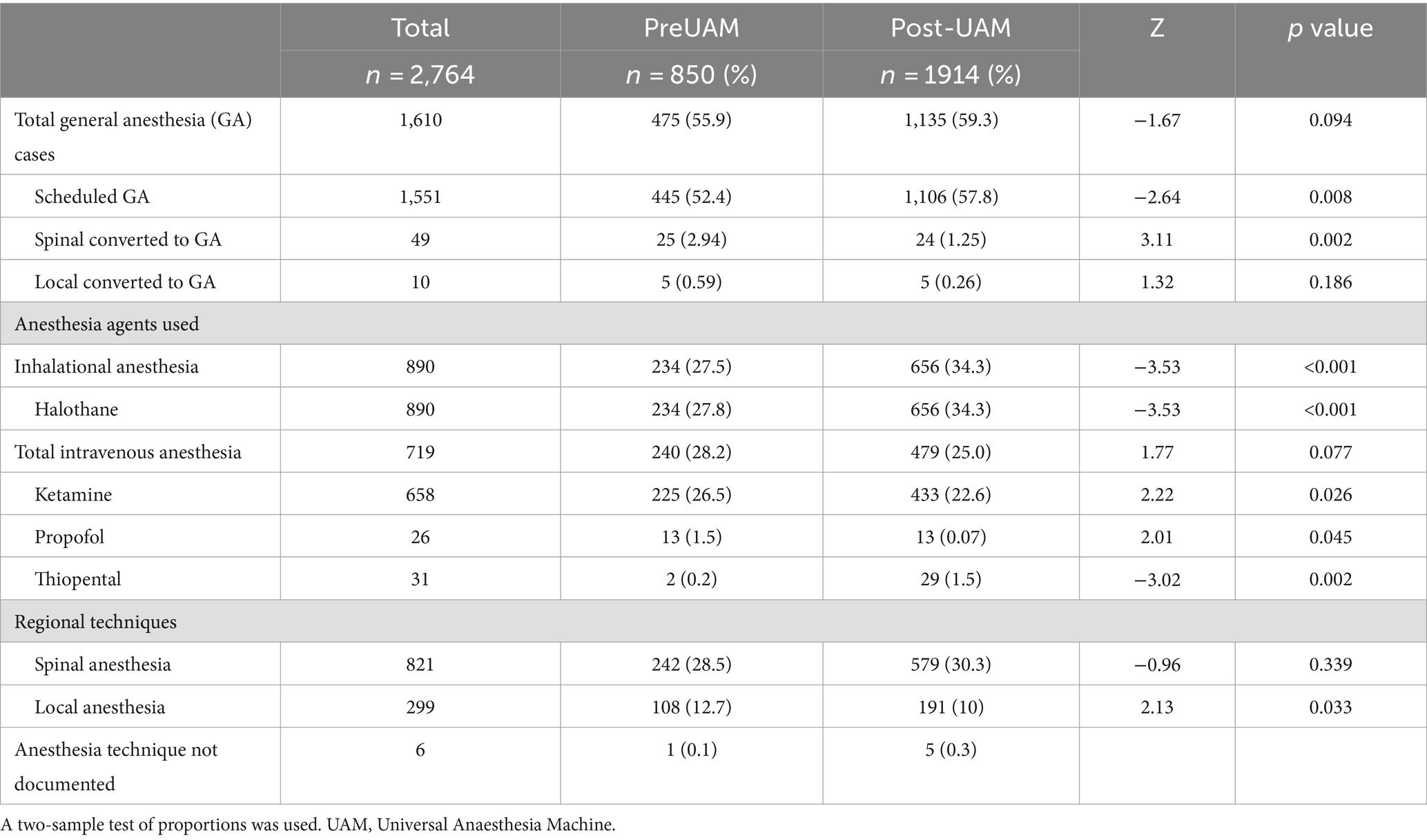
3 Results and discussionAccording to hospital operating room records (Table 1), 2,764 anesthetic cases were performed between June 2012 and July 2014. Of these, 850 took place before the introduction of the UAM®, and 1,917 took place after the introduction of UAM®. Table 2 describes the distribution of anesthesia techniques.
Table 1. Description of anesthetic cases (Connaught Hospital operating room registry).
Table 2. Description of all performed anesthesia techniques (operating room registry).
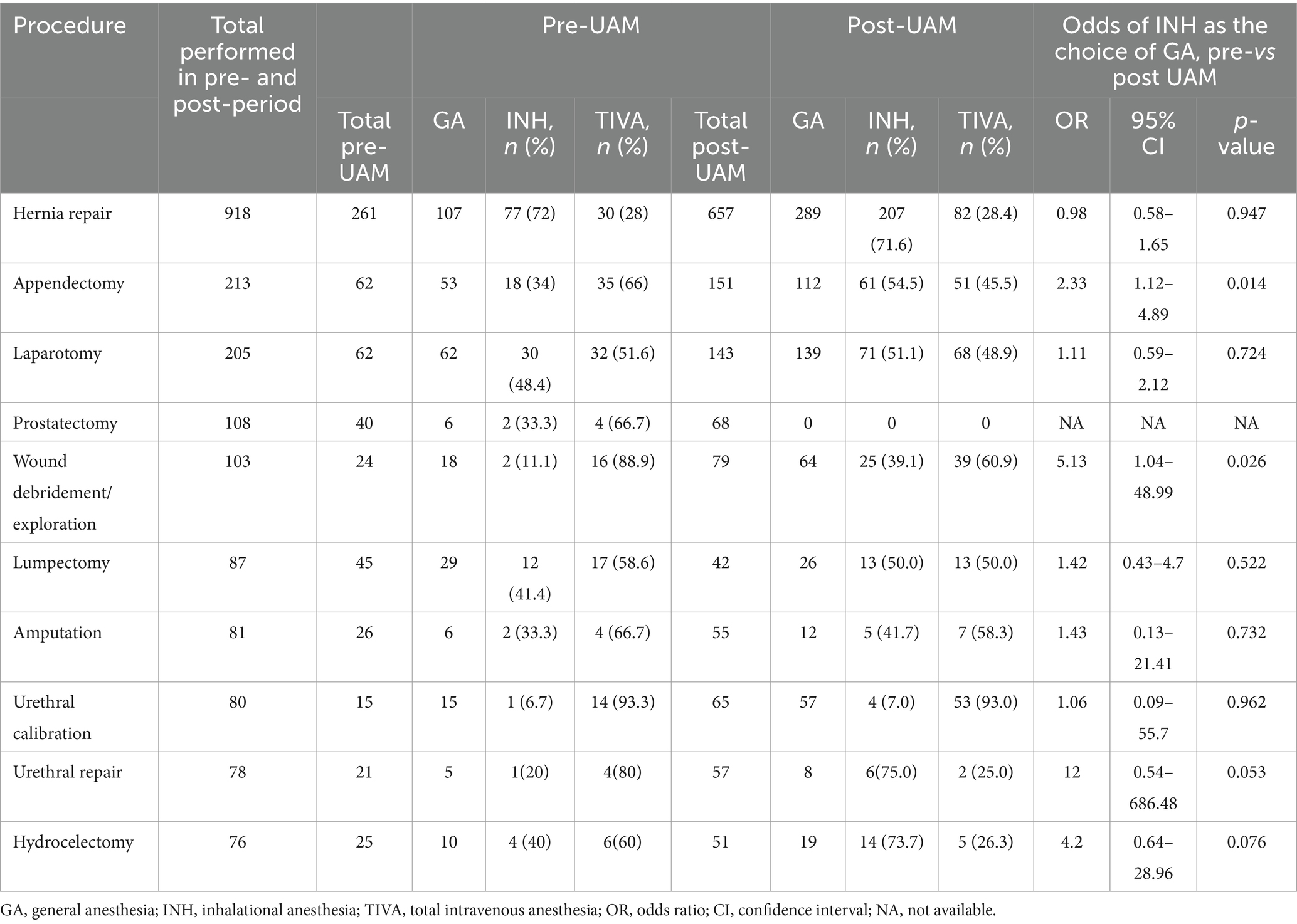
We reviewed all general anesthesia techniques performed in pre-and post-UAM® study phases and, after controlling for age and surgical categories, observed a 1.6-fold increase (p = 0.001, 95% CI [1.19–2.14]) in the odds of inhalational anesthesia administration compared to TIVA, in the post-UAM® period. This shift from TIVA (predominantly ketamine) to inhalational anesthesia was most demonstrable in anesthesia care for patients undergoing appendectomies and surgical wound management (Table 3).
Table 3. General anesthesia use among the 10 most common surgical cases performed (operating room registry).
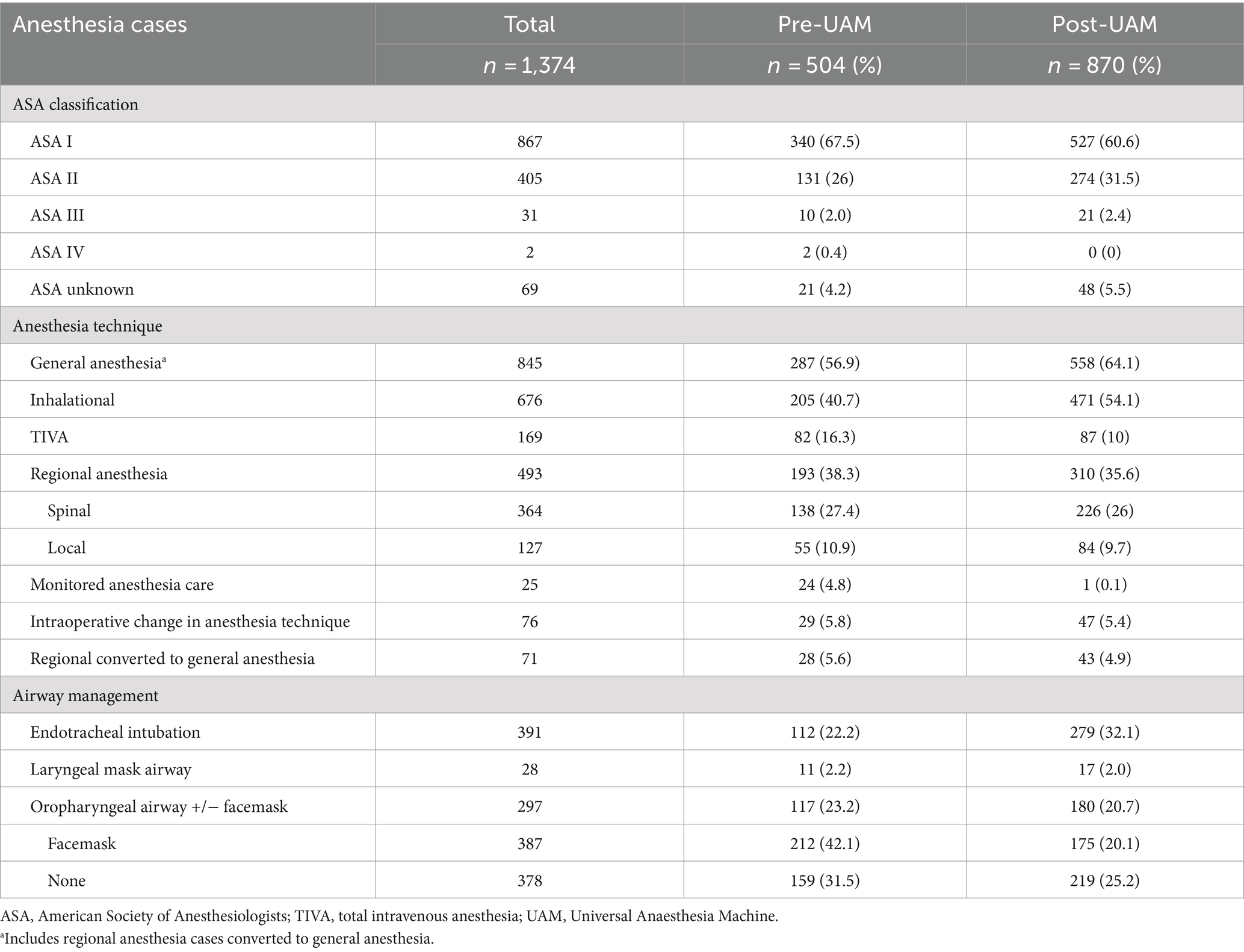
3.1 Directly observed anesthesia casesIn the post-UAM® phase, we observed 870 cases of perioperative anesthesia care (Table 4), 45.5% of all cases performed. In total, 20 of these cases were described as emergent by local providers.
Table 4. Anesthesia cases/techniques performed on directly observed cases (directly observed by the team).
3.2 Intraoperative periodAmong regional cases converted to general anesthesia (Table 4), inhalational agents were utilized 54% of the time. Providers monitored blood pressure in 612 (70.3%) patients, pulse oximetry in 827 (95.1%), electrocardiography in 30 (3.5%), temperature in 23 (2.7%), and capnography in 10 (1.15%). Blood pressure was more likely to be measured in patients older than 18 years of age, χ2 (2, N = 870) p < 0.001.
We observed 343 incidents of intraoperative tachycardia (heart rate > 100 beats/min for ≥10 min in patients >12 years). The proportion of patients who experienced tachycardia did not differ among patients who received inhalational anesthesia from the UAM® and those whose anesthesia was delivered by another machine, z = 1.96, p = 0.05.
The portable free-standing oxygen concentrator onsite had a maximum delivery capacity of 5 L/min and had been improvised to connect to the Compact-3 anesthesia machine. All observations where oxygen delivery flow rates were greater than 5 L/min occurred in cases involving the UAM® or an oxygen tank. Compressed cylinder oxygen was unavailable for >50% of the duration of the total observational period, and, when available, there was no reliable method to confirm the oxygen concentration in the cylinder.
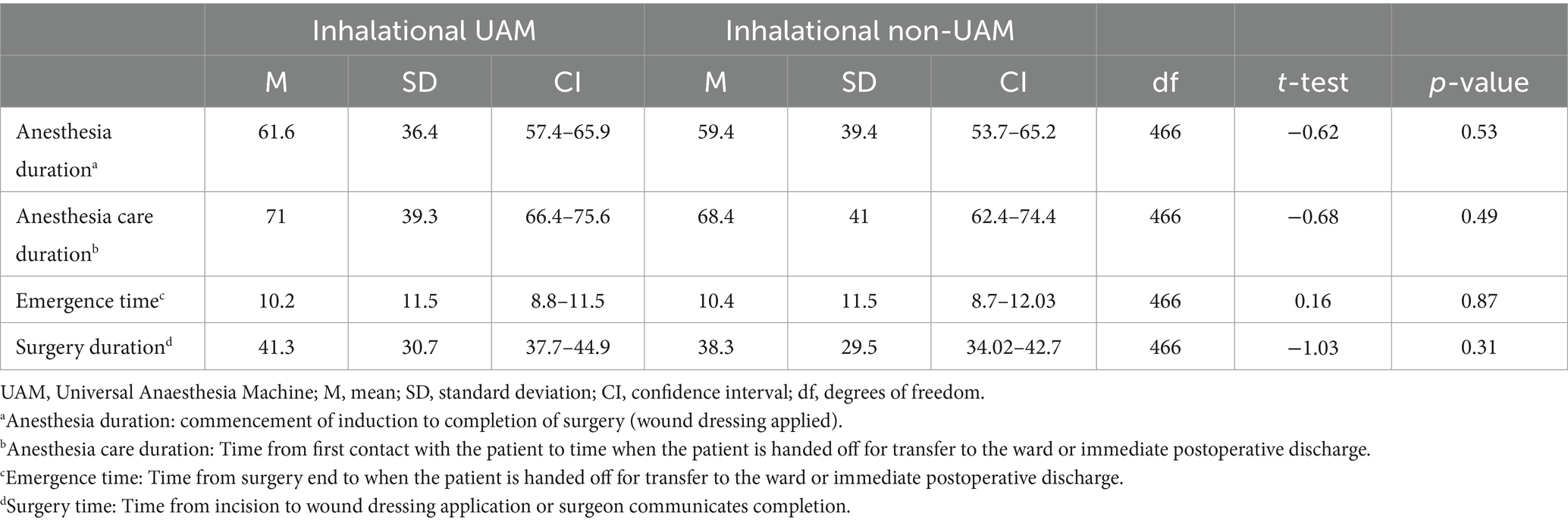
The UAM® was used to deliver inhalational anesthesia in 287 cases, and for supplemental oxygen delivery in 38 cases that did not involve the use of inhalational anesthesia. The choice of anesthesia machine did not affect the duration of anesthesia or surgical care (Table 5).
Table 5. Perioperative care duration (minutes) among inhalational anesthesia cases administered by UAM and non-UAM machines.
We recorded 27 instances of power outages ranging from 1 min to 90 min in duration. In total, 17 of these occurred during inhalational anesthesia delivery, of which 10 were administered with the UAM®. There were no interruptions in the latter as the UAM® immediately reverted to room air (with inhalational anesthetic), while ventilation in other cases was continued with an Ambu bag® (without inhalational anesthetic). There were two occasions of reported anesthesia equipment-related malfunction. On investigation, neither originated from the machine. One incident was a power surge, which damaged fuses in the UAM® as a result of surge protector removal prior to the event.
Biomedical technicians at Connaught Hospital replaced the fuses within hours of discovery, and the machine returned to full service. In the second event, the oxygen monitor displayed an alarm for the replacement of the oxygen sensor. This was initially mistaken for low oxygen concentration readings and occurred 11.5 months after the installation of the machine. The manufacturer recommends replacing the oxygen sensor after 12 months.
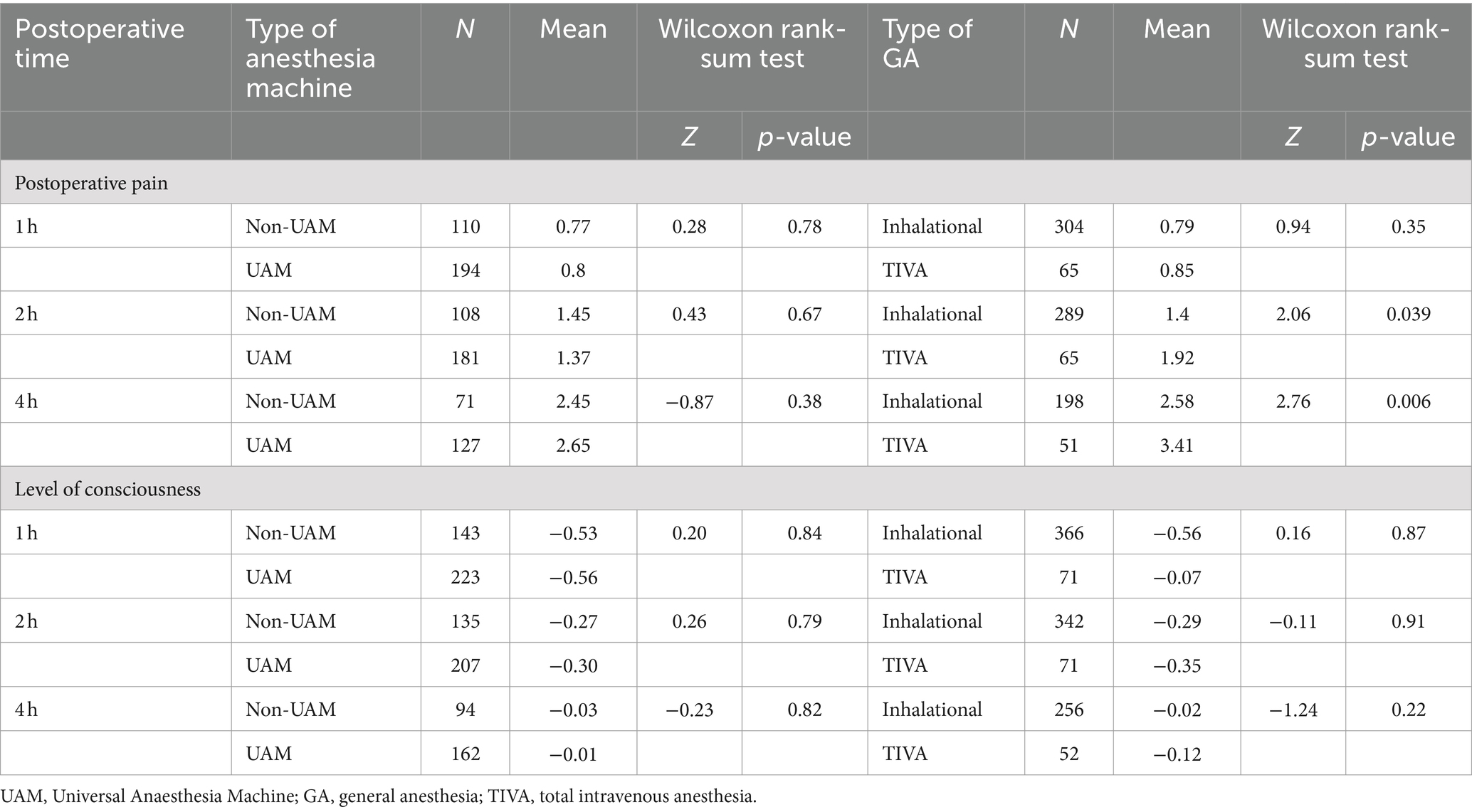
3.3 Postoperative outcomes and mortalityA Wilcoxon rank-sum test revealed a difference in hours 2 and 4 pain scores between TIVA and inhalational anesthesia cases (Table 6).
Table 6. Pain and level of consciousness scores among inhalational cases (by type of anesthesia machine) and general anesthesia cases 1–4 h postoperatively.
Linear regression showed this to be significant at only hour 4, with pain scores lower in inhalational cases by −0.83, 95% CI [−1.37 to 0.29], p = 0.003. The rate of consciousness recovery did not differ between the two groups in hours 1, 2, or 4 postoperatively. Anesthesia machine differences used did not demonstrate a change in postoperative pain or level of consciousness scores at the 1-, 2-, or 4-h monitoring times (Table 6). In total, 30-day postoperative mortality among observed cases was 2.3% (20 patients), with a risk ratio of 1.66, 95% CI [0.7–3.9], p = 0.24, compared to the pre-UAM® period. We were unable to determine the postoperative status of 21 patients during the study period. These were either cases that were canceled mid-procedure or cases that we were unable to follow for the designated follow-up period owing to the 2014 Ebola Viral Hemorrhagic outbreak. Among inhalational anesthesia cases, we found no relation between mortality and the type of anesthesia machine used, χ2(1, N = 454) = 0.16, p = 0.691.
4 DiscussionIn 2008, the World Health Organization commenced the Global Initiative on Health Technologies to promote the design of innovative technologies adapted for use in resource-limited settings, among other goals. This initiative was borne out of a recognition of the mismatch between available health technology and health infrastructure in many low-resource locations (9, 10). A 2011 study of medical devices in developing countries revealed that, on average, 38.3% of medical technologies in such locations were out of service (8). These findings have been attributed to a lack of appropriate training and infrastructure as well as technological mismanagement (11, 12). The oxygen sensors continue to be a problem. More recent studies involving the UAM aimed to examine simulation methodologies to adopt the use of the UAM (13–15). In the case of anesthesia technology, other factors that may be responsible for the premature retirement of devices include unreliable electricity, absence of compressed gases, insufficient biomedical expertise for maintenance, and ill-suited inhalational agent vaporizers. Although three anesthesia machines were used in varying degrees during the project, six anesthesia machines were physically present in the operating suite areas (Table 6).
As described above, we identified a significant increase in the use of inhalational anesthetic agents following the installation of the UAM®. Among failed regional anesthesia cases, the proportion converted to inhalational anesthesia relative to TIVA was significantly higher after the UAM® was introduced into the environment, z = 4.56, p ≤ 0.001.
The routine practice prior to the UAM® often included holding parts of the anesthesia machine together. In the absence of active maintenance agreements with anesthesia machine manufacturers, these machines were repaired by biomedical technicians and anesthesia staff through improvisation and inventive use of available materials or parts from other machines, which required securing them together so that they do not fall apart. Other challenges included unreliable oxygen delivery to the patient.
While power outages are relatively rare events, when they occur, then there is an increased risk to patients and barriers to the safe use of anesthesia. These events can be stressful and challenging, potentially leading to avoidance of the use of general anesthesia. With a system specifically designed for use in constrained environments, the UAM® allows for more consistently reliable delivery of general anesthesia and possibly more comfort for providers to utilize general anesthesia in these challenging environments.
During the study period, the facility experienced a number of unforeseen challenges that had adverse effects on surgical productivity. These events included shortages of inhalational anesthetics, periodic interruptions to compressed oxygen production and availability, autoclave breakdowns, and a shutdown of the operating room as a result of flooding from extreme weather. Although power outages were frequent, these were mitigated by the presence of a functional generator. Some of these impediments to surgical delivery could not be ameliorated by the UAM®, whereas some were specifically overcome by qualities of the UAM®. These include:
• efficient oxygen concentrator: able to administer 10 L/min of 95% oxygen, advantageous during the study period as compressed oxygen was unavailable >50% of the time.
• an oxygen analyzer: reliably measures the percentage of oxygen available to the patient by the oxygen concentrator. Before the study, we had been unable to confirm the concentration of oxygen in cylinders because the hospital lacked an oxygen analyzer. This monitor is powered by a trickle charge from the main power supply. This safety feature is critical to monitoring inspired oxygen content, especially during simultaneous power outages and compressed oxygen shortages.
• a low-pressure vaporizer: It enables continued inhalational anesthesia delivery during the simultaneous absence of compressed oxygen and electricity. In these events, the UAM® reverts to room air draw-over anesthetic mode, sustaining the patient at 21% oxygen. There were 10 incidents of power outages during inhalational anesthesia delivery with the UAM®.
• a halothane vaporizer: Although halothane has been largely replaced by isoflurane in high-income countries because of related side effects, it is still widely used in many African nations owing to its low cost (16, 17). The UAM® is outfitted with two detachable vaporizers: one each for halothane and isoflurane. Halothane and ether were the only available inhalational anesthetics.
• a one-way valve system: It prevents rebreathing and provides unidirectional gas flow. In this environment, CO2-absorbing granules are often not available or replaced. End-tidal CO2 (ETCO2) levels are not routinely measured, and hypercapnia may go undiagnosed with rebreathing systems. Although two capnography monitors were available in the operating suites, ETCO2 was rarely monitored as described in the Results section. The manufacturer recommends the use of passive scavenging of exhaust gases from the system. We did not observe adherence to these guidelines. Reasons for not using capnography included its unavailability in Sierra Leone at the time, the fact that capnography was not part of the UAM monitoring package, and, even when capnography monitors were introduced, the nurse anesthetists did not adopt its use because they were never formally trained in it, and the leadership was reluctant due to not having a good knowledge base for using it.
4.1 ImplicationsAmong all cases, we identified an increase in the proportion of general anesthetics performed, with the greater percentage being inhalational anesthesia, rather than ketamine TIVA. In debrief interviews, anesthesia providers described the UAM® as “simple,” “convenient,” and “straightforward.” Multiple users recommended the inclusion of an automated ventilator mode to ease the workload of manual ventilation during long cases. Subsequent UAM® models designed since the conclusion of the study include a mechanical ventilator.
4.2 Perioperative outcomesWe did not detect a difference in the occurrence of adverse events between UAM® and non-UAM® cases. With respect to postoperative pain, we identified a slight decrease in pain scores at hour 4 among inhalational cases compared to TIVA. There were no differences in analgesic administration. This fact is noteworthy; as halothane has minimal to no analgesic properties, it was often co-administered with boluses of intravenous anesthetics or narcotic analgesics, especially during anesthetic induction. Such co-administration occurred in 342 cases. It is possible that more reliable depth of anesthesia and quality general anesthesia may have led to less noxious stimulation during the surgery and may have led to pre-emptive analgesia, and thus difference in pain scores.
4.3 LimitationsWhile the training program can be viewed as a confounding and contributing factor in the outcome of the study, from its inception, the study design made a priori assumptions that training on clinical use and maintenance were essential elements to the acceptance and use of the UAM in common clinical practice. The training program does not overcome the obstacles of oxygen availability, stable electricity, and maintenance ease. However, it would be unethical to deploy novel technology in the absence of relevant training.
5 ConclusionAnesthesia technologies tailored to overcome austere environmental conditions have the ability to deliver safe anesthesia care while maintaining fidelity to recommended international anesthesia practice standards. In this study, we observed the in situ use of a low-resource optimized anesthesia machine, the Universal Anaesthesia Machine. In an environment with multiple unfavorable conditions, we were able to determine that the UAM® provided efficient and reliable anesthetic delivery without adverse outcomes. Since UAM® introduction at Connaught Hospital, a shift in ketamine-TIVA anesthetic administration to inhalational general anesthesia was observed. While there is no basis for identifying one anesthetic technique as superior to another, there are advantages to having options for different types of anesthesia for different types of cases and different types of patients.
The UAM® functioned without any significant mechanical problems and provided a reliable source of oxygen via the concentrator with an oxygen sensor/monitor to ensure adequate oxygen delivery during surgery. The use of devices that are designed to function in challenging austere environments, require minimal maintenance, and utilize local sources of replacement parts, combined with training of providers and technicians, should theoretically provide reliable, safe, and efficient care in these settings. Currently, there are two UAMs at Connaught that are frequently used. The maintenance team has been able to fix any problems that arise. Capnography is also being used. Pursuant to the 2015 World Health Assembly’s Resolution on Surgery and Anesthesia Care (3), it is imperative to examine the technological resources available to perioperative providers working in constrained conditions and strive to engineer appropriate technology for safe perioperative care in their environments.
Data availability statementThe original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statementThe studies involving humans were approved by Johns Hopkins Institutional Review Board; Sierra Leone Ethics and Scientific Review committee. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributionsJS: Writing – original draft, Writing – review & editing, Investigation, Methodology. RK: Writing – review & editing, Formal analysis, Investigation. OT: Writing – review & editing. AC: Data curation, Writing – review & editing, Methodology. EJ: Writing – review & editing, Investigation, Methodology. MR: Writing – review & editing, Investigation. MK: Writing – review & editing, Methodology, Investigation. HN-W: Writing – review & editing. ED: Writing – review & editing. BL: Funding acquisition, Investigation, Methodology, Writing – review & editing.
FundingThe author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study received financial support from Gradian Health Systems, Inc. (#900478). The authors acknowledged the financial support of the Thomas and Dorothy Tung Endowment, and the Division of Neuroanesthesiology, Johns Hopkins Department of Anesthesiology & Critical Care Medicine. The authors also acknowledge the Johns Hopkins Global Alliance of Perioperative Professionals for support throughout all the phases of this project.
Conflict of interestThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s noteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References1. Evers, A, and Crowder, M. Cellular and molecular mechanisms of anesthesia In: PG Barash, BF Cullen, RK Stoelting, M Cahalan, and MC Stock, editors. Clinical anesthesia. New York: Lippincott Williams & Wilkins (2006), 95–114.
2. Ezi-Ashi, TI, Papworth, DP, and Nunn, JF. Inhalational anaesthesia in developing countries. Part I. The problems and a proposed solution. Anaesthesia. (1983) 38:729–35. doi: 10.1111/j.1365-2044.1983.tb12195.x
Crossref Full Text | Google Scholar
3. World Health Assembly resolution A68/15. Strengthening emergency and essential surgical care and Anaesthesia as a component of universal health coverage, May 22nd (2015).
4. Koka, R, Chima, AM, Sampson, JB, Jackson, EV, Ogbuagu, OO, Rosen, MA, et al. Anesthesia practice and perioperative outcomes at 2 tertiary care hospitals in Freetown, Sierra Leone. Anesth Analg. (2016) 123:213–27. doi: 10.1213/ANE.0000000000001285
Crossref Full Text | Google Scholar
6. Watt, M . The evolution of the Boyle apparatus 1917-67. Anaesthesia. (1968) 23:103–18. doi: 10.1111/j.1365-2044.1968.tb00015.x
Crossref Full Text | Google Scholar
7. Sessler, CN, Gosnell, MS, Grap, MJ, Brophy, GM, O'Neal, PV, Keane, KA, et al. The Richmond agitation-sedation scale: validity and reliability in adult intensive care unit patients. Am J Respir Crit Care Med. (2002) 166:1338–44. doi: 10.1164/rccm.2107138
Crossref Full Text | Google Scholar
8. Garra, G, Singer, AJ, Taira, BR, Chohan, J, Cardoz, H, Chisena, E, et al. Validation of the Wong-baker FACES pain rating scale in pediatric emergency department patients. Acad Emerg Med. (2010) 17:50–4. doi: 10.1111/j.1553-2712.2009.00620
PubMed Abstract | Crossref Full Text | Google Scholar
9. World Health Organization. Medical devices: managing the mismatch: an outcome of the priority medical devices project (2010), pp. 14–15.
10. Howitt, P, Darzi, A, Yang, GZ, Ashrafian, H, Atun, R, Barlow, J, et al. Technologies for global health. Lancet. (2012) 380:507–35. doi: 10.1016/S0140-6736(12)61127-1
Crossref Full Text | Google Scholar
11. Perry, L, and Malkin, R. Effectiveness of medical equipment donations to improve health systems: how much medical equipment is broken in the developing world? Med Biol Eng Comput. (2011) 49:719–22. doi: 10.1007/s11517-011-0786-3
PubMed Abstract | Crossref Full Text | Google Scholar
12. Pena-Mohr, J . Distributing and transferring medical technology. A view from Latin America and the Caribbean. Int J Technol Assess Health Care. (1987) 3:281–91. doi: 10.1017/S026646230000057X
Crossref Full Text | Google Scholar
13. Tomobi, O, Toy, S, Ondari, M, Lee, S, Nelson-Williams, H, Koroma, M, et al. Evaluating rapid-cycle deliberate practice versus mastery learning in training nurse anesthetists on the universal anaesthesia machine ventilator in Sierra Leone. J Educ Perioper Med. (2021) 23:E658. doi: 10.46374/volxxiii_issue1_sampson
Crossref Full Text | Google Scholar
14. Sampson, JB, Lee, BH, Koka, R, Chima, AM, Jackson, EV, Ogbuagu, OO, et al. Human factors evaluation of the universal Anaesthesia machine: assessing equipment with high-fidelity simulation prior to deployment in a resource-constrained environment. J Natl Med Assoc. (2019) 111:490–9. doi: 10.1016/j.jnma.2019.03.005
PubMed Abstract | Crossref Full Text | Google Scholar
15. Chima, AM, Koka, R, Lee, B, Tran, T, Ogbuagu, OU, Nelson-Williams, H, et al. Medical simulation as a vital adjunct to identifying clinical life-threatening gaps in austere environments. J Natl Med Assoc. (2018) 110:117–23. doi: 10.1016/j.jnma.2017.12.003
PubMed Abstract | Crossref Full Text | Google Scholar
16. Halliday, NJ . Problems facing the visiting anesthesia team in an underdeveloped nation and possible solutions. J Craniofac Surg. (2015) 26:1066–8. doi: 10.1097/SCS.0000000000001629
留言 (0)