
記住我









Retroperitoneal fibrosis is an uncommon disorder of unclear etiology, with 8% of cases associated with malignancies, among which breast cancer is a relatively common cause. The pathogenesis of peritoneal fibrosis caused by tumors remains unclear, potentially involving direct neoplastic cell infiltration or inflammatory reactions triggered by cytokines secreted by tumor cells. Retroperitoneal fibrosis is characterized by increased fibrotic deposition in the retroperitoneum, frequently leading to ureteral obstruction [1]. Herein, we report a case of breast cancer with retroperitoneal fibrosis and renal insufficiency as the first symptoms. Conventional imaging did not reveal any evidence of breast cancer or distant metastases. However, 18F-deoxyglucose positron emission tomography/computer tomography (18F-FDG PET/CT) images demonstrated increased 18F-FDG uptake in the breast and kidney, which was suspicious of bilateral breast cancer (BBC) with diffuse renal metastatic lesions. PET/CT plays a crucial role in detecting primary lesions and metastatic lesions, monitoring relapses, managing treatment, and improving patient prognosis. In addition, we summarized the basic information and clinical details of some cases with tumor-associated retroperitoneal fibrosis in Table 1.
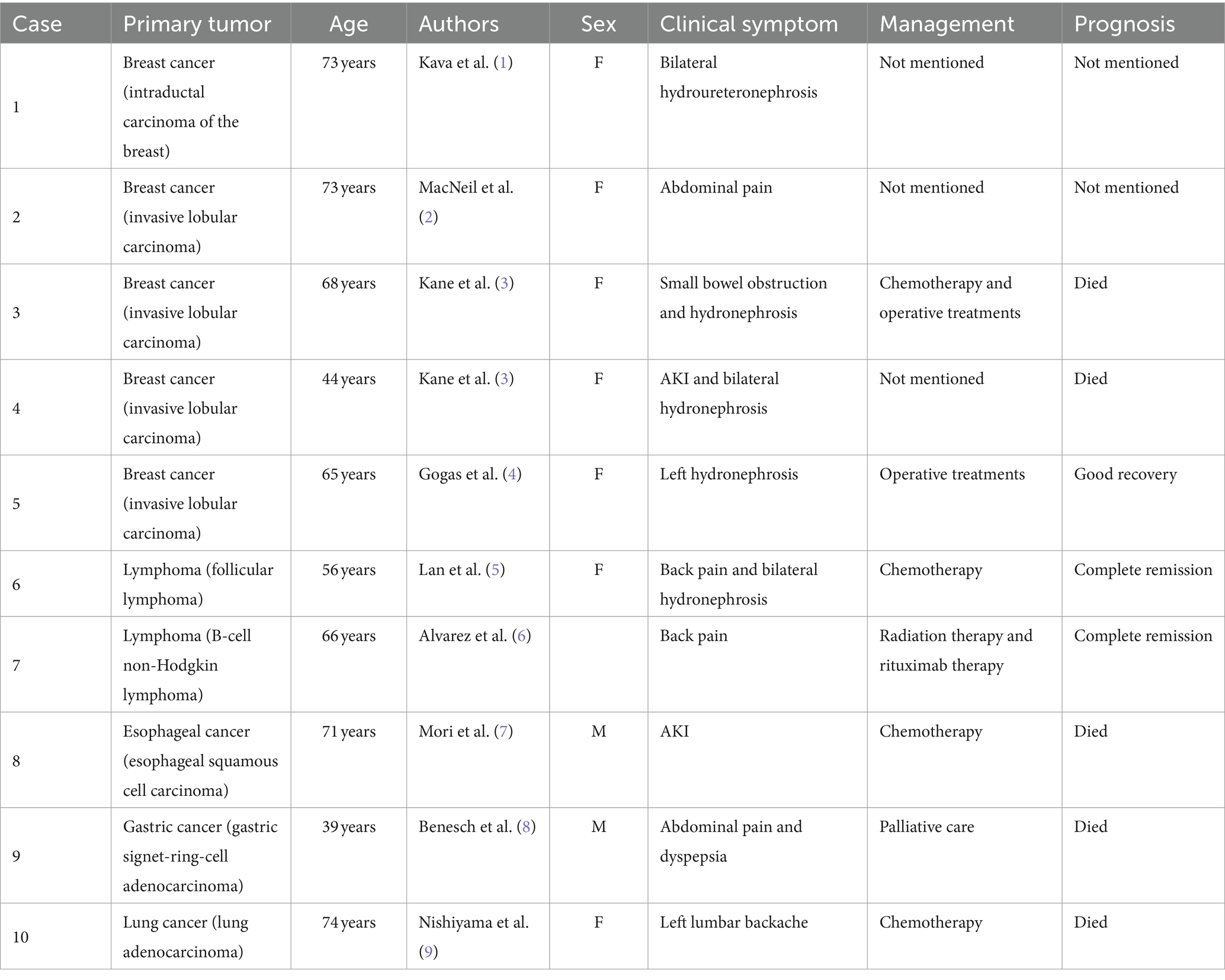
Table 1. Literature review of tumor-related retroperitoneal fibrosis.
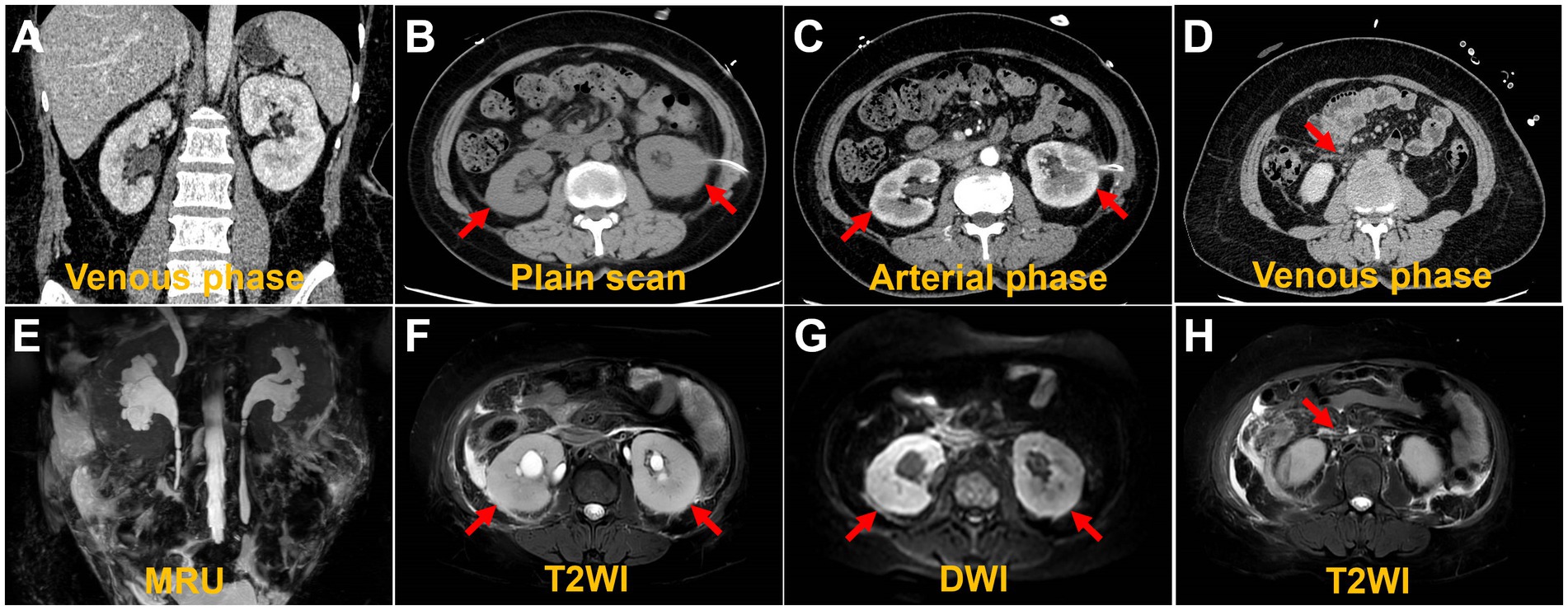
Case presentationA 49-year-old woman was referred to the hospital with elevated creatinine and oliguria for over a month. The patient experienced abdominal pain and lower back pain with noticeable pitting edema in both lower extremities, along with decreased urine, without an apparent trigger over a month ago. The patient has no family history of the disease. Laboratory results revealed a serum creatinine level of 1,054 μmol/L and a hemoglobin level of 76 g/L, suggestive of acute kidney injury (AKI). Ultrasonography demonstrated bilateral hydronephrosis with widening of the proximal ureters and moderately low echogenicity around the abdominal aorta, suggesting that retroperitoneal fibrosis might be present. Abdominal CT and magnetic resonance imaging (MRI) (Figure 1) revealed bilateral kidney swelling, dilation of the bilateral kidneys, renal calyces, and upper ureters, accompanied by multiple retroperitoneal and bilateral perirenal exudations, suggestive of retroperitoneal fibrosis. No focal lesions were found in either kidney.
Figure 1. Computed tomography images and magnetic resonance images. The coronal image shows bilateral hydronephrosis and enlarged kidneys (A,E). The axial images show diffuse lesions in the renal parenchyma, with no obvious masses detected (B,C,F,G). The axial image shows retroperitoneal multiple exudation (D,H).
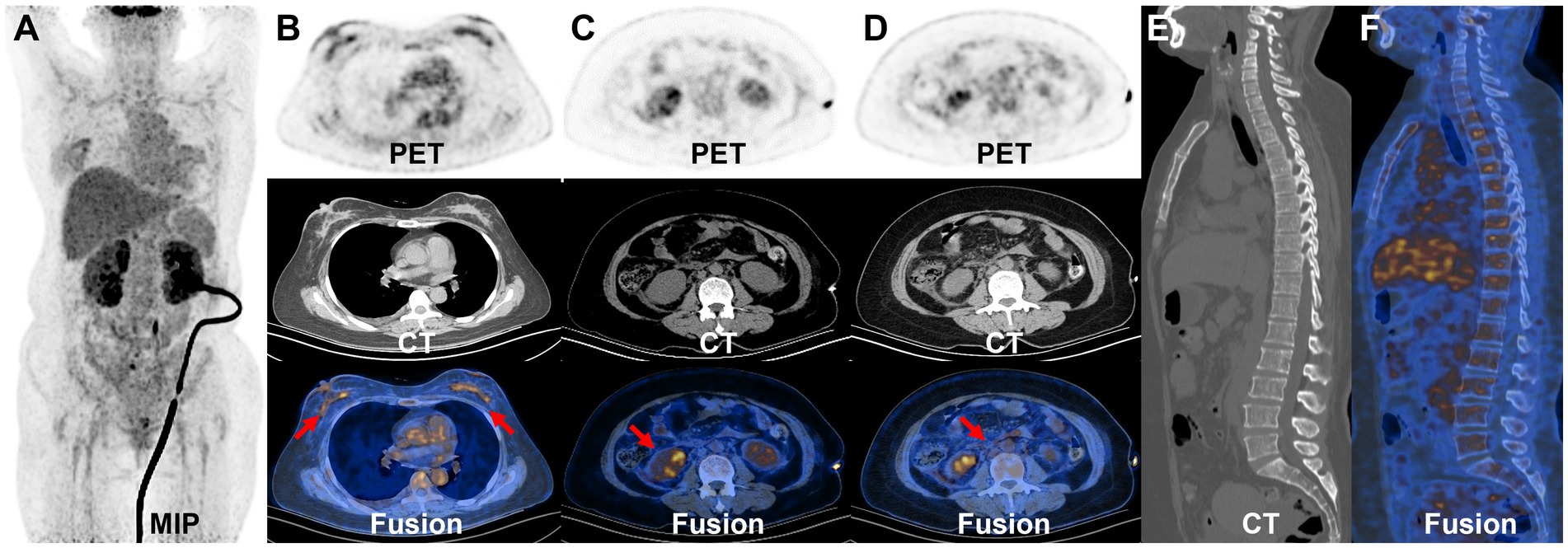
AKI is likely attributed to post-renal obstruction secondary to retroperitoneal fibrosis. To further define the histological features of renal lesions and exclude the probability of primary kidney disease, a biopsy was performed of the lower pole of the right kidney. The biopsy of the lower pole of the right kidney demonstrated acute renal tubular necrosis and heterotypic cells in the renal tissue. The tumor cells have moderate dysplasia, form adenoid arrangements, and show an invasive growth pattern. Immunohistochemical results showed that P120-, HER2-, PR 90%, ER 90%, E-Cadherin-, GATA (3+), CKpan (3+), and Vimentin-. Combined with the results of immunohistochemistry, it was consistent with breast cancer metastasis. Therefore, the mammary gland of the patient was further examined. A physical examination of the patient revealed an orange peel change on the skin of both breasts and a bilateral inverted nipple. Breast ultrasound showed bilateral hyperplasia (BIRADS 4a) of the mammary glands with a reduced echo. Contrast-enhanced breast MRI was precluded by the patient’s compromised renal function and aimed at averting potential adverse reactions to the gadolinium contrast agent, including those associated with nephrogenic systemic fibrosis. Consequently, whole-body 18F-deoxyglucose positron emission tomography/computed tomography (18F-FDG PET/CT) imaging was conducted to pinpoint the most reliable clinical biopsy site. Moreover, 18F-FDG PET/CT proves valuable in distinguishing between benign and malignant lesions, as well as in determining breast cancer staging, grading, and locating primary and metastatic tumor foci. The anteroposterior 3-dimensional maximum intensity projection (MIP) image demonstrated patchy metabolic elevation on both sides of the mammary glands, along with diffusely uneven metabolic foci in both kidneys (Figure 2A). Bilaterally dense mammary glands with a diffuse, mild 18F-FDG uptake were seen, with a maximum standardized uptake value (SUVmax) of 4.7. Bilateral local thickening of the breast skin with an SUVmax of 2.3 was found, which was higher on the right side. BBC was considered (Figure 2B). Enlargement of both kidneys with various degrees of 18F-FDG uptake is found, with an SUVmax at approximately 8.2 (Figure 2C). A patchy soft tissue density lesion is visible around the renal fascia and adjacent to the abdominal aorta, with mild 18F-FDG uptake, and the SUVmax is approximately 3.3 (Figure 2D). Furthermore, diffuse inhomogeneous 18F-FDG uptake was observed in bone lesions, characterized by an SUVmax of approximately 2.9. Additionally, inhomogeneous hyperintensities in bone mineral density were identified in the cones (Figures 2E,F), prompting suspicion of potential bone metastasis. Nevertheless, we cannot definitively exclude the possibility of myelodysplasia, and we will vigilantly monitor this concern during subsequent follow-up assessments. The lesions in the kidneys, bones, and retroperitoneal area were associated with the metastasis of breast cancer.
Figure 2. 18F-FDG PET/CT images. The MIP demonstrated patchy metabolic elevation on both sides of the mammary glands, as well as increased volume in both kidneys, accompanied by a diffusely uneven elevated metabolic lesion (A). The bilateral dense breast tissue shows diffuse mild 18F-FDG uptake, with an SUVmax of approximately 4.7. There is a local thickening of the skin in both breasts, with an SUVmax of 2.3, more prominent on the right side (B). The transverse images show inhomogeneous 18F-FDG uptake in the bilaterally enlarged kidneys, with an SUVmax of approximately 8.2 (C). The transverse images show right perirenal fascia thickening with a significantly higher uptake of an SUVmax of approximately 3.3 (D). The sagittal images show the heterogeneous bone density elevation with radioactive distribution, SUVmax of approximately 2.9 (E,F).
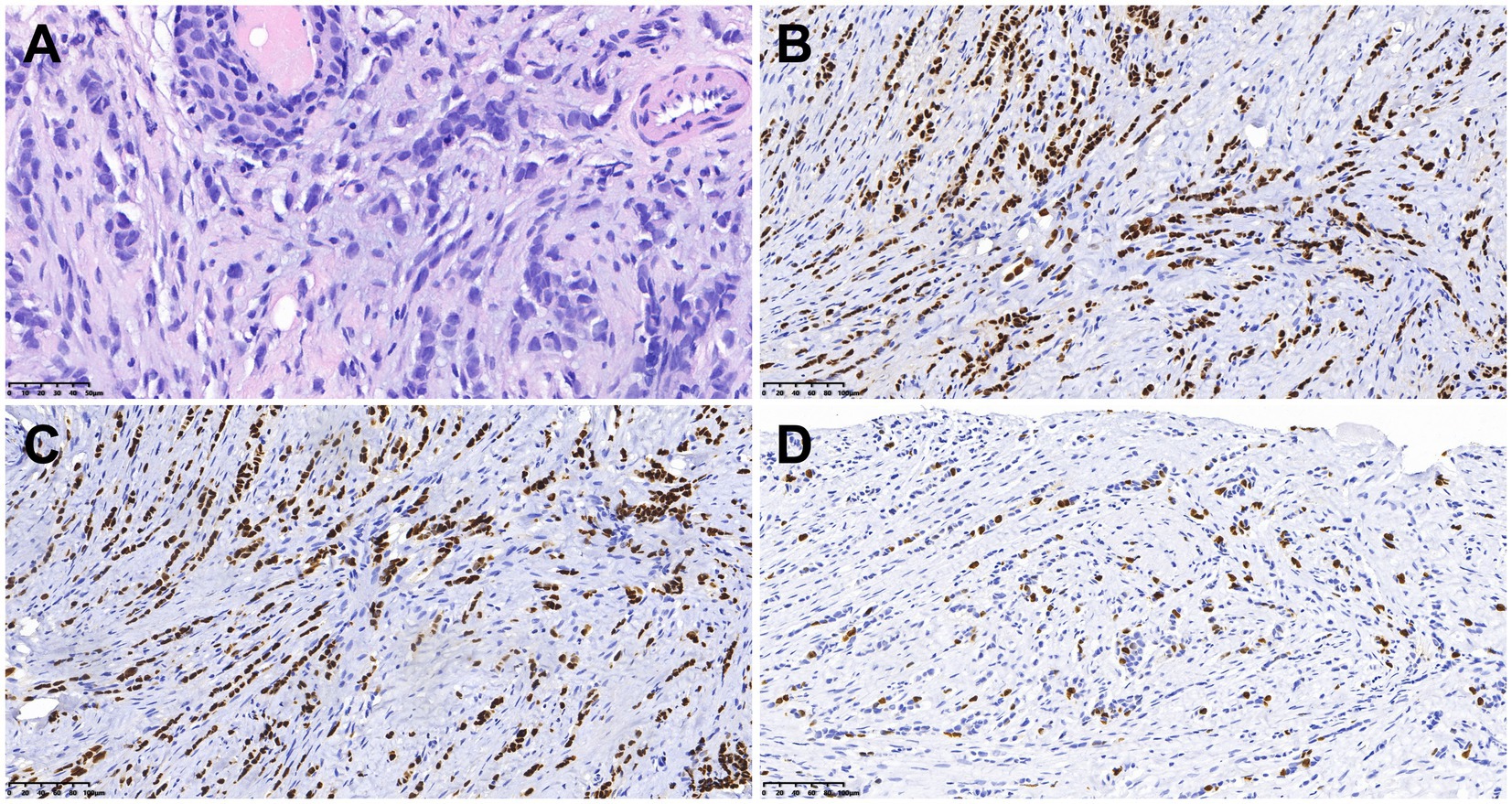
Subsequently, the bilateral mammary glands were examined histologically and immunohistochemically. Pathological examination (Figure 3) revealed grade II invasive lobular carcinoma with ER 90%, PgR 50%, P40-, E-cadherin-, P120++, GATA (3+), Ki67 15%, HER2-, and PD-L1- in both breasts. The clinician diagnosed stage IV invasive breast cancer. The presence of the BRCA1 gene mutation was identified in the germline of the BBC. Renal metastases due to breast cancer were diagnosed on the basis of immunohistochemistry. The patient was ultimately identified as having BBC accompanied by metastases to the bones, kidneys, and retroperitoneal location. Additionally, AKI was observed due to retroperitoneal fibrosis. A week later, after the contraindication of chemotherapy was excluded, the patient was treated with albumin-bound (nab)-paclitaxel (0.3 mg). At present, the chemotherapy has been 11 cycles, and the patient has had no obvious adverse reactions during the course of the chemotherapy. We are still following up.
Figure 3. Histologic and immunohistochemical features of breast cancer. (A) Hematoxylin–eosin (HE) staining (×400). In immunohistochemical staining, the tumor cells were positive for ER (B) and GATA3 (C). Moreover, 15% of them were positive for Ki-67 (D) [magnification (B–D) × 200].
DiscussionBreast cancer represents 24.5% of all cancer cases in women. In 2022, breast cancer will have the highest incidence and mortality in most countries (10). BBC is uncommon and accounts for 1.4–12% of all breast cancers (11). Based on the time interval between the diagnosis of bilateral malignant tumors, BBC can manifest synchronously or asynchronously (12). The primary risk factors associated with BRCA1-related breast cancer include a family history of breast cancer, younger age (under 40 years old), multifocal cancer, a history of lobular carcinoma, inherited genetic mutations such as those in the BRCA1 and BRCA2 genes, and exposure to radiation (13–16). For BRCA1 mutation carriers, the risk of breast cancer increases substantially between the ages of 30 and 50, while for women with a BRCA2 mutation, the risks are highest between ages 40 and 60 (16). BRCA-related breast cancer is characterized by a more aggressive phenotype than sporadic breast cancer, with BRCA1-related breast cancer being more frequently high grade and triple negative, and BRCA2-related breast cancer being on average a higher histological grade than sporadic cases (17). The systematic review and meta-analysis conducted by Baretta et al. (17) showed that mutation carriers have worse overall survival than BRCA-negative/sporadic cases (hazard ratio, HR 1.30, 95% CI: 1.11–1.52) and worse breast cancer-specific survival than sporadic/BRCA-negative cases among patients with stage I–III breast cancer (HR 1.45, 95% CI: 1.01–2.07). In this particular case, the patient had no other risk factors, and genetic testing revealed a mutation in the BRCA1 gene. BRCA1 mutation carriers with breast cancer may benefit from treatment with cisplatinum (18) or olaparib (19) compared to those without a mutation. These data collectively indicate the important role of BRCA mutation status with respect to treatment decisions that may impact outcomes. Genetic mutation detection plays an essential role in the clinical management of breast cancer, as it enables physicians to more accurately identify the molecular characteristics of the disease, formulate personalized treatment plans, and predict the efficacy of therapy and patient prognosis (20, 21). Family members can understand their genetic risks through genetic counseling and undergo appropriate screening and management based on the recommendations of healthcare professionals. Moreover, studies have found that the infiltrating ductal type is the most common histology in BBC (22–24). Some studies indicate that the survival rates of patients with unilateral and BBC are comparable (25, 26). While routine radiological assessments, including mammography and ultrasonography, are conducted for women presenting with suspicious breast symptoms, these methods have certain limitations in diagnosing BBC (27). In addition, contrast-enhanced MRI is forbidden for patients with renal failure. In such a situation, PET/CT, in particular, is instrumental in detecting axillary extra-nodal disease and occult metastasis in patients with locally advanced breast cancer. Its role in assessing responses to neoadjuvant or adjuvant chemotherapy is continually evolving. In the detection of suspected recurrences, it proves more effective than traditional imaging modalities (28).
Retroperitoneal fibrosis is a rare condition of diverse etiology, associated with radiotherapy, aortic aneurysms, infections, and malignancy (29). Eight percent of cases are associated with malignancies (30). Common tumors leading to retroperitoneal fibrosis include breast, lung, gastrointestinal, genitourinary, thyroid, lymphoma, sarcoma, and carcinoid (31). The pathogenic mechanism of peritoneal fibrosis induced by tumors is unknown. It may result from a desmoplastic reaction of the retroperitoneum to malignant cells, an inflammatory reaction, or cytokines secreted by the tumor (30). We have compiled a subset of cases presenting with tumor-associated retroperitoneal fibrosis, and the basic information and clinical details are summarized in Table 1. In the literature, several cases of malignant retroperitoneal fibrosis associated with breast cancer have been documented, with the majority of reported cases featuring a history of breast cancer in the patients (1, 2, 4). Obstructive uropathy is typical of retroperitoneal fibrosis, and bilateral flank pain is the most frequent clinical presentation (1, 2, 4). Our patient presented classic symptoms of bilateral flank pain and hydronephrosis. CT reveals a diffusely infiltrative soft tissue mass enveloping retroperitoneal structures, which is a typical radiological manifestation of retroperitoneal fibrosis (32). 18F-FDG PET/CT can be a valuable tool in evaluating the disease activity and lesion range of retroperitoneal fibrosis and monitoring the treatment of retroperitoneal fibrosis. Furthermore, as illustrated by our cases, in some patients with malignant tumors present with peritoneal fibrosis as the initial manifestation, PET/CT can assist in identifying the primary lesion and accurately staging and grading the condition.
Breast cancer metastasis to the kidneys is rarely seen (33). In one study, the incidence of metastasis of breast cancer to the kidneys was 12% (34). The mechanism of breast cancer metastasis to the kidneys can be attributed to the physiological characteristics of the kidneys. Specifically, the substantial proportion of cardiac output dedicated to renal blood flow makes it likely for circulating tumor cells to enter the renal capillaries (35). Common symptoms of renal metastasis are flank pain and hematuria (36, 37). The most common form of metastatic renal carcinomas is multiple bilaterally circumscribed, rounded masses (35). In patients with known primary tumors, diffuse enlargement of the kidney without a clear mass may suggest renal metastatic disease (38). In this case, the imaging findings were bilaterally enlarged kidneys without focal lesions. However, PET findings indicated various degrees of 18F-FDG uptake in the bilateral kidneys with suspicions of breast cancer metastasis to the kidney, which was agreeable with the pathological diagnosis. In PET/CT imaging, renal metastasis may manifest as small, multiple, bilateral, circular lesions with high 18F-FDG uptake and a diffusely invasive, large, single mass with high 18F-FDG uptake. By the time the primary lesion was detected by PET/CT at some sites, especially tumors prone to renal metastasis (lymphomas and carcinomas of the lung, breast, stomach, pancreas, and colon), there was a high probability of renal involvement. A biopsy for histological analysis was performed if necessary. Conducting a thorough examination of the renal cortex through 18F-FDG PET, coupled with a review of anatomical images such as CT and MRI results, plays a pivotal role in the identification of renal tumors.
ConclusionIn conclusion, we present a case study detailing the 18F-FDG PET/CT imaging manifestations in a BBC patient with retroperitoneal fibrosis and renal metastasis. Compared with conventional imaging, PET can find systemic metastases based on the detection of primary foci, which can be used for disease staging and the evaluation of treatment efficacy.
Data availability statementThe original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Ethics statementWritten informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article. Written informed consent was obtained from the participant/patient(s) for the publication of this case report.
Author contributionsLS: Writing – original draft, Writing – review & editing. YQ: Conceptualization, Writing – original draft. WH: Data curation, Writing – original draft. XS: Investigation, Writing – original draft. QY: Methodology, Writing – original draft. YP: Project administration, Writing – review & editing. LK: Conceptualization, Funding acquisition, Investigation, Project administration, Supervision, Writing – review & editing.
FundingThe author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This study was supported by the National Natural Science Foundation of China (82171970), the Beijing Science Foundation for Distinguished Young Scholars (JQ21025), the Beijing Municipal Science and Technology Commission (Z221100007422027), and the National High-Level Hospital Clinical Research Funding (Interdisciplinary Research Project of Peking University First Hospital, 2023IR17).
Conflict of interestThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s noteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary materialThe Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2024.1353822/full#supplementary-material
References2. MacNeil, JAB, Selegean, S, and Williams, AS. Metastatic lobular carcinoma presenting as retroperitoneal fibrosis: a rare presentation detected using post-mortem cytology. Pathology. (2020) 52:387–90. doi: 10.1016/j.pathol.2019.12.004
PubMed Abstract | Crossref Full Text | Google Scholar
3. Kane, AJ, Wang, ZJ, Qayyum, A, Yeh, BM, Webb, EM, and Coakley, FV. Frequency and etiology of unexplained bilateral Hydronephrosis in patients with breast Cancer: results of a longitudinal Ct study. Clin Imaging. (2012) 36:263–6. doi: 10.1016/j.clinimag.2011.10.001
PubMed Abstract | Crossref Full Text | Google Scholar
4. Gogas, J, Markopoulos, C, Kouskos, E, Gogas, H, and Kiriakou, V. Metastatic retroperitoneal and mediastinal fibrosis as first sign of recurrence of breast cancer. Eur J Surg. (2001) 167:715–8. doi: 10.1080/11024150152619408
PubMed Abstract | Crossref Full Text | Google Scholar
6. Alvarez Argote, J, Bauer, FA, Posteraro, AF 3rd, and Dasanu, CA. Retroperitoneal fibrosis due to B-cell non-Hodgkin lymphoma: responding to rituximab! J Oncol Pharm Pract. (2016) 22:179–85. doi: 10.1177/1078155214543279
Crossref Full Text | Google Scholar
7. Mori, T, Nabeshima, S, Fujino, S, Imoto, A, Shima, H, Yamamoto, K, et al. A case of acute kidney injury due to secondary retroperitoneal fibrosis caused by direct invasion of esophageal squamous cell carcinoma. CEN Case Rep. (2015) 4:185–9. doi: 10.1007/s13730-014-0164-8
PubMed Abstract | Crossref Full Text | Google Scholar
8. Benesch, MGK, and Mathieson, A. Gastric signet-ring-cell adenocarcinoma with delayed retroperitoneal metastasis and fibrosis. Case Rep Oncol. (2022) 15:114–9. doi: 10.1159/000521888
PubMed Abstract | Crossref Full Text | Google Scholar
9. Nishiyama, A, Yoshioka, H, Ikeo, S, Morita, M, Sone, N, Ikeda, S, et al. Retroperitoneal metastasis from lung adenocarcinoma mimics retroperitoneal fibrosis. J Thorac Oncol. (2016) 11:266–7. doi: 10.1016/j.jtho.2015.10.023
PubMed Abstract | Crossref Full Text | Google Scholar
10. Sung, H, Ferlay, J, Siegel, RL, Laversanne, M, Soerjomataram, I, Jemal, A, et al. Global Cancer statistics 2020: Globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2021) 71:209–49. doi: 10.3322/caac.21660
PubMed Abstract | Crossref Full Text | Google Scholar
11. Hartman, M, Czene, K, Reilly, M, Adolfsson, J, Bergh, J, Adami, HO, et al. Incidence and prognosis of synchronous and Metachronous bilateral breast Cancer. J Clin Oncol. (2007) 25:4210–6. doi: 10.1200/jco.2006.10.5056
Crossref Full Text | Google Scholar
12. Mishra, S, Sable, M, Das Majumdar, SK, Mishra, P, Muduly, DK, and Parida, DK. Bilateral breast Cancer-its Clinicopathological profile and management: an experience from a tertiary care center from eastern India. J Cancer Res Ther. (2022) 18:S341–6. doi: 10.4103/jcrt.JCRT_1729_20
PubMed Abstract | Crossref Full Text | Google Scholar
13. Mallory, MA, Whiting, K, Park, A, Gönen, M, Gilbert, E, King, TA, et al. Synchronous and Metachronous bilateral breast Cancer among women with a history of lobular carcinoma in situ. Breast Cancer Res Treat. (2022) 194:137–48. doi: 10.1007/s10549-022-06532-4
PubMed Abstract | Crossref Full Text | Google Scholar
14. El Hanchi, Z, Berrada, R, Fadli, A, Ferhati, D, Brahmi, R, Baydada, A, et al. Bilateral breast Cancer. Incidence and risk factors. Gynecol Obstet Fertil. (2004) 32:128–34. doi: 10.1016/j.gyobfe.2003.01.002
Crossref Full Text | Google Scholar
15. Wang, YA, Jian, JW, Hung, CF, Peng, HP, Yang, CF, Cheng, HS, et al. Germline breast Cancer susceptibility gene mutations and breast Cancer outcomes. BMC Cancer. (2018) 18:315. doi: 10.1186/s12885-018-4229-5
PubMed Abstract | Crossref Full Text | Google Scholar
17. Baretta, Z, Mocellin, S, Goldin, E, Olopade, OI, and Huo, D. Effect of Brca germline mutations on breast Cancer prognosis: a systematic review and Meta-analysis. Medicine. (2016) 95:e4975. doi: 10.1097/md.0000000000004975
PubMed Abstract | Crossref Full Text | Google Scholar
18. Byrski, T, Gronwald, J, Huzarski, T, Grzybowska, E, Budryk, M, Stawicka, M, et al. Pathologic complete response rates in young women with Brca1-positive breast cancers after neoadjuvant chemotherapy. J Clin Oncol. (2010) 28:375–9. doi: 10.1200/jco.2008.20.7019
PubMed Abstract | Crossref Full Text | Google Scholar
19. Lee, JM, Ledermann, JA, and Kohn, EC. Parp inhibitors for Brca1/2 mutation-associated and Brca-like malignancies. Ann Oncol. (2014) 25:32–40. doi: 10.1093/annonc/mdt384
Crossref Full Text | Google Scholar
20. Kuchenbaecker, KB, Hopper, JL, Barnes, DR, Phillips, KA, Mooij, TM, Roos-Blom, MJ, et al. Risks of breast, ovarian, and contralateral breast Cancer for Brca1 and Brca2 mutation carriers. JAMA. (2017) 317:2402–16. doi: 10.1001/jama.2017.7112
Crossref Full Text | Google Scholar
22. Li, B, Xu, W, Cao, J, Guo, D, Tao, Z, Jin, J, et al. A study of clinical and molecular characteristics in bilateral primary breast Cancer. Cancer Med. (2023) 12:15881–92. doi: 10.1002/cam4.6226
PubMed Abstract | Crossref Full Text | Google Scholar
23. Vuoto, HD, García, AM, Candás, GB, Zimmermann, AG, Uriburu, JL, Isetta, JA, et al. Bilateral breast carcinoma: clinical characteristics and its impact on survival. Breast J. (2010) 16:625–32. doi: 10.1111/j.1524-4741.2010.00976.x
PubMed Abstract | Crossref Full Text | Google Scholar
24. Li, CI, Malone, KE, Porter, PL, and Daling, JR. Epidemiologic and molecular risk factors for contralateral breast Cancer among young women. Br J Cancer. (2003) 89:513–8. doi: 10.1038/sj.bjc.6601042
PubMed Abstract | Crossref Full Text | Google Scholar
25. Nichol, AM, Yerushalmi, R, Tyldesley, S, Lesperance, M, Bajdik, CD, Speers, C, et al. A case-match study comparing unilateral with synchronous bilateral breast Cancer outcomes. J Clin Oncol. (2011) 29:4763–8. doi: 10.1200/jco.2011.35.0165
PubMed Abstract | Crossref Full Text | Google Scholar
26. Irvine, T, Allen, DS, Gillett, C, Hamed, H, and Fentiman, IS. Prognosis of synchronous bilateral breast Cancer. Br J Surg. (2009) 96:376–80. doi: 10.1002/bjs.6553
Crossref Full Text | Google Scholar
27. Johnson, L, Pinder, S, and Douek, M. Multiple foci of invasive breast Cancer: can breast Mri influence surgical management? Breast Cancer Res Treat. (2011) 128:1–5. doi: 10.1007/s10549-011-1491-5
Crossref Full Text | Google Scholar
29. Carloss, H, and Saab, G. Breast Cancer and retroperitoneal metastasis. South Med J. (1980) 73:1570–1. doi: 10.1097/00007611-198012000-00009
Crossref Full Text | Google Scholar
30. Vega, J, Ceriani, A, and Jensen, D. Retroperitoneal fibrosis associated with malignancies: report of eight cases. Rev Med Chile. (2014) 142:791–8. doi: 10.4067/s0034-98872014000600015
PubMed Abstract | Crossref Full Text | Google Scholar
32. Kim, J, Hwang, JH, Nam, BD, Park, YW, and Jeen, YM. Mediastinal and retroperitoneal fibrosis as a manifestation of breast Cancer metastasis: a case report and literature review. Medicine (Baltimore). (2018) 97:e11842. doi: 10.1097/md.0000000000011842
PubMed Abstract | Crossref Full Text | Google Scholar
33. Huo, Z, Gao, Y, Yu, Z, Zuo, W, and Zhang, Y. Metastasis of breast cancer to renal cancer: report of a rare case. Int J Clin Exp Pathol. (2015) 8:15417–21.
PubMed Abstract | Google Scholar
34. Abrams, HL, Spiro, R, and Goldstein, N. Metastases in carcinoma; analysis of 1000 autopsied cases. Cancer. (1950) 3:74–85. doi: 10.1002/1097-0142(1950)3:1<74::aid-cncr2820030111>3.0.co;2-7
PubMed Abstract | Crossref Full Text | Google Scholar
35. Ahmed, Y, Aynaou, M, El Houmaidi, A, Mhanna, T, Tombet, C, and Barki, A. Breast Cancer metastatic to the kidney: case report. Urol Case Rep. (2020) 33:101302. doi: 10.1016/j.eucr.2020.101302
PubMed Abstract | Crossref Full Text | Google Scholar
36. Cazacu, SM, LD, SĂ, Mitroi, G, Neagoe, DC, Streba, C, and Albulescu, DM. Metastases to the kidney: a case report and review of the literature. Curr Health Sci J. (2020) 46:80–9. doi: 10.12865/chsj.46.01.11
PubMed Abstract | Crossref Full Text | Google Scholar
37. Zhou, C, Urbauer, DL, Fellman, BM, Tamboli, P, Zhang, M, Matin, SF, et al. Metastases to the kidney: a comprehensive analysis of 151 patients from a tertiary referral Centre. BJU Int. (2016) 117:775–82. doi: 10.1111/bju.13194
PubMed Abstract | Crossref Full Text | Google Scholar
38. Srisung, W, Mankongpaisarnrung, C, Warraich, I, Sotello, D, Yarbrough, S, and Laski, M. Carcinoma of the lungs causing enlarged kidneys. Proc (Baylor Univ Med Cent). (2015) 28:221–3. doi: 10.1080/08998280.2015.11929235
留言 (0)