
記住我






This Institutional Review Board-approved prospective pilot study was conducted at a urogynecology clinic in a tertiary care hospital in metropolitan Los Angeles between April 2021 and December 2022.
English-speaking cisgender women aged 18 to 80 years with sexual dysfunction, pelvic floor disorder, and/or genitourinary syndrome of menopause were recruited for participation in the urogynecological clinic via direct referrals, intra-organizational email communication, and social media. Exclusion criteria included women who were non-English speaking, not assigned female at birth, had a history of genital gender-affirming surgeries, had a history of genital mutilation, were currently pregnant, within 6 months postpartum, or who had medical or mental health conditions affecting their dexterity and ability to operate the vibrator.
Standardized screening interviews were conducted either in person or via phone by research personnel. Screening interviews included questions about gender, the presence of any pelvic floor disorders, sexual dysfunction, and interest in participation in the study. Conditions categorized as sexual dysfunction in this study included hypoactive sexual desire disorder, decreased arousal, decreased lubrication, and absent or muted orgasm. The conditions included in the pelvic floor disorders were stress urinary incontinence, urge urinary incontinence, pelvic organ prolapse, interstitial cystitis, pelvic floor dysfunction (hypertonic pelvic floor), genitourinary syndrome of menopause, and skin dermatoses.
After informed consent was signed, demographic information was obtained, including age, menopausal status, hormone therapy history, medical history, and sexual history. Sexual function was assessed using the Female Sexual Function Index (FSFI) and the Pelvic Organ Prolapse/Urinary Incontinence Sexual Questionnaire IUGA-Revised (PISQ-IR). The FSFI is a validated 19-item measure of sexual function in four domains: desire, arousal, orgasm, and sexual pain. The total score ranges from 0 to 36, with higher scores indicating better sexual functioning. A total score below 26.6 indicates clinical Female Sexual Dysfunction (FSD). The PISQ-IR is a validated measure of sexual function among sexually active women with and without a partner. This questionnaire contains 20 questions and is used to assess sexual activity in women with urinary incontinence and pelvic organ prolapse. Higher scores indicated better sexual function.
Pelvic floor function was assessed with the following validated questionnaires: Pelvic Floor Disability Index, Female Genitourinary Pain Index (F-GUPI), and the Interstitial Cystitis Symptoms Index/Interstitial Cystitis Problem Index (ICSI-ICPI). The Pelvic Floor Distress Inventory (PFDI) is a condition-specific quality-of-life questionnaire for women with bowel, bladder, and/or pelvic symptoms. The scores ranged between 0 and 300, with higher scores indicating more severe distress. The F-GUPI is used to assess symptom severity and impact in women with genitourinary pain complaints. The score ranges from 0 to 45, and is the sum of the individual scores for the domains of pain, urinary symptoms, and impact on quality of life. The ICSI-ICPI is the sum of four items that measure urinary urgency, frequency, night-time urination, and pain/burning. In addition, participants were asked if they had a prolapse and the degree of bother it caused. Responses from questionnaires, physical examinations, and subjective reports were all recorded and assessed at the initial appointment and follow-up.
Mental health and quality of life were assessed using the Patient Health Questionnaire (PHQ9) and the Health-Related Quality of Life-Short Form (SF12) respectively. The PHQ9 is a validated tool for the assessment of depression. Depression severity was assessed by summarizing the scores assigned to each category. Scores range between 1 and 27, with higher scores correlating with more severe depression. The SF12 is a general health measure that assesses the impact of health on everyday life. The SF12 consists of eight domains and generates two separate summary scores, physical functional scores (PCS), and mental function scores (MCS), each ranging from 0 to 100. Higher scores indicate better health-related quality of life.
A baseline pelvic examination was performed to evaluate vulvar dermatoses, vaginal epithelium changes, pelvic organ prolapse, urinary or anal incontinence, pelvic floor muscle strength, and trigger points. The presence and severity of vaginal atrophy were recorded based on examiner assessment on a scale of 1 to 3, corresponding to mild, moderate, and severe changes respectively. This classification was based on the degree of anatomical changes in the genitalia that have been routinely used in our practice, as no validated tool has been developed to date. The assessment included the color and friability of the tissue, the amount of vaginal lubrication, the presence of a urethral caruncle, the presence of rugae, elasticity, vaginal caliber, resorption or fusion of the labia majora and/or minora, and introital retraction [14]. Similarly, the presence and severity of lichen sclerosus were recorded based on examiner assessment on a scale of 1 to 3, corresponding to mild, moderate, and severe respectively. This classification was based on the amount of involved skin, as no validated tools have been developed to date, and it has been routinely used in our practice. The assessment of vaginal tissue assessment was performed by the same examiner. Pelvic organ prolapse was assessed by the examiner and categorized based on the Baden–Walker Halfway Scoring System. To mitigate potential bias, all assessment measurements were recorded during the examination, and the investigator was not allowed to review the initial examination findings prior to seeing the study participants at their 3-month follow-up visit.
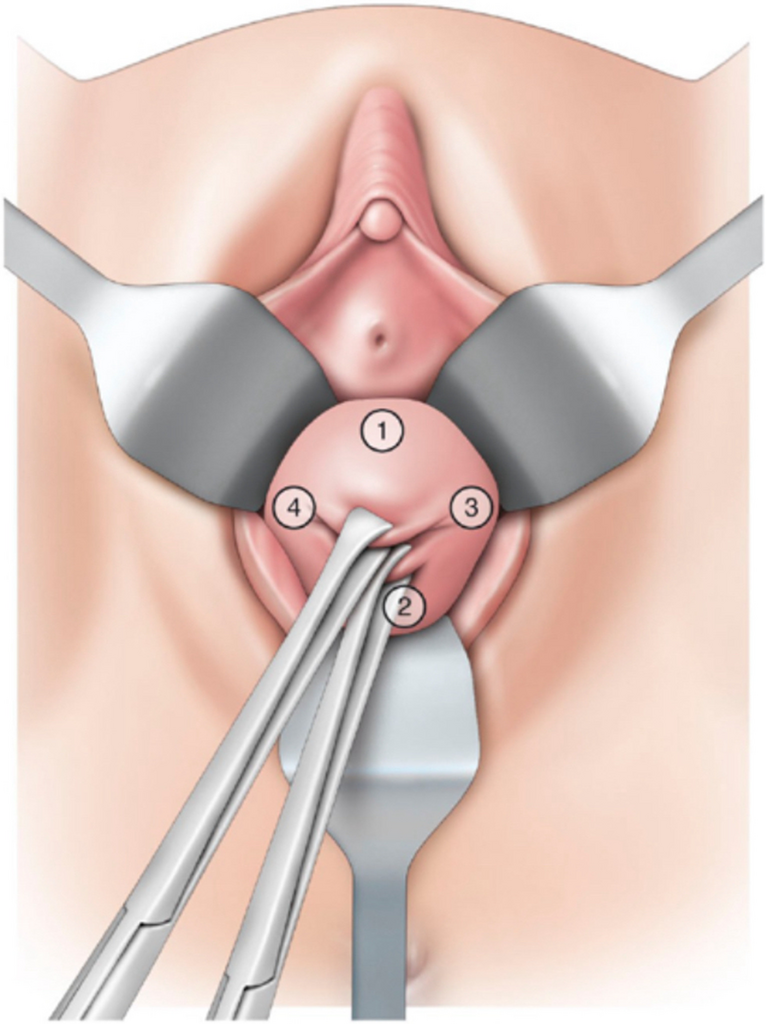
After baseline data collection, women were given a multimodal bullet vibrator (Fig. 1) and were instructed to apply it to their external genitalia for 5–10 min, two to three times per week for 3 months. Participants were encouraged to focus on adhering to the protocol rather than on reaching an orgasm. They were also advised to use a vibrator to determine whether they felt sexual desire or interest. Setting reminder alarms on their smartphones is highly encouraged. Each woman was given a calendar diary to track her vibrator use and any additional sexual encounter. Participants were encouraged to use the vibrator alone and with their partners. Instruction on safe use and cleaning was discussed and provided in a written form. Women who had never masturbated or were not familiar with their anatomy were educated by research personnel and recommended to visit the Betty Dodson website (https://www.dodsonandross.com/sexfeature/first-time-orgasm?utm_source=www.dodsonandross.com), as her method of achieving an orgasm has been evaluated and demonstrated to be effective [8]. Women were also given information on lubricants and their compatibility with the vibrator (Appendix 1, Supplemental Material). Women were not compensated for participation, but were allowed to keep the vibrator after the completion of the study.
Fig. 1
The primary outcomes of this pilot study were the effects of regular vibrator use on sexual function, pelvic floor disorders/genitourinary function, and mental health, including health-related quality of life. Secondary outcomes were the identification of any demographic or health-related differences between the participants who completed the study and those who dropped out.
Changes in pelvic floor disorders/genitourinary health, sexual function, and mental health from baseline to the 3-month follow-up were tested using a McNemar test for dichotomous data, a paired t test for normally distributed data, or a Wilcoxon sign test for rank data. Statistical analysis was performed using SAS v9.4, and statistical significance was set at p < 0.05. Differences in demographics and questionnaire-based data between participants who completed the study and those who dropped out were tested using a Chi-squared test for categorical data, a two-sample t test for normally distributed data, or a Wilcoxon rank sum test, as appropriate. This study was designed as a pilot study to collect data for future in-depth investigations; therefore, no power analysis was performed.
留言 (0)