Importance
Macrosomia represents the most significant risk factor of shoulder dystocia (SD), which is a severe and emergent complication of vaginal delivery. They are both associated with adverse pregnancy outcomes.
Objective
The aim of this study was to review and compare the most recently published influential guidelines on the diagnosis and management of fetal macrosomia and SD.
Evidence Acquisition
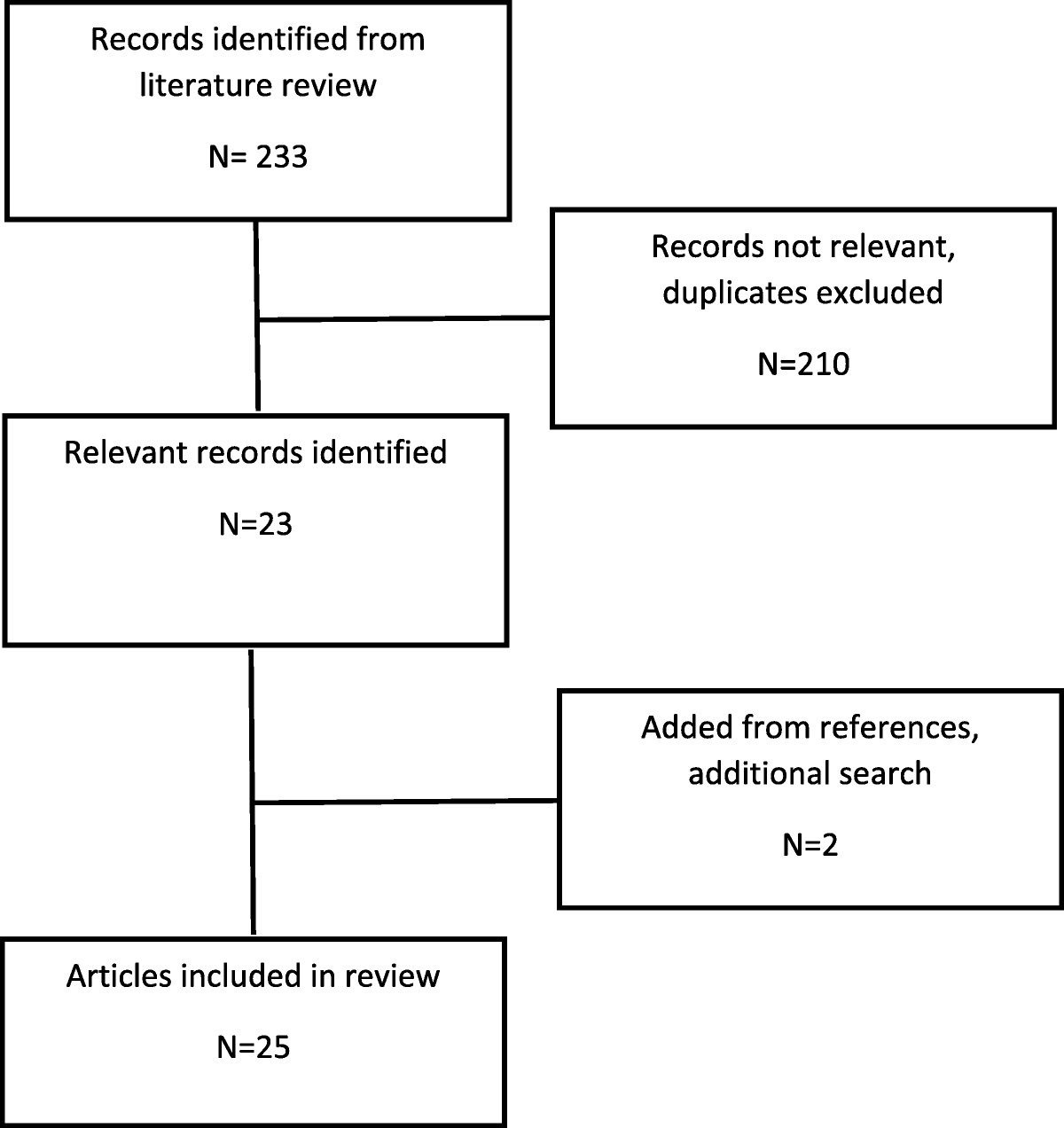
A comparative review of guidelines from the American College of Obstetricians and Gynecologists (ACOG), the Royal College of Obstetricians and Gynaecologists, the National Institute for Health and Care Excellence, the Royal Australian and New Zealand College of Obstetricians and Gynaecologists (RANZCOG), and the Department for Health and Wellbeing of the Government of South Australia on macrosomia and SD was conducted.
Results
The ACOG and RANZCOG agree that macrosomia should be defined as birthweight above 4000–4500 g regardless of the gestational age, whereas the National Institute for Health and Care Excellence defines macrosomia as an estimated fetal weight above the 95th percentile. According to ACOG and RANZCOG, ultrasound scans and clinical estimates can be used to rule out fetal macrosomia, although lacking accuracy. Routine induction of labor before 39 weeks of gestation with the sole indication of suspected fetal macrosomia is unanimously not recommended, but an individualized counseling should be provided. Exercise, appropriate diet, and prepregnancy bariatric surgery are mentioned as preventive measures. There is also consensus among the reviewed guidelines regarding the definition and the diagnosis of SD, with the “turtle sign” being the most common sign for its recognition as well as the poor predictability of the reported risk factors. Moreover, there is an overall agreement on the algorithm of SD management with McRoberts technique suggested as first-line maneuver. In addition, appropriate staff training, thorough documentation, and time keeping are crucial aspects of SD management according to all medical societies. Elective delivery for the prevention of SD is discouraged by all the reviewed guidelines.
Conclusions
Macrosomia is associated not only with SD but also with maternal and neonatal complications. Similarly, SD can lead to permanent neurologic sequalae, as well as perinatal death if managed in a suboptimal way. Therefore, it is crucial to develop consistent international practice protocols for their prompt diagnosis and effective management in order to safely guide clinical practice and improve pregnancy outcomes.
Target Audience
Obstetricians and gynecologists, family physicians.
Learning Objectives
After participating in this activity, the learner should be better able to describe fetal macrosomia; identify risk factors and early signs of shoulder dystocia; and discuss appropriate techniques for the management of fetal macrosomia and shoulder dystocia.




留言 (0)