
記住我

Refractory heart failure (RHF), also known as intractable heart failure or end-stage heart failure, refers to a group of clinical syndromes in which patients, after standardized management and treatment, remain unable to be effectively controlled or deteriorate even further; their condition is recurrent, requires repeated hospitalization, and has a high mortality rate (1, 2). In recent years, the prevalence of heart failure has continuously increased, and the number of patients with RHF has also increased. Epidemiology shows that the number of people with heart failure has reached as high as 64.3 million worldwide (3), of which RHF accounts for approximately 6%–25% (4–6). Currently, although advanced means, such as implantation of ventricular assist devices, surgical ventricular remodeling, and cardiac transplantation, are available for the treatment of RHF, medication is still the main treatment modality (7). The main drugs used in the clinical treatment of RHF are diuretics, inotropic agents, vasodilators, and neuroendocrine inhibitors. Even though these drugs can effectively improve patients’ clinical symptoms, long-term use can lead to adverse reactions and even worsen heart failure, exacerbating the condition (8). Therefore, how to find new targets for the treatment of heart failure, prevent and delay myocardial remodeling and then reduce the rehospitalization rate and mortality of patients with RHF, and improve the quality of survival is still the hotspot and difficult point in the field of cardiovascular research at present.
In recent years, the traditional Chinese medicine (TCM) treatment for RHF has increasingly been reported. Clinical studies have shown that the combined use of TCM based on the conventional treatment of Western medicine is superior to the treatment of Western medicine alone in improving clinical symptoms, such as chest tightness and shortness of breath, fatigue, dyspnea, and urine oligoedema, in patients with RHF, improving exercise tolerance and improving long-term outcomes. In this article, we systematically summarize the clinical evidence and the mechanism of action of TCM for the treatment of RHF, as well as the scientific problems that exist in TCM for the treatment of RHF, to provide a reference for the clinical treatment of RHF.
2 TCM in the treatment of RHF 2.1 Understanding RHF in TCM theoryThere is no specific record of RHF in ancient Chinese medicine, and according to its clinical manifestations, it can be classified as “palpitation,” “severe palpitation,” “asthma,” “edema,” and other categories. At present, there is a lack of systematic research on the characteristics of TCM syndromes in RHF, and clinical physicians tend to equate it with heart failure. Although RHF belongs to HF, it is in the end stage of the disease, and the treatment is more difficult. The characteristics of RHF syndrome are indeed different from those of heart failure. There is no unified understanding of the etiology, pathogenesis, and characteristics of this disease in TCM. Based on the literature, some scholars classify the TCM characteristics of RHF as a deficiency in origin and excess in superficiality, and the combination of deficiency and excess. The deficiency in origin is mainly Yang deficiency, and the excess in superficiality is mainly blood stasis and water retention. Some scholars believe that the main pathogenesis of RHF is heart-kidney Yang deficiency and the combination of blood stasis and water (9). The principle of treatment should balance the priorities, tonify deficiency, and reduce excess. The first step in treatment is to support the Yang deficiency and consolidate the foundation, dissipate blood stasis, and promote diuresis, while also regulating qi and dispersing stasis, resolving phlegm and removing blood stasis, and capturing and promoting drinking (10).
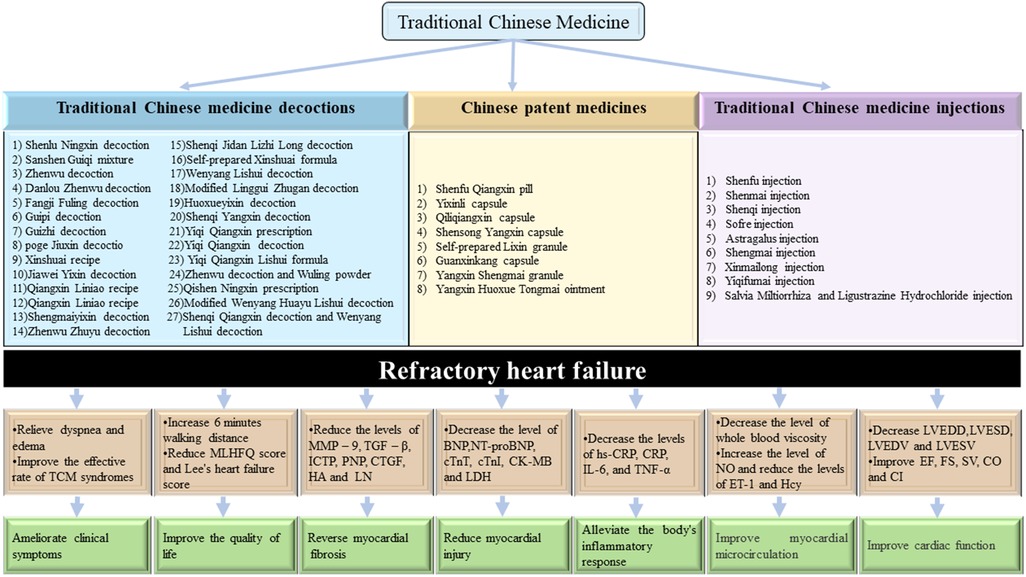
2.2 Clinical evidence of TCM for RHFThis article summarizes 58 representative randomized controlled trials (RCTs), including 28 TCM decoctions, 12 Chinese patent medicines (CPMs), and 18 TCM injections. According to the available clinical data, there have been many clinical trials on the clinical advantages of TCM in the prevention and treatment of RHF, as shown in Figure 1. Supplementary Table S1 summarizes the clinical evidence for the TCM treatment of RHF, including (1) clinical manifestations, (2) cardiac function indexes, and (3) laboratory results.
Figure 1. Clinical evidence of TCM for RHF.
2.2.1 TCM decoctions for RHF treatmentClinical symptoms
(1) Shenlu Ningxin decoction (11), modified Linggui Zhugan decoction (12), Shenqi Qiangxin decoction and Wenyang Lishui decoction (13), Danlou Zhenwu decoction (14), modified Wenyang Huayu Lishui decoction (15), Zhenwu Zhuyu decoction (16), Yiqi Qiangxin Lishui formula (17), Jiawei Yixin decoction (18), and Wenyang Lishui decoction (19) can all improve symptoms of palpitations, chest tightness, wheezing, shortness of breath, and fatigue in patients. Shenlu Ningxin decoction (11), self-prepared Xinshuai formula (20), and Yiqi Qiangxin prescription (21) can improve symptoms such as palpitations, bloating, suffocation, cyanosis of the lips, and chills in the limbs of patients. Shenqi Qiangxin decoction and Wenyang Lishui decoction (13) and Yiqi Qiangxin Lishui formula (17) can improve symptoms such as difficulty breathing, poor appetite, and urinary edema in patients. Yiqi Qiangxin decoction (22), modified Wenyang Huayu Lishui decoction (15), and Zhenwu Zhuyu decoction (23) can all slow down heart rate; Poge Jiuxin decoction (24) and self-prepared Xinshuai formula (20) can reduce Lee's heart failure score. Shenlu Ningxin decoction (11), Jiawei Yixin decoction (18), and Yiqi Qiangxin prescription (21) reduce the Minnesota Living with Heart Failure Questionnaire (MLHFQ) and improve patients’ quality of life. Zhenwu Zhuyu decoction (16), Shenqi Yangxin decoction (25), and Danlou Zhenwu decoction (14) can increase walking distance by 6 min and improve exercise tolerance.
Echocardiography
(2) Shenlu Ningxin decoction (11), Shenqi Jidan Lizhi Long decoction (26), Shenqi Qiangxin decoction and Wenyang Lishui decoction (13), Danlou Zhenwu decoction (14), Guipi decoction (27), modified Wenyang Huayu Lishui decoction (15), modified Linggui Zhugan decoction (12), Jiawei Yixin decoction (18), Wenyang Lishui decoction (19), Fangji Fuling decoction (28), Shenqi Yangxin decoction (25), Yiqi Qiangxin prescription (21), Dingchuan decoction (29), and Qishen Ningxin prescription (30) can improve heart function, reduce left ventricular end diastolic diameter (LVEDD), and left ventricular end-systolic diameter (LVESD), reduce left ventricular end-systolic volume (LVESV) and increase left ventricular ejection fraction (LVEF). Shenqi Jidan Lizhi Long decoction (26), Jiawei Yixin decoction (18), Poge Jiuxin decoction (24), and Yiqi Qiangxin decoction (22) increase the heart index (CI). Guizhi decoction (31), Zhenwu Zhuyu decoction (16), and Yiqi Qiangxin prescription (21) increase cardiac output (CO). Shenlu Ningxin decoction (11), Danlou Zhenwu decoction (14), Guizhi decoction (31), Zhenwu Zhuyu decoction (16), and Zhenwu decoction (32) increase stroke volume (SV).
Biochemical indicators
(3) Shenlu Ningxin decoction (11), Danlou Zhenwu decoction (14), Guipi decoction (27), Guizhi decoction (31), Jiawei Yixin decoction (18), Shengmaiyixin decoction (33), Sanshen Guiqi mixture (34), Zhenwu Zhuyu decoction (23), Shenqi Yangxin decoction (25), modified Wenyang Huayu Lishui decoction (15), Poge Jiuxin decoction (24), Wenyang Lishui decoction (19), Xinshuai recipe (35), Yiqi Qiangxin Lishui formula (17), and Dingchuan decoction (29) can significantly reduce N-terminal pro-B-type natriuretic peptide (NT-proBNP) or brain natriuretic peptide (BNP). Zhenwu Zhuyu Decoction (23) can significantly reduce inflammatory factors, such as tumor necrosis factor-α (TNF-α), interleukin-6 (IL-6), and C-reactive protein (CRP). Shenlu Ningxin Decoction (11) reduced the levels of transforming growth factor-β1 (TGF-β1) and matrix metalloproteinase-9 (MMP-9). Guizhi decoction (31) can increase 24 h urine volume and serum sodium and reduce serum creatinine. Qiangxin Liniao recipe (36) can accelerate the improvement of symptoms such as hypotension, renal insufficiency, and insufficient blood volume. Zhenwu Zhuyu Decoction (23), Huoxueyixin decoction (37), Zhenwu decoction, and Wuling powder (38) can reduce the levels of whole blood low shear viscosity, whole blood high shear viscosity, fibrinogen, and plasma viscosity.
2.2.2 TCM patent medicines for RHF treatmentClinical symptoms
(1) The Qiliqiangxin capsule (39), Yangxin Huoxue Tongmai ointment (40), Yixinli capsule (41), and self-prepared Lixin granule (42) improved the condition of patients with RHF and reduced cardiovascular dysfunctions. The most typical clinical symptoms include palpitations, shortness of breath and chest tightness, wheezing, fatigue, cough and expectoration, and edema. Self-prepared Lixin granule (42) improved the symptoms of jugular vein distension and bilateral lung moist rales. The Yixinli capsule (41), Yangxin Shengmai granule (43), and Qiliqiangxin capsule (44) can increase the 6-min walking distance (6MWD) and improve exercise tolerance. In addition, the Qiliqiangxin capsule (45) can improve the quality of life of patients and reduce the readmission rate.
Echocardiography
(2) The Shenfu Qiangxin pill (46, 47), Qiliqiangxin capsule (45), Yangxin Huoxue Tongmai ointment (40), Yixinli capsule (41), Shensong Yangxin capsule (48), Guanxinkang capsule (49), and self-prepared Lixin granule (42) can increase LVEF and reduce LVESD, LVEDD, LVESV, and left ventricular end diastolic volume (LVEDV). The Qiliqiangxin capsule (39) can increase CI, SV, myocardial contractility, and venous return blood volume. The Yixinli capsule (41) and Yangxin Huoxue Tongmai ointment (40) improve the grading evaluation of heart function.
Biochemical indicators
(3) The Shenfu Qiangxin pill (46), Qiliqiangxin capsule (39), and Shensong Yangxin capsule (48) can significantly reduce the level of serum NT-proBNP. The Shenfu Qiangxin pill (46) and Shensong Yangxin capsule (48) can reduce the levels of serum cTnT and cTnI. The Shenfu Qiangxin pill (47) reduces the serum levels of heart-fatty acid binding protein (H-FABP), creatine kinase myocardial bound (CK-MB), procollagen type I carboxy terminal peptide (ICTP), type III procollagen amino terminal peptide (PIIINP), connective tissue growth factor (CTGF), hyaluronic acid (HA), and laminin (LN) in patients. The Qiliqiangxin capsule (39, 50) can increase total cholesterol (TC), triglyceride (TG), low-density lipoprotein cholesterol (LDL-C) levels, reduce high density lipoprotein (HDL-C) indicators, and regulate blood lipid levels. In addition, the Shensong Yangxin capsule (48) can reduce the levels of inflammatory mediator hypersensitive C-reactive protein (hs-CRP).
2.2.3 TCM injections for RHF treatmentClinical symptoms
(1) Shenfu injection (51), Astragalus injection (52), Shengmai injection (53), Xinmailong injection (54), and Sofre injection (55) can improve the clinical total effective rate, and improve the clinical symptoms, such as shortness of breath and fatigue, chest tightness and suffocation, tachypnea, palpitation, lower limb edema, and so on. Shengmai injection (56) can alleviate symptoms such as systemic fatigue, lower limb edema, and liver enlargement, as well as alleviate symptoms of total heart failure, such as jugular vein dilation and purple forceps. Shenfu injection (51), Shenmai injection (57), Sofre Injection (55), Xinmailong injection (58), and Yiqifumai injection (59) can increase the 6-min walking distance of patients and improve exercise endurance. Astragalus injection (52) and Sofre injection (55) can shorten hospitalization time and reduce the rate of readmission. Shenfu injection (51) and Xinmailong injection (60) can improve TCM syndrome scores and Minnesota Heart Failure Quality of Life Questionnaire scores, and improve quality of life.
Echocardiography
(2) Shenfu injection (61–63), Shenmai injection (57, 64), Astragalus injection (65), Sofre Injection (55), and Xinmailong injection (54) improve cardiac function, reduce LVEDD, LVEDV, LVESD, and LVESV levels, increase fraction shortening (FS) levels, and increase LVEF. Shenfu injection (61, 62), Shenmai injection (64, 66), Sofre injection (55), and Salviae Miltiorrhizae and Ligustrazine Hydrochloride injection (67) can increase SV. Shenfu injection (63) and Shenmai injection (57, 64) increase the output per minute (CO). Shenmai injection (57, 64) and Sofre injection (55) increased the CI level.
Biochemical indicators
(3) Shenfu injection (51, 61), Shenqi injection (68), Astragalus injection (65), Salviae Miltiorrhizae and Ligustrazine Hydrochloride injection (67), Xinmailong injection (58, 69), and Yiqifumai injection (59) can reduce the levels of NT-proBNP or BNP. Shenfu injection (61–63) can reduce the levels of inflammatory factors hs-CRP and IL-6, and it can also reduce the levels of CK-MB, cTnT, E-selection (ES), and H-FABP, and alleviate myocardial injury. Shenqi injection (68, 70) can reduce the myocardial enzymes lactate dehydrogenase (LDH), aspartate aminotransferase (AST), alanine aminotransferase (ALT), CK-MB, Hydroxybutyrate dehydrogenase (HBDH), and myocardial fibrosis TGF-β1, CTGF, Recombinant Procollagen I C-Terminal Propeptide (PICP), type I pro-hydroxy terminal cross linked peptide (CITP), and PIIINP related indicators, and reduce myocardial fibrosis to protect cardiomyocytes. Shenmai injection (66), Astragalus injection (65), and Xinmailong injection (54) can reduce cTnI levels. Astragalus injection (52, 65) can improve ventricular remodeling, reduce pulmonary artery systolic pressure (SPAP), increase PaO2, SaO2, force expiratory volume in 1 s (FEV1), and effectively expand blood vessels, improve pulmonary microcirculation and systemic hypoxia, and reduce heart load. Xinmailong injection (58) can improve pulmonary artery systolic pressure (PASP), mean pulmonary artery pressure (MPAP), endothelin (ET), nitric oxide (NO), thromboxane (TXA2), and prostacyclin (PGI2), reduce pulmonary artery pressure, and alleviate vascular endothelial function damage. Salviae Miltiorrhizae and Ligustrazine Hydrochloride injection (67) increased systolic blood pressure (SBP), diastolic blood pressure (DBP), and estimated glomerular filtration rate (eGFR) levels, decreased plasma renin activity, angiotensin II, serum creatinine (SCr), and aldosterone (ALD) levels, and inhibited the activation of renin-angiotensin-aldosterone system (RAAS).
2.2.4 Other traditional alternative strategies for RHF treatmentOne of the unique advantages of traditional Chinese medicine treatment lies in the combination of internal and external treatments. In addition to internal treatment, external treatment methods, such as acupuncture, Tai Chi exercise, Baduanjin exercise, and acupoint application, also play a role in the treatment of heart failure. A systematic review and meta-analysis of 32 RCTs involving 2,499 patients revealed that integrated acupuncture and Western medicine therapies were more effective than Western medicine treatments alone regarding the indicators of efficacy rate, LVEF, improved 6MWD, MLHFQ, and CO (71). Multiple meta-analyses showed that heart failure patients took Tai Chi rehabilitation exercise on the basis of conventional drug treatment. After 6 months of treatment, quality of life, cardiac function grading, 6MWD, LVEF, and LVEDD in the treatment group was significantly better than that of the control group (72, 73). Clinical research (74, 75) reported that, compared with taking conventional drugs alone, conventional Western medicine combined with Ba Duan Jin's comprehensive treatment can significantly improve patients’ BNP, metabolic equivalents (METs), maximum oxygen consumption (VO2Max), 6MWD, New York Heart Association (NYHA) classification, LVEF, TCM symptoms, quality of life, and other indicators, and the degree of improvement is obviously better than that of the control group. A clinical study by Huang et al. (76) reported that acupoint application can significantly improve clinical symptoms, cardiac function, and quality of life, and reduce the level of NT-proBNP.
In summary, the clinical evidence suggests that TCM is beneficial for the treatment of RHF. First, TCM improves the clinical symptoms of patients, including alleviating symptoms such as dyspnea, cough and expectoration, chest tightness and shortness of breath, shortness of breath, palpitation and palpitation, and intractable edema, while improving cardiopulmonary function. It also attenuates signs of global heart failure, such as jugular vein irritability and purple forceps, and can improve the patient's 6-min walking distance and exercise tolerance. It can improve the symptoms of traditional Chinese medicine, the total effective rate of clinical efficacy, and the quality of life of patients, shorten the length of stay and reduce the rate of readmission. Second, TCM improves cardiac function, including increased LVEF levels and FS levels, and decreased LVEDV, LVESD, and LVESV levels, increased SV, CO, and CI levels, and enhanced cardiac contractility. Third, TCM improves biochemical parameters as follows: lowers indexes of myocardial zymography, LDH, AST, ALT, CK-MB, HDBH, and decreases myocardial injury; decreases SPAP, increases PaO2, SaO2, and FEV1, improves microcirculation and systemic hypoxia in the lungs, and reduces cardiac workload; preserves endothelial function, reduces ET-1 levels, increases NO levels, and suppresses inflammatory responses; decreases the level of hs-CRP; improves lipids, including lower TG, TC, and LDL-C levels and higher HDL-C levels; inhibits ventricular remodeling and decreases TGF, a marker of myocardial fibrosis-β1. CTGF, PICP, CITP and PIIINP levels.
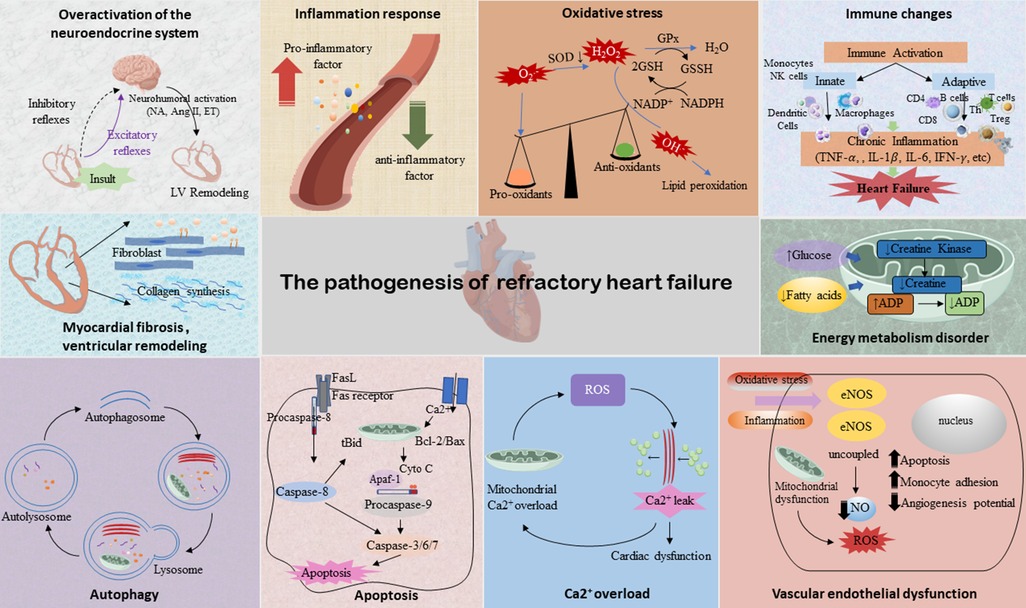
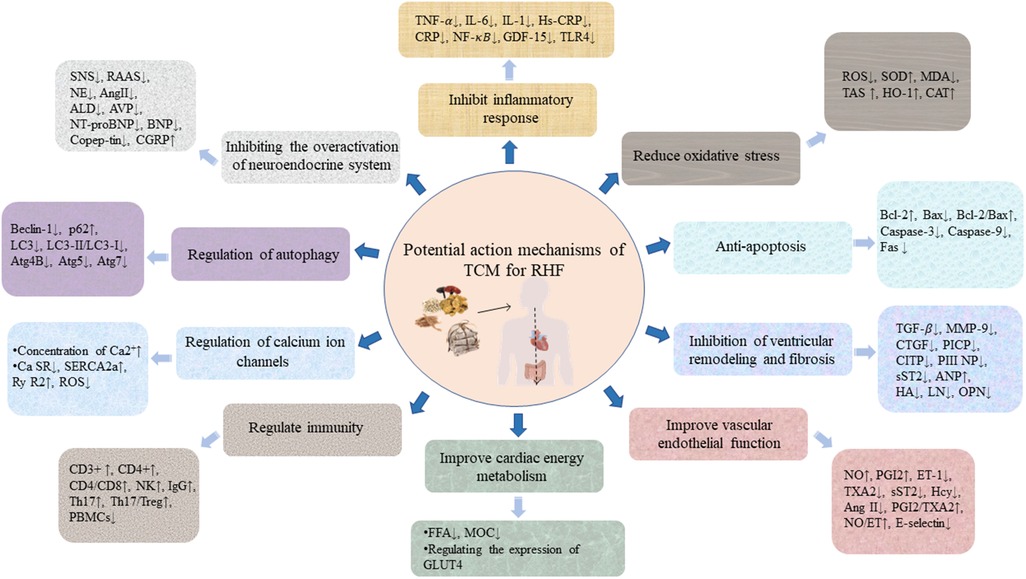
3 The mechanism of TCM in treating refractory heart failureThe pathogenesis of RHF has not been fully elucidated. Current research shows that neuroendocrine mechanisms, mainly including enhanced excitability of the sympathetic nervous system (SNS), activation of RAAS, and ventricular remodeling play important roles in the progress of RHF. In addition, cardiomyocyte energy supply and utilization disorders, inflammatory mediators, oxidative stress, vascular endothelial cell dysfunction, intracellular Ca2+ overload, and cardiomyocyte apoptosis are also involved in the pathophysiology of RHF (Figure 2), which are the key factors that make it deteriorate and cascade (77). The potential action mechanisms of TCM for RHF are shown in Figure 3.
Figure 2. The pathogenesis of RHF. Illustrations by Figdraw.
Figure 3. The potential action mechanisms of TCM for RHF. Illustrations by Figdraw.
3.1 Suppression of neuroendocrine system hyperactivationDuring the pathogenesis of HF, the activation of the neuroendocrine system leads to myocardial remodeling, which is a key factor in the occurrence and development of HF. In the early stage of HF, the SNS and RAAS are activated, playing a certain compensatory role. With the excessive activation of the neuroendocrine system, negative systemic effects will be generated on various organs, causing hemodynamic stress, circulatory disorder, and ventricular remodeling, thereby accelerating the progress of HF (78, 79). At the same time, with the aggravation of HF and the long-term activation of the neuroendocrine system, the myocardial afterload and oxygen consumption will be increased, promoting myocardial hypertrophy and then further worsening of HF, and producing a series of adverse cardiovascular events in the subsequent development of the diseases (80, 81).
By inhibiting the activity of the RAAS, aconite downregulates the level of nerve-cytokines, significantly improves the neuroendocrine disorder in HF rats caused by abdominal aortic coarctation, relieves ventricular remodeling, and improves the symptoms of HF (82). Dong et al. (83), through an experimental study of the chronic heart failure (CHF) rat model established by narrowing the abdominal aorta, confirm that Zhenwu decoction can inhibit SNS by reducing the plasma norepinephrine (NE) level of rats in the administered group, and then effectively improve the cardiac function of rats with HF. Liu et al. (84) also confirm that Zhenwu decoction can significantly reduce the levels of serum Ang II and ALD in rats with HF, and fight cardiac failure by antagonizing the excessive activation of RAAS. Xinmailong injection can correct hemodynamic disorder in various ways, and has the effects of strengthening the heart, diuresis, pulmonary vascular dilation, reducing pulmonary artery pressure, improving microcirculation and ventricular remodeling, regulating humoral factors and neuroendocrine, and scavenging oxygen free radicals, etc., to correct the neuroendocrine imbalance and antagonize a ventricular remodeling effect (85). The Qiliqiangxin capsule can reduce the levels of serum NE and ALD, and inhibit the activation of SNS and RAAS, thus delaying ventricular remodeling and disease progression in patients with CHF (85).
3.2 Inhibition of inflammatory responseNormal cardiac function is maintained by a balanced homeostasis of pro-inflammatory and anti-inflammatory cytokines. Dysregulation of the inflammatory response induces cardiomyocyte hypertrophy, apoptosis, fibrosis, and changes in cardiac hemodynamics (86), ultimately accelerating the progression of HF. Several studies have proved that the increase of pro-inflammatory biomarkers in patients with HF is associated with disease severity (87), and reducing the expression of these inflammatory factors can effectively improve HF (86, 88–90). Therefore, inhibiting the release of inflammatory factors is of great significance for delaying ventricular remodeling and improving cardiac function.
Inflammatory cytokines related to RHF mainly include TNF-α, interleukin, nuclear factor κB (NF-κB), and other inflammatory cytokines, which play an important role in cardiac dysfunction and adverse cardiac remodeling. Besides inflammation, inflammatory mediators can also activate endothelial cytokines (91), form a driving network with the RAAS system, and jointly participate in the development of HF. The activation of NF-κB increases the production of inflammatory cytokines and chemokines. Zhang et al. (92) found that astragaloside can reduce the levels of inflammatory factors, such as IL-6, IL-1, and TNF-α, by regulating the TLR4/NF-κB/PPAR α signaling pathway, thus improving cardiac function and cardiomyocyte viability, and alleviating myocardial injury in HF with midrange EF (HFmrEF) mouse model induced by LPS. Experimental studies (93) have shown that the compatibility of aconite and licorice can relieve inflammation and ventricular remodeling in mice through the TLR4/NF-κB pathway. Qichenyiqi dropping pills (94) can reduce the expression of inflammatory cytokines TNF-α and IL-6, thereby inhibiting the function of inflammatory factor pathways TNF-α, NF-κB, and IL-6-STAT3, improving the hemodynamic of the HF model, downregulating the level of inflammatory cell pathways NF-κB and PNFKB1, and alleviating ventricular remodeling (95).
3.3 Reduction of oxidative stressOxidative stress refers to the process in which highly reactive molecules such as reactive oxygen species (ROS) and reactive nitrogen species (RNS) accumulate excessively and then exceed the oxide scavenging capacity, resulting in the imbalance between pro-oxidation and the antioxidant system in the body (96). It is an important inducing factor of myocardial injury. HF can lead to the excessive accumulation of ROS and lipid peroxide, which aggravates cell membrane damage and leads to myocardial contraction and diastolic function deterioration (97). In addition, ROS cannot activate a variety of signaling kinases and transcription factors to mediate apoptosis but can stimulate the proliferation of cardiac fibroblasts, and activate matrix metalloproteinase, causing an increase of the extracellular matrix to induce myocardial remodeling, which is an important pathogenesis of HF.
Many studies have proved that TCM can reduce myocardial damage through antioxidation. Chen et al. (98) established a CHF model of cardiac hypertrophy induced by AAS and found that Qishenyiqi dropping pills (QSYQ) can significantly inhibit the progression of cardiac hypertrophy to HF induced by AAS in rats; its mechanism is related to the improvement of energy metabolism, oxidative stress, apoptosis, and other pathways. Lingguizhugan decoction can affect the SIRT1-AMPK-PGC-1α pathway, restore mitochondrial membrane potential, reduce ROS and malondialdehyde (MDA) levels, alleviate mitochondria and oxidative stress damage, promote mitochondrial biogenesis, increase the ejection fraction, and improve cardiac function in rats with HF (99). At the same time, it also antagonizes oxidative stress damage through the Nrf2/Keap1/HO-1 pathway (100). In addition, after different doses of Qiliqiangxin capsule intervention in rat models of chronic heart failure, the LDH and ROS levels in the serum of rats with HF are decreased, the activity of superoxide dismutase (SOD) is enhanced, the expression of the pro-apoptotic protein is inhibited, and the expression of B-cell lymphoma-2 (Bcl-2), p-Akt/Akt and p-GSK3β/GSK3β is upregulated. The cell experiments also demonstrate that, after hydrogen peroxide (H2O2) damage to cardiomyocyte (H9C2), cell proliferation is significantly improved, SOD activity, heme oxygenase-1 (HO-1), and catalase (CAT) mRNA expressions are significantly upregulated, while LDH, ROS, and apoptosis are significantly inhibited after 24 h under the intervention of Qiliqiangxin ultrafine powder. At the same time, it also inhibits mitochondria division, the opening of the mitochondrial membrane permeability transition pore (mPTP) and the decline of MMP, and alleviates the mitochondria-dependent apoptosis of cardiomyocytes damaged by oxidative stress (101). Ginsenoside Rb 1 can improve the hypoxia tolerance of cardiomyocytes by mediating the AMPK signaling pathway, reducing the levels of Atg4B, Atg5, Beclin1, Atg 7, LC3BII, and LC3BII/I ratio, and inhibit excessive autophagy to protect cardiomyocytes from hypoxic injury (102).
3.4 Inhibition of cardiomyocyte apoptosis and pyroptosisApoptosis can promote the progression of various cardiovascular diseases and is one of the important pathological mechanisms of myocardial tissue injury. In the failing heart, the decrease in the number of ventricular cardiomyocytes and the apoptosis of cardiomyocytes caused by interstitial fibrosis not only participate in ventricular remodeling, but is also one of the important reasons closely related to the severity of HF (103). Pyroptosis is a type of programmed cell death accompanied by inflammation, whose features are the formation of membrane pores on the cytoplasmic membrane, release of pro-inflammatory factors and cell contents, and swelling and rapid rupture of cells (104). Recent studies have suggested that pyroptosis is closely related to CHF; therefore, targeting pyroptosis has a good prospect in alleviating CHF (105). Therefore, inhibiting cardiomyocyte apoptosis and pyroptosis, intervening with the cause of apoptosis, and blocking the pathway of inducing cardiomyocyte apoptosis are of great significance in preventing the occurrence of HF and the deterioration of cardiac function (106).
Basic research has shown that Shenfu Qiangxin pills can significantly reduce myocardial hypertrophy in rats with chronic binding stress, inhibit ventricular septal thickness, and left ventricular posterior wall hypertrophy, reduce the expression of mRNA of damaged tissue pattern receptors, inhibit the expression of extracellular regulatory protein kinases 1/2 and p38 protein of mitogen-activated protein kinase signaling pathway, upregulate Bcl-2 expression, inhibit associated X protein (Bax) expression, and reduce the rate of cardiomyocyte apoptosis, exerting a protective role on the heart (107, 108). By downregulating the expression of the pro-apoptotic protein Bax, upregulating the anti-apoptotic protein Bcl-2 expression and the Bcl-2/Bax ratio, Yiqi Huoxue formula can improve the cardiac function of rats with myocardial infarction, thereby alleviating the myocardial apoptotic injury and protecting the heart (109). The Qiliqiangxin capsule activates the PI3K/AKT/Gsk3β signaling pathway by decreasing ROS and downregulating the expression of apoptosis-related proteins Fas and caspase-3, and inhibits the apoptosis of cardiomyocytes of rats with chronic heart failure (101). Shengmai injection can alleviate endoplasmic reticulum stress, upregulate Bcl-2/Bax ratio, downregulate caspase-3 expression, inhibit caspase-dependent apoptosis, and then protect the myocardial damage caused by doxorubicin (110, 111). Fan et al. (112) report that Shenfu injection can improve CHF by regulating pyroptosis based on the NLRP3/caspase-1 pathway. There are also studies that Shenkui Tongmai Granule can improve the cardiac function of the CHF rat model and reduce the pyroptosis of cardiomyocytes (113). Studies have shown that excessive or continuous endoplasmic reticulum stress promotes the occurrence and development of chronic heart failure by inducing cardiomyocyte apoptosis (114). Luo et al. (115) report Yiqi Huoxue Recipe improves heart function through inhibiting apoptosis related to endoplasmic reticulum stress in a myocardial infarction model of rats.
3.5 Inhibition of ventricular remodeling and fibrosisThe alteration of ventricular structure and myocardial fibrosis are the key factors causing the further progression of RHF. It has been found that the deposition of a large amount of extracellular matrix and collagen changes the ventricular structure along with the increase of the chamber volume, damages the myocardial structure, causes cardiac diastolic and systolic dysfunction, reduces cardiac function, and promotes the development of HF (116). Therefore, in addition to the improvement of existing clinical symptoms, patients with RHF should focus on delaying the process of ventricular remodeling and myocardial fibrosis.
A number of basic and clinical studies have shown that TCM can effectively delay cardiac remodeling and improve myocardial fibrosis. Zhen et al. (117) discovered that the Qiliqiangxin capsule can effectively improve the clinical symptoms of patients with HF, reduce the serum levels of MMP-2, MMP-9, and MMP-13, increase the levels of tissue inhibitor of matrix metalloproteinases (TIMP)-1 and TIMP-2, regulate the expression of MMPs and TIMPs in patients with HF, and improve the metabolic disorders of the extracellular matrix, thereby inhibiting myocardial fibrosis and ventricular remodeling and improving cardiac function. Another study has reported that astragaloside can improve myocardial ultrastructural damage, reduce myocardial collagen deposition in rats with HF (118), improve myocardial fibrosis, improve cardiac function, and inhibit the development of CHF (119). Li et al. (120) used Ang II to induce the CHF model when studying the intervention effect of Shengmai injection on animals with chronic heart failure and discovered that Shengmai injection can reduce cardiomyocyte hypertrophy and apoptosis, protect mitochondrial function in hypertrophic cardiomyocytes, and inhibit cardiac fibrosis. Wei et al. (121) applied the Isoproterenol(ISO)-induced myocardial injury model to study the effect mechanism of compound Danshen dropping pills and found that it can significantly improve the survival rate of ISO-treated rats and alleviate myocardial fibrosis, whose mechanism is associated with improving the metabolism of myocardial tissue. The Qiliqiangxin capsule alleviates cardiac remodeling by inhibiting the TGF-β1/Smad3 and NF-κB signaling pathways (122). Shenfuyixin granules can downregulate the expression of c-fos and c-myc and delay myocardial remodeling in HF rats (123).
3.6 Improvement of vascular endothelial functionEndothelial dysfunction is the pathophysiological basis of HF (124). Cardiac endothelial cells not only participate in the formation and metabolism of blood vessels but also regulate myocardial fibrosis, cardiac hypertrophy, and cardiomyocyte apoptosis and autophagy. When HF occurs, endothelial cell dysfunction not only causes a decrease in NO and an increase in ET, leading to increased vascular resistance, but also the damaged endothelial cells will produce a large number of growth factors and active substances and promote the proliferation of smooth muscle cells and the production of the matrix (125), resulting in systemic peripheral resistance to decrease vascular compliance, vascular stiffness, and arterial dilation damage, aggravate vascular remodeling, cause heart inflammation and myocardial fibrosis, and promote the occurrence and development of HF (126).
TCM can reduce arterial wall stiffness and vascular resistance, and slow down ventricular remodeling by protecting vascular endothelial function. Studies have found that the Shensongyangxin capsule can not only reduce the damage of oxidative stress and immune inflammation on vascular endothelial function by inhibiting the formation of oxygen free radicals and the body's inflammation, but also inhibit the secretion of angiotensin and catecholamine, promote the release of vasodilator factor, regulate the body's vasomotor balance, and protect vascular endothelial function (127). Zhang and Huang (128) studied the effect of the Qiliqiangxin capsule on myocardial injury and vascular endothelial function in patients after percutaneous coronary intervention, and found that the Qiliqiangxin capsule may protect the microvascular endothelial function, reduce myocardial injury, and improve cardiac function by increasing plasma NO and reducing ET-1. In addition, in animal experiments, the Qiliqiangxin capsule can improve the serum concentrations of VEGF and HIF-1 in HF rats, and activate the angiogenesis pathway associated with HIF-1-VEGF, thereby promoting angiogenesis, alleviating myocardial ischemia and hypoxia injury, and delaying ventricular remodeling. The Guanxinkang capsule combined with ivabradine hydrochloride tablets can regulate the levels of serum Ang II, ACE II, and NT-pro BNP, reduce vascular endothelial cell damage in patients with RHC, and improve cardiac function (49). The Shenfu injection enhances eNOS activity through the PI3K/Akt signaling pathway, to promote vasodilation and improve the microcirculation in the failing heart (129).
3.7 Improvement of cardiac energy metabolismThe heart is the most active organ with high oxygen consumption and high energy consumption in the human body. The process by which cardiomyocytes can use a variety of energy substrates to store and utilize energy is called myocardial energy metabolism (130). Normal myocardial energy metabolism can maintain a stable environment in cardiomyocytes and keep a normal diastolic function. Studies have found that patients with HF will exhibit serious energy metabolism disorders, including substrate absorption and utilization disorders, mitochondrial structure and function abnormalities, and myocardial high-energy phosphate changes, resulting in insufficient heart energy supply, which will lead to heart pump dysfunction and systemic energy metabolism disorders, thus causing the change of heart structure and function and speeding up the development of HF (131). Numerous studies have shown that there is abnormal energy metabolism in HF, and the regulation of myocardial energy metabolism may be a new treatment for HF (132).
Experimental studies have proved that the Shenfuqiangxin mixture can upregulate the expression of phosphorylated AMPK (p-AMPK) and PGC-1α in rats with HF, reduce the levels of serum BNP, free fatty acid (FFA) and LDH in HF rats, regulate glucose transport and fatty acid oxidation metabolism, and accelerate myocardial energy metabolism (133). Shenfu formula, through activating AMPK-mediated fatty acid and glucose metabolism in the heart, regulates the gene expression of glucose transporter 4 (GLUT4) and promotes the myocardial uptake and utilization of cardiac glucose, thus improving the myocardial energy metabolism to alleviate heart failure (134). Shenmai injection maintains the mitochondrial structure and function, improves energy metabolism, and increases the survival rate of cardiomyocytes by maintaining mitochondrial membrane potential and inhibiting the opening of mitochondrial permeability transition pore (135). Han et al. (136) use the AAC model to study its mechanism and find that the potential mechanism of Yiqifumai in treating HF is realized by enhancing myocardial mitochondrial function and regulating myocardial energy metabolism.
3.8 Regulation of immunityStudies have found that many types of immune cells, such as NK cells, T cells, B cells, monocytes, macrophages, etc., are all involved in the process of cardiac fibrosis and myocardial remodeling (137). Therefore, the activation of immune cell-mediated immunity may play a crucial role in the pathogenesis of various forms of RHF. The treatment targeting immune regulation is considered beneficial in patients with HF with immune disorders that are a key factor in the aggravation of RHF (138).
A study found that the Shenfu injection can reduce the levels of plasma IL-10 and NT-pro BNP in patients with HF, and increase the proportion of TGF-β1, peripheral blood CD4+, and CD4+CD+25Foxp3+Treg cells, thereby exerting an immune regulatory role and then delaying the development of HF (139). The Qiliqiangxin capsule can significantly increase the levels of CD4+cell subsets, NK cells and IgG in patients with HF, improve ventricular remodeling and related immune indexes, and improve immunity and patients’ quality of life (140). The Lingguizhugan decoction can reduce the serum levels of IL-6, IL-18, and TNF-α in patients with HF, increase the levels of CD3+T, CD4+T, and CD4+T/CD8+T, and improve the cardiac function and clinical symptoms of patients by regulating immunity and inhibiting inflammatory response (141). The Qishanyiqi dropping pills can affect the dynamic balance of immune cell subsets and increase the levels of CD4 and CD4/CD8, thereby improving the immune function of patients with HF (142). The Shenqi compound can effectively regulate the disorder of CD4+T lymphocyte subsets in the peripheral blood of patients with HF, increase the levels of Th17, Th17/Treg and the serum IL-10, and reduce the expression of IL-2, IL-6, IL-17, TNF-α, and IFN-γ pro-inflammatory factors. At the same time, in animal experiments, the Shenqi compound can also reduce inflammatory damage, improve cardiac function in rats, and alleviate ventricular remodeling by inhibiting the IL-6/STAT3 signaling pathway and the differentiation of Th17 cells, and restoring the balance of the Th17/Treg cell (143).
3.9 Regulation of calcium ion channelsAs the “second messenger” of cells, calcium ions (Ca2+) play an important role in the pathogenesis of cardiovascular diseases, and the imbalance of Ca2+ homeostasis in cardiomyocytes is a key factor in the pathological changes of HF. We all know that the essence of HF is the contraction or diastole dysfunction of cardiomyocytes, and the contraction and diastole of the heart are mainly carried out through the exchange of Ca2+ inside and outside the cell. When calcium homeostasis occurs in patients with HF, the intracellular Ca2+ homeostatic order will cause contraction and diastolic dysfunction by interfering with RyR2, the sarcoplasmic Ca2+-ATP enzyme (SERCA) pathway, and the sodium/calcium exchange protein (NCX) (144, 145), resulting in the development of HF.
TCM can repair abnormal calcium homeostasis in failing cardiomyocytes by regulating the expression and activity of various calcium-treated proteins. For example, ginsenoside Rg1 can regulate the intracellular Ca2+ concentration, reduce the expression of Ca SR, and play a myocardial protective role through the Ca2+/Ca SR pathway (146). Astragaloside can inhibit Ca2+ accumulation induced by LPS, prevent LPS-induced cardiac hypertrophy by inhibiting the Ca2+/CaN/NFAT-3/GATA-4 signaling pathway, and increase myocardial contractility (147). Liggustrazine can not only scavenge oxygen free radicals, but also inhibit lipid peroxidation and inflammation, maintain the dynamic balance of Ca2+, inhibit cell death, and protect cardiomyocytes (148). Qishen granule treatment can effectively reduce the concentration of Ca2+ in the cardiomyocytes of rats with HF, and improve cardiac function, ventricular remodeling, and lipid metabolism (149). Wenyang Yiqi Huoxue decoction can improve cardiac dysfunction in rats with HF by enhancing the activity of the Na+-K+-ATP and Ca2+-ATP enzymes and upregulating their mRNA and protein expressions (150).
3.10 Regulation of autophagyAutophagy is a highly conserved dynamic change process in cell life that maintains cellular energy balance and organelle renewal (151), and is an important mechanism for maintaining the stability and function of the environment in cardiomyocytes, which can limit cardiac injury under many pathological conditions. However, increased autophagic flux in cardiomyocytes may cause autophagic cell death, leading to uncontrolled degradation of materials or an imbalance with lysosomal degradation, which is accompanied by excessive accumulation of autophagosomes, eventually leading to cell death (152). Several studies have found that autophagy in cardiomyocytes with high activation for a long period of time is one of the key factors leading to the progression of HF (153, 154). Therefore, regulating and stabilizing moderate autophagy in cardiomyocytes is important for the maintenance of normal cardiac function.
In animal experiments, Liao et al. (155) found that the Shenfu injection can activate the PI3K/Akt/mTOR signaling pathway, downregulate the content of autophagosome marker microtubule-related protein 1 light chain 3 (LC3) of myocardial tissue, increase the expression level of autophagy marker protein p62 to inhibit autophagy, and reduce myocardial fibrosis, thereby protecting the damaged cardiomyocytes and improving heart function. The PINK1/Parkin pathway is a typical mitochondrial autophagy pathway and an important regulator in the process of mitochondrial autophagy (156). Many studies have found that the activation of the PINK1/Parkin pathway can prevent mitochondrial damage and cardiomyocyte apoptosis by increasing the level of mitochondrial autophagy (157), improve cardiac contractile function (158), and reduce heart failure(159). There are studies (160, 161) reporting that Nuanxinkang can prevent the development of myocardial infarction-induced chronic heart failure by promoting PINK1/Parkin-mediated mitophagy and ginsenoside Rg1 can protect against cardiac remodeling in heart failure via SIRT1/PINK1/Parkin-mediated mitophagy.
In summary, the mechanism of TCM in treating RHF includes, but is not limited to, the following: (1) inhibiting the overactivation of the neuroendocrine system by targeting to reduce the levels of serum NE, AngII, ALD, etc.; (2) regulating the immune and inflammatory responses by targeting inflammatory cytokines, such as TNF-α, IL-6, IL-1β, IL-2β, NF-κB, CD3+ T, CD4+ T, etc.; (3) enhancing myocardial mitochondrial function, maintaining a Ca2+ dynamic balance, improving the myocardial energy metabolism and inhibiting myocardial damage by balancing myocardial energy metabolism, including reducing the content of lactic acid and free fatty acids, promoting the transport and utilization of fatty acids, and mediating the metabolism of fatty acids and glucose in the heart; (4) improving extracellular matrix metabolism disorders, and inhibiting myocardial fibrosis and ventricular remodeling by targeting the expression of MMPs and TIMPs, and upregulating the expression of LCAD, LVMI, CVF, LVPWD, PFK1 protein, and mRNA; (5) alleviating myocardial damage caused by hypoxia-induced apoptosis and oxidative stress through targeted regulation of LDH, ROS, SOD, HO-1, CAT, Fas, and caspase-3 expression, as well as the Bcl-2/Bax ratio; (6) activating the HIF-1-VEGF angiogenesis pathway and alleviating the endothelial cell dysfunction by targeting NO, PGI2, and ET-1; and (7) regulating mitochondria and cell autophagy activity to play a role in myocardial protection by targeting key autophagy proteins such as Atg4B, Atg5, Atg7, Beclin1, mTOR, LC3-II, LC3-I, and p62.
4 Conclusion and perspectivesRHF is a serious clinical problem that imposes a significant economic burden on a patient's family and society. Due to the increasing aging population, the prevalence of RHF has climbed annually and the difficulty finding treatment has also increased, which has gradually led to a long treatment cycle, persistent symptoms and signs, a poor prognosis, and other clinical characteristics. Currently, there are no large randomized clinical trials with RHF as the research subject and cardiovascular events as the observation endpoint; therefore, the treatment modalities that can reduce the cardiovascular event rate of RHF are unclear, and modern medicine still lacks effective methods of treating RHF. As a result, how to take effective measures to improve the survival rate of patients with RHF is a current medical dilemma that urgently needs to be addressed.
Guideline-directed medical therapy (GDMT) is the fundamental treatment for RHF. In recent years, clinical trials for sacubitril valsartan, ivabradine, levosimendan, and sodium glucose cotransporter 2 inhibitors have been released, which can benefit patients in reducing the risk of death and readmission rates (162–165). The standardized application of GDMT has improved the overall prevention and control of RHF. After the appropriate application of various treatment measures based on GDMT, if the patient's heart function is still severely damaged and there are no other effective treatment methods, heart transplantation is the most effective treatment. However, the shortage of heart donors and the ischemic time of donors restrict the possibility of heart transplantation (166). In addition, complications, such as thrombosis, bleeding, infection, and those caused by mechanical devices used in heart transplantation, are still difficult to avoid, and it is still necessary to continue to explore the fully built-in device and appropriate anti-thrombotic scheme in the future. In China's long-term medical practice, traditional Chinese medicine has been widely used in the treatment of heart failure due to its unique efficacy and safety advantages, accumulating rich experience. The combination of traditional Chinese and Western medicine in the treatment of heart failure is currently a research hotspot. With the emergence of research results, the efficacy of traditional Chinese medicine in treating heart failure has gradually been confirmed. Reports have shown that the combined treatment of syndrome differentiation based on a Chinese herbal decoction, CPMs, and Chinese medicine injection, which is based on the conventional treatment of Western medicine, can effectively alleviate the clinical symptoms, improve the quality of life and exercise tolerance, improve the long-term prognosis, and reduce the rate of rehospitalization and mortality in patients with RHF.
TCM has provided new ideas and directions for the treatment of RHF; however, several problems have also been identified. First, it is difficult to apply TCM widely clinically: TCM shows certain clinical advantages through syndrome differentiation and individualized treatment of RHF, and because of the flexibility of syndrome differentiation, there is no uniform protocol for syndrome differentiation and treatment, making it difficult to apply TCM widely in the clinic. Second, there are few high-quality clinical studies: on the one hand, the clinical sample size is small, the observation period is short, and large-scale, multicenter, prospective randomized controlled studies are lacking; on the other hand, the clinical protocol design was not rigorous, and some of the included clinical studies had unclear descriptions of sample size estimation, random allocation concealment scheme, blinded design, and dropout rate, resulting in generally low-quality articles. Third, clinical efficacy is unclear: although clinical studies have focused on RHF, the results of large sample, multicenter, prospective RCTs focusing on RHF with cardiovascular events as the outcome measure are still lacking, and the treatment of RHF is still limited to improving clinical symptoms. Therefore, it is unclear which treatment modality can reduce the cardiovascular event rate of RHF. Finally, there is an unclear mechanism of action: TCM has a complex composition, and its mechanism of action in treating RHF is unclear. In addition, animal models of RHF that meet the clinical characteristics are currently lacking. In response to the above scientific questions, we suggest future research should focus on the following directions: (1) strengthening the scientific and normative of clinical research, carrying out multicenter and large sample high-quality RCTs with cardiovascular events as the observed endpoints, establishing treatments with evidence-based medical evidence, and provide more reliable clinical evidence for the Chinese medicine treatment of RHF; (2) establishing an animal model of RHF that conforms to clinical characteristics; (3) combining the use of network pharmacology, bioinformatics, transcriptomics, proteomics, metabolomics, UPLC-Q/Orbitrap/MS, and other techniques to deeply mine the deep action mechanisms of TCM for the treatment of RHF to provide a scientific basis for its clinical application.
In conclusion, RHF remains an urgent clinical problem. TCM has great potential for treating RHF, but further systematic and in-depth clinical and basic experimental studies are still needed.
Author contributionsLG: Writing – original draft. ZY: Writing – review & editing. WF: Writing – review & editing. YL: Writing – review & editing. ZL: Writing – original draft. PZ: Methodology, Supervision, Writing – review & editing. MR: Funding acquisition, Writing – review & editing.
FundingThe authors declare financial support was received for the research, authorship, and/or publication of this article.
This study is subsidized by the National Key Research and Development Plan (2018YFC1707403) and the Innovation Team Development Plan of the Ministry of Education (IRT_16R54).
AcknowledgmentsThe authors acknowledge Figdraw (www.figdraw.com) for designing the images for Figures 2 and 3.
Conflict of interestThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's noteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary materialThe Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2024.1369642/full#supplementary-material
AbbreviationsRHF, refractory heart failure; TCM, traditional Chinese medicine; NYHA, classification of heart function by the New York Heart Association; MLHFQ, Minnesota Living with Heart Failure Questionnaire; TGF-β1, transforming growth factor-β1; PGC-1α, peroxisome proliferator-activated receptor gamma coactivator 1-alpha; 6MWD, 6-min walking distance; BNP, brain natriuretic peptide; LA, lactic acid; LVEDD, left ventricular end diastolic diameter; LVESD, left ventricular end systolic diameter; LVEF, left ventricular ejection fraction; LVFS, left ventricular fraction shortening; LVIDd, left ventricular internal diastolic diameter; LVIDs, left ventricular internal dimension systole; NT-proBNP, N-terminal pro-B-type natriuretic peptide; SPAP, pulmonary artery systolic pressure; PaO2, partial pressure of oxygen in artery; SaO2, arterial blood saturation; FEV1, forced expiratory volume in 1 s; CRP, C-reactive protein; TNF-α, tumor necrosis factor-α; IL-6, interleukin-6; ALD, aldosterone; SOD, superoxide dismutase; ROS, reactive oxygen species; MDA, malondialdehyde; TAS, total antioxidant; LDH, lactate dehydrogenase; E/A, early diastolic peak mitral orifice velocity/late diastolic peak mitral orifice velocity; ET-1, endothelin-1; cTnI, cardiac troponin I; H-FABP, heart-fatty acid binding protein; CK-MB, creatine kinase myocardial bound; ICTP, procollagen type I carboxy terminal peptide; PIIINP, type III procollagen amino terminal peptide; CTGF, connective tissue growth factor; HA, hyaluronic acid; LN, laminin; CI, cardiac index; SV, stroke volume; CO, cardiac output; LVESV, left ventricular end systolic volume; LVEDV, left ventricular end diastolic volume; LVRI, left ventricular remodeling index; Ang II, angiotensin II; LPS, lipopolysaccharide; TC, total cholesterol; LDL-C, low-density lipoprotein cholesterol; SBP, systolic blood pressure; DBP, diastolic blood pressure; RyR2, ryanodine2; NF-κB, nuclear factor kappa-B; Bax, associated X protein; Bcl-2, B-cell lymphoma-2; MMPs, matrix metalloproteinases; TIMPs, tissue inhibitor of matrix metalloproteinases; MMP-9, matrix metalloproteinase-9; TLR4, toll-like receptor4; GLUT4, gene expression of glucose transporter 4; LC3, microtubule-related protein 1 light chain 3; LC3-I, microtubule-associated protein 1 light chain 3-I; LC3-II, microtubule-associated protein 1 light chain 3-II; TG, triglyceride; HDL-C, high density lipoprotein; hs-CRP, hypersensitive C-reactive protein; ES, E-selection; AST, aspartate aminotransferase; ALT, alanine aminotransferase; HBDH, Hydroxybutyrate dehydrogenase; PICP, Recombinant Procollagen I C-Terminal Propeptide; CITP, type I pro-hydroxy terminal cross linked peptide, eGFR, estimated glomerular filtration rate; SCr, serum creatinine, QSYQ, Qishenyiqi dropping pills; HFmrEF, HF with midrange EF; ISO, Isoproterenol.
References1. Cappannoli L, Scacciavillani R, Rocco E, Perna F, Narducci ML, Vaccarella M, et al. Cardiac contractility modulation for patient with refractory heart failure: an updated evidence-based review. Heart Fail Rev. (2021) 26(2):227–35. doi: 10.1007/s10741-020-10030-4
PubMed Abstract | Crossref Full Text | Google Scholar
2. Fang JC, Ewald GA, Allen LA, Butler J, Westlake Canary CA, Colvin-Adams M, et al. Advanced (stage D) heart failure: a statement from the Heart Failure Society of America Guidelines Committee. J Card Fail. (2015) 21(6):519–34. doi: 10.1016/j.cardfail.2015.04.013
PubMed Abstract | Crossref Full Text | Google Scholar
3. GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the global burden of disease study 2017. Lancet. (2018) 392(10159):1789–858. doi: 10.1016/S0140-6736(18)32279-7
留言 (0)