This is the first study to correlate stone characteristics with two different treatment outcomes. The absence of standardized criteria defining a successful ESWL treatment might account for the varying data observed in prior studies. Our findings notably diverge when comparing the two treatment outcome categories. The only significant variable in our study that could predict stone disintegration was stone location. Nakasato et al., in a retrospective study of 260 patients with renal and ureteral stones, also encountered this correlation, with a better outcome in stones located in the ureter than renal stones [10]. Nevertheless, this latest study defined treatment success as an SFR of < 4 mm at twelve weeks, not solely stone fragmentation. Most published research does not emphasize stone location as a major predictor of stone disintegration; it appears to be more relevant when related to the stone clearance rate. Stones located in the lower renal pole, when treated, tend to leave fragments that remain in the calyx and cause recurrent stone formation. The reported SFR for lower pole calculi is 25–95% [29], compared to the SFR of 32% in our study.
The second outcome defined in our work, the retreatment rate, is probably even more relevant for treatment selection. Stone fragmentation is an important factor when evaluating the effectiveness of ESWL but does not translate to its overall success. This is because even in cases where fragmentation is successful, additional interventions may be necessary if residual fragments exceed 4 mm and the patient continues to experience symptoms. Upon analyzing our findings, 30% (77 cases) of the cohort with successful fragmentation still needed further intervention. The definition of retreatment is, however, different between studies. The overall success of ESWL in our study increases from 63 to 83.5%, if we set the retreatment outcome including or excluding another session of ESWL, respectively. There is a trend towards a higher success rate in studies that consider treatment to be successful when they include one to three ESWL sessions (Table 1).
Our findings indicate that the maximum stone size measured on KUB can predict the need or retreatment, aligning with the majority of literature. It’s worth noting that we measured size on KUB rather than NCCT, which may lead to discrepancies in results due to its lower sensitivity. However, other studies have also measured stone size in KUB and had similar results. One such example is the study by Ng et al. in which 2489 patients were assessed using ultrasound and KUB alone. A statistically significant correlation (p < 0.001) was also found between size and treatment success (stone-free status after one session at three months of follow-up) [13]. The study by Perks et al. measured stone size with KUB and NCCT, with similar results in terms of correlation to stone fragmentation [20].
NCCT is a widely accepted imaging method to characterize stone disease; the information obtained through this method, namely stone density, size, and SSD, has been widely studied and related to ESWL efficacy. The preliminary studies of Joseph et al. [17] and Pareek et al. [4] first described a significant correlation between stone disintegration and MAV. After these, a relevant part of the discussion in the literature was related to the standardization of MAV measurement [6]. We adopted the same method as Müllhaupt et al., defining regions of interest just smaller than the stone in magnified images [16]. Different measuring methods can justify distinct results in the literature. As in the study by Müllhaupt et al., our study did not show any correlation between MAV and stone disintegration. However, when the defined treatment outcome was the need for retreatment, a significant correlation was found, with a cut-off value of 827 HU. This result is similar to the one described by Wiesenthal et al., in which the treatment outcome was also defined as a single-treatment success, with a cut-off value of 900 MAV [7].
The measuring method of SSD did not vary among studies [19]. In our results, SSD could not predict treatment outcomes in both its definitions. Although the majority of literature supports the predictive value of SSD in treatment success, some studies align with our findings. Yl et al. conducted a retrospective study of 115 patients with renal stones who underwent more than one ESWL session. They found no correlation between SSD and an SFR of < 3 mm at one-month follow-up (p = 0.501) [22]. Another example is the study by Kang et al., also with a retrospective nature, that evaluated 399 patients with ureteral stones who underwent a single ESWL session [25].
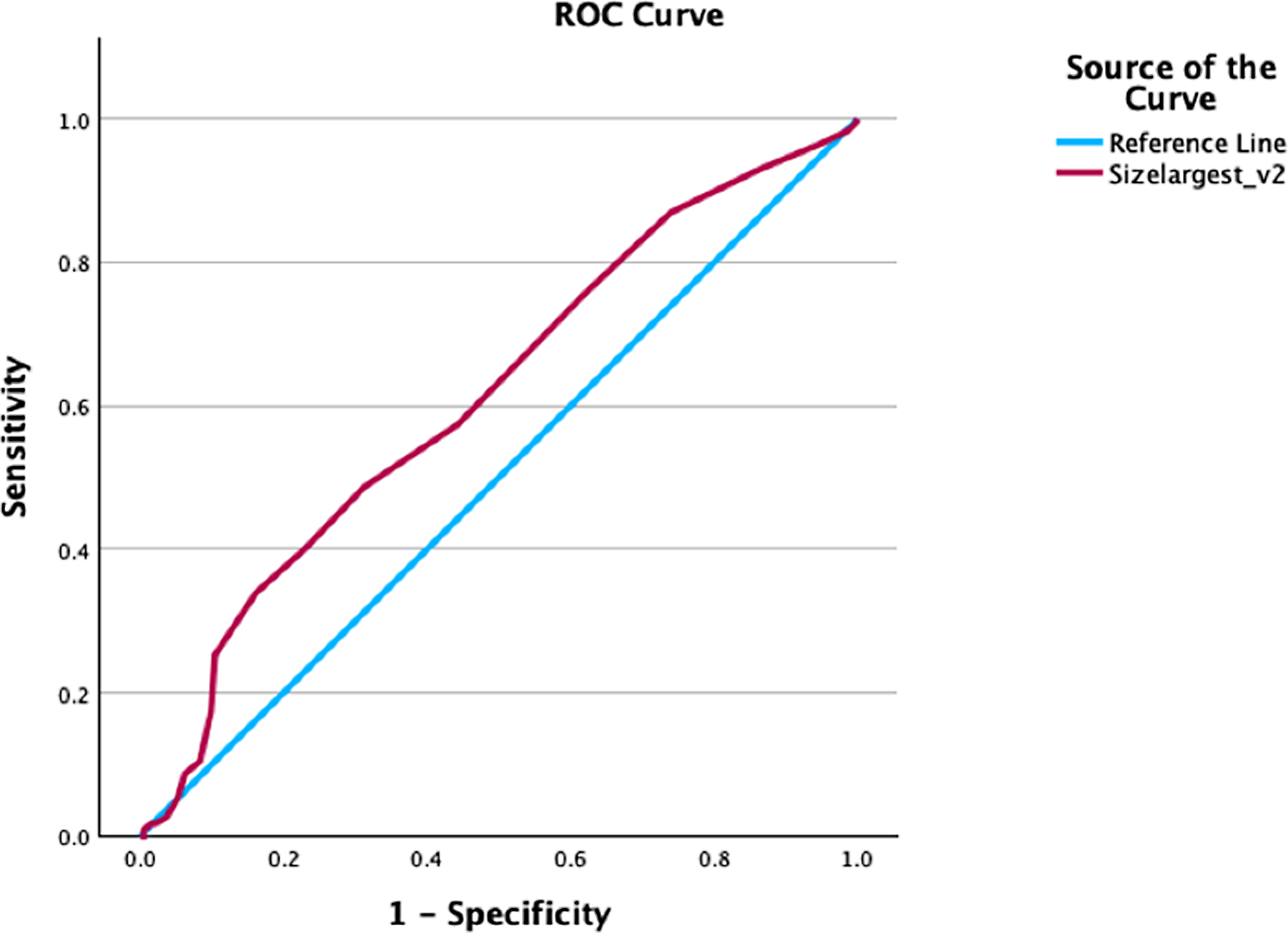
An important consideration is whether NCCT is strictly necessary for treatment decision. It is generally accepted that NCCT allows for a superior assessment of stone disease. However, good patient selection also seems to be possible using KUB alone, namely assessing stone size. In our study, the sensitivity and specificity of MAV as a predictor of treatment success is higher compared to stone size alone; the AUC of the ROC curve is 0.729, compared to the AUC of stone size, 0.613. However, the difference between groups in both treatment outcomes did not reach statistical significance. Also, the predicting value of stone size demonstrated in our study seems to be lower compared to the results of other studies. In the prospective study by Wang et al. that included 80 patients with renal stones, both stone size and stone density were significant predictors of treatment outcome (SFR ≤ 4 mm in NCCT at three months). The AUC for stone size was higher than stone density (0.855 and 0.768, respectively) [18]. Another example is the retrospective study by Park et al., which included 115 patients with renal stones. Here, the AUC between stone density and size did not differ significantly (stone density: 0.874; stone size: 0.827, p = 0.388) [22]. On the other hand, in the prospective study from Yoshida et al., which included 62 patients with renal and proximal ureteral stones, MAV had a better negative predictive value than maximal diameter (78.6% compared to 66.7%), being treatment failure residual fragments bigger than 3 mm after three ESWL sessions [6]. Tanaka et al. analyzed 75 patients retrospectively and described MAV as the only independent predictor of ESWL success (AUC of 0.692) [9]. These conflicting results leave room for discussion about whether it is mandatory to assess patients with NCCT for treatment selection.
Our study is not without limitations. Its retrospective nature implies a lack of standardization in assessing patients before treatment, particularly in terms of imaging. This comparison was, nevertheless, one of the aims of this study. NCCT images were acquired using different devices, with collimation adapted to each patient, differing from some prospective studies. Patients were assessed by different physicians using KUB images, usually less sensitive for detecting residual fragments. However, this reflects the usual practice among urologists; we believe that studies should be tailored to the reality of clinical practice.




留言 (0)