

記住我



Percutaneous coronary intervention (PCI) is widely recognized in clinical practice to improve the symptoms and outcomes of patients with coronary artery disease (CAD) (1, 2). Despite the established benefits of PCI, certain patients who undergo successful PCI still experience adverse cardiovascular events (3). Conventional coronary angiography can provide information only on the contour of the culprit vessel and may not account for physiological dysfunction, which explains the unanticipated adverse events in patients undergoing successful revascularization (4).
Physiological assessments are of increasing importance because of their ability to provide functional information about target vessels and to optimize treatment strategies (5, 6). Fractional flow reserve (FFR) is a widely accepted physiological assessment technique and is considered the gold standard in revascularization procedures (7, 8). Although the FFR provides significant functional information, it is still underutilized in clinical practice due to the prolonged procedure time and invasive use of guidewires (9, 10). The quantitative flow ratio (QFR) has emerged as an alternative approach for deriving physiological parameters, with the advantages of having equivalent diagnostic value and being faster and more convenient than the FFR (11, 12).
The residual QFR is an essential indicator derived from the QFR computation procedure and can simulate the anticipated QFR value after successful revascularization based on pre-PCI angiographic images (13). Previous studies have reported that the residual QFR significantly correlates with the post-PCI FFR, especially in patients with suboptimal PCI results (14). Based on the residual QFR, a cardiologist can identify the major lesion from a functional perspective, further optimizing the PCI strategy. The residual QFR-guided PCI strategy was superior to angiographic guidance in reducing the 2-year incidence of target vessel failure (TVF) (15, 16). However, research into the predictive value of the residual QFR for adverse events is limited, particularly in patients whose residual QFR does not match their post-PCI QFR. Therefore, the present study aimed to further investigate the prognostic value of the residual QFR by exploring the correlation between the ΔQFR (defined as the value of the post-PCI QFR minus the residual QFR) and clinical outcomes.
Materials and methods Study designThe present research was a single-center, retrospective, observational study. Consecutive patients who underwent PCI were recruited from January 1, 2016, to December 31, 2017, at Fujian Medical University Union Hospital. The QFR of the enrolled patients were retrospectively assessed at the different time points of the PCI procedure, and the patients were further divided into five groups according to the ΔQFR: (1) Overanticipated group: ΔQFR ≥ 0.1; (2) Slightly overanticipated group: 0 < ΔQFR < 0.1; (3) Consistent group: ΔQFR = 0; (4) Slightly underanticipated group: −0.1 < ΔQFR < 0; and (5) Underanticipated group: ΔQFR ≤ −0.1. The primary purpose of this study was to test the prognostic value of the consistency between the residual QFR and post-PCI for cardiovascular adverse events. This study was approved by the Ethics Committee of Fujian Medical University Union Hospital (No. 2020KY098).
The study population consisted of adult patients who underwent successful PCI, including patients with stable or unstable angina pectoris, non-ST elevation myocardial infarction (NSTEMI), or ST elevation myocardial infarction (STEMI), over 7 days. All enrolled patients met the requirements for QFR computation, which suggests that in all patients, at least one lesion with a percent diameter stenosis (DS%) between 50% and 90% is present in a coronary artery with a reference vessel diameter of ≥2.5 mm according to visual assessment. Patients were excluded if they had any of the following criteria: (1) acute myocardial infarction (AMI) within 7 days, (2) lack of follow-up data, or (3) inability to perform QFR computation, including patients who only had one coronary artery lesion with >90% stenosis and a TIMI grade <3; the interrogated lesion involving the myocardial bridge; severe overlap in the stenosed segment or severe tortuosity of any interrogated vessel; or poor angiographic image quality.
PCI procedure and QFR computationPCI was performed, and the stenting strategy was determined by an experienced cardiologist according to the ESC/EACTS guidelines at the time of enrollment (17). All patients received standard dual antiplatelet therapy for at least 12 months after successful revascularization. Rational medication was prescribed according to the clinical situation.
The QFR was computed using the AngioPlus system (Pulse Medical Imaging Technology Shanghai, China) according to standard operating procedures, which were performed by two independent investigators blinded to the clinical data. All coronary angiography images were transferred locally to the AngioPlus system. Angiographic images were recorded with an AngioPlus system at a rate of 15 frames/second. Two angiographic image runs, acquired at angles greater than or equal to 25 degrees, were transferred to the QFR system via the local network. Based on the reconstruction of the contoured vessels, the QFR value was computed using a contrast flow velocity model. The QCA information derived from the QFR analysis of the interrogated vessels consisted of the minimum lumen diameter (MLD), diameter stenosis percentage (DS%) and area stenosis percentage (AS%).
Data collection and clinical outcomesThe biochemical indices and examination results, including low-density lipoprotein cholesterol (LDL-C), fasting blood glucose, creatinine, N-terminal pro brain natriuretic peptide (NT-proBNP), troponin I, left ventricular ejection fraction (LVEF), and E/E′, were recorded. E/E′ is the ratio of the peak mitral early filling velocity (E) to the early diastolic mitral annular velocity (E′), as an indicator of diastolic cardiac function.
Target vessel failure (TVF) was defined as a combination of cardiogenic death, target vessel-related myocardial infarction and target vessel revascularization (TVR) (18). TVR was defined as a repeat PCI or surgical bypass of any segment of the target vessel, including the target lesion (18). All patients were followed for 5 years and received optimal guideline-based medical therapy during follow-up.
Statistical analysisContinuous variables are expressed as the mean ± standard deviation (SD) or median [interquartile range (IQR)]. Categorical variables are expressed as numbers (percentages). Continuous variables were compared by ANOVA or the Kruskal‒Wallis test, and categorical variables were compared by chi‒squared analysis. The association between the ΔQFR and 5-year TVF in the five groups was estimated by the Kaplan‒Meier method and compared by the log-rank test. Restricted cubic spline regression analysis was used to assess the association between the ΔQFR and the hazard ratio (HR) for TVF. A 2-sided P value < 0.05 was considered to indicate statistical significance. All analyses were performed with R software version 4.1.1 (R Foundation for Statistical Computing, Vienna, Austria) and SPSS version 26 (IBM, Inc., New York, NY, USA).
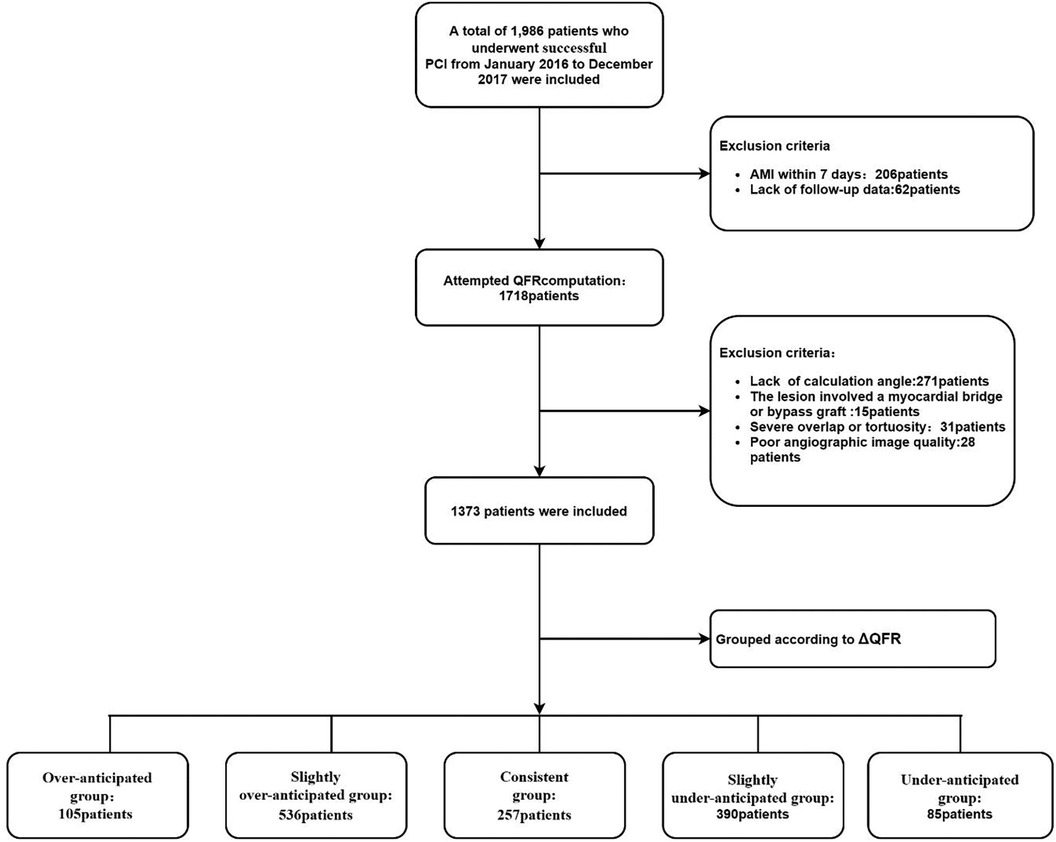
Results Study populationBetween January 1, 2016, and December 31, 2017, 1,986 patients who underwent PCI were screened for enrollment; 268 patients were excluded due to meeting the clinical exclusion criteria, and 345 patients were excluded due to meeting the angiographic exclusion criteria. The remaining 1,373 patients were included in the final analysis. According to the ΔQFR, all enrolled patients were further divided into five groups: (1) the overanticipated group: ΔQFR ≥ 0.1, n = 105; (2) the slightly overanticipated group: 0 < ΔQFR < 0.1, n = 536; (3) the consistent group: ΔQFR = 0, n = 257; (4) the slightly underanticipated group: −0.1 < ΔQFR < 0, n = 390; and (5) the underanticipated group: ΔQFR ≤ −0.1, n = 85. (Figure 1).
Figure 1. Study flowchart. PCI, percutaneous coronary intervention; STEMI, ST-segment elevation myocardial infarction; QFR, quantitative flow ratio; ΔQFR = post-PCI QFR—residual QFR.
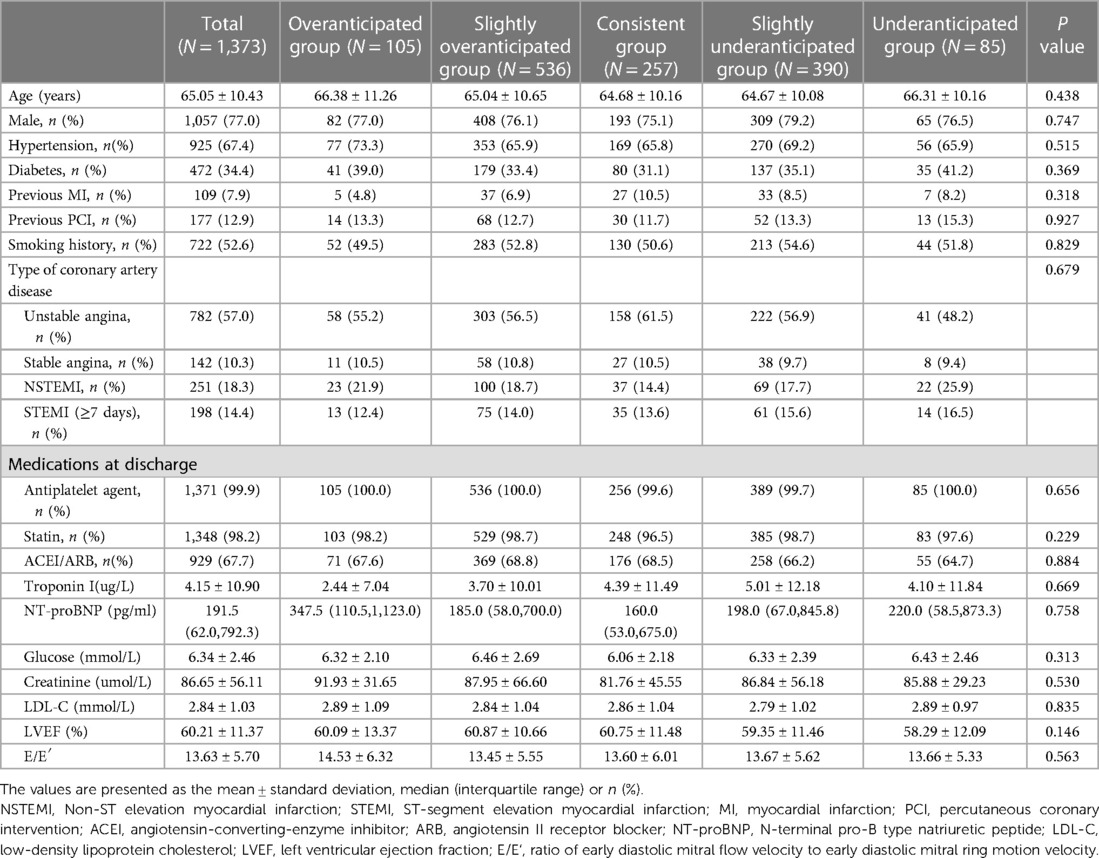
Clinical baseline characteristicsThe baseline characteristics are shown in Table 1. No significant differences were found between the groups with regard to age, sex, smoking status, hypertension, diabetes, previous MI, previous PCI, type of coronary artery disease, or post-PCI medication. Patients in the five groups had similar pre-PCI results for troponin I, LDL-C, NT-proBNP, blood glucose, serum creatinine, LVEF and E/E′.
Table 1. Baseline characteristics.
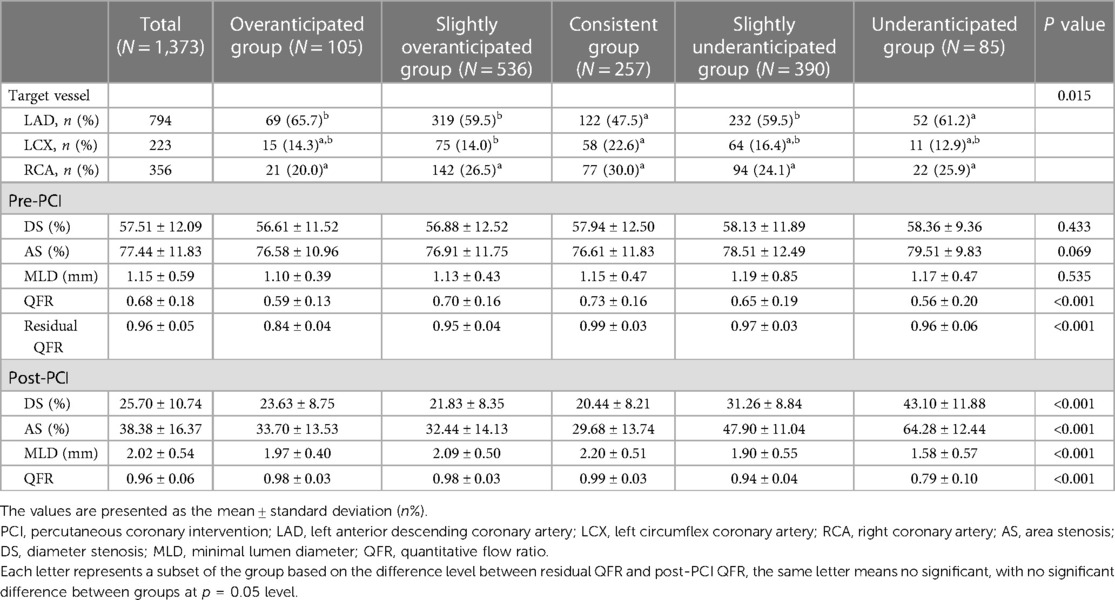
QCA and QFR analysisThe results of the QCA and QFR analyses are summarized in Tables 2, 3. In terms of target vessel locations, the consistent group had a greater proportion of LCX (22.6%) and a lower proportion of LAD (47.5%). Compared with those in the consistent group, the patients in the overanticipated group had longer stents (43.42 ± 17.47 vs. 31.41 ± 14.12, P < 0.001), more stents (1.65 ± 0.62 vs. 1.23 ± 0.45, P < 0.001), and similar stent diameters (3.03 ± 0.42 vs. 3.11 ± 0.44, P = 0.056).
Table 2. The results of the QCA and QFR analysis.
Table 3. Parameters related to the stent.
There was a significant difference in the pre-PCI QFR among the five groups (P < 0.001), with lower pre-PCI QFRs in the overanticipated group and underanticipated group. Significant differences in the post-PCI QFR were found in the five groups, of which the underanticipated group had a significantly worse post-PCI QFR than the other groups. No significant differences in DS%, AS% or MLD were found among the five groups at pre-PCI, whereas a difference was found for the post-PCI between the groups.
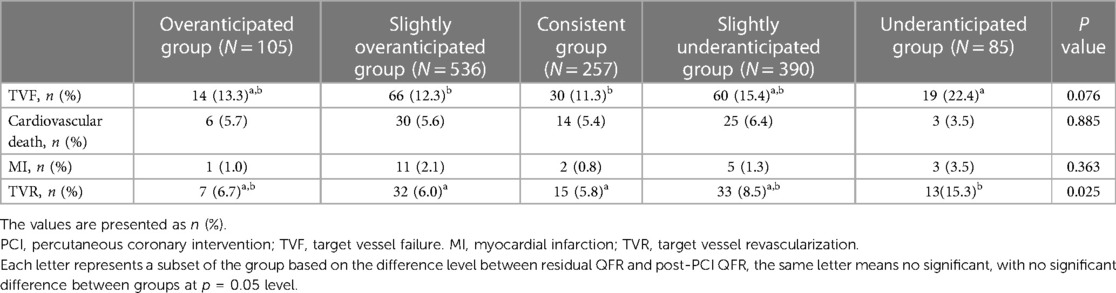
Clinical outcomesA five-year follow-up was completed for all eligible patients, with a median follow-up of 61 months. Comparisons of the clinical outcomes between the 5 groups are shown in Table 4. TVF occurred within 5 years in 189 patients in all the groups; 14 patients were in the overanticipated group, 66 patients were in the slightly overanticipated group, 30 patients were in the consistent group, 60 patients were in the slightly underanticipated group, and 19 patients were in the underanticipated group. The consistent group had the lowest incidence of TVF, and the underanticipated group had the highest risk of TVF. Supplementary Table S1 compares the difference in the incidence of TVF between the consistent group and the other groups. Supplementary Table S2 showes shows that TVF is independent of target vessel distribution. The incidence of TVF was significantly greater in the underanticipated group than in the consistent group (P = 0.008), whereas no significant differences were found when comparing the underanticipated group with the other three groups.
Table 4. Clinical outcomes at the 5-year follow-up.
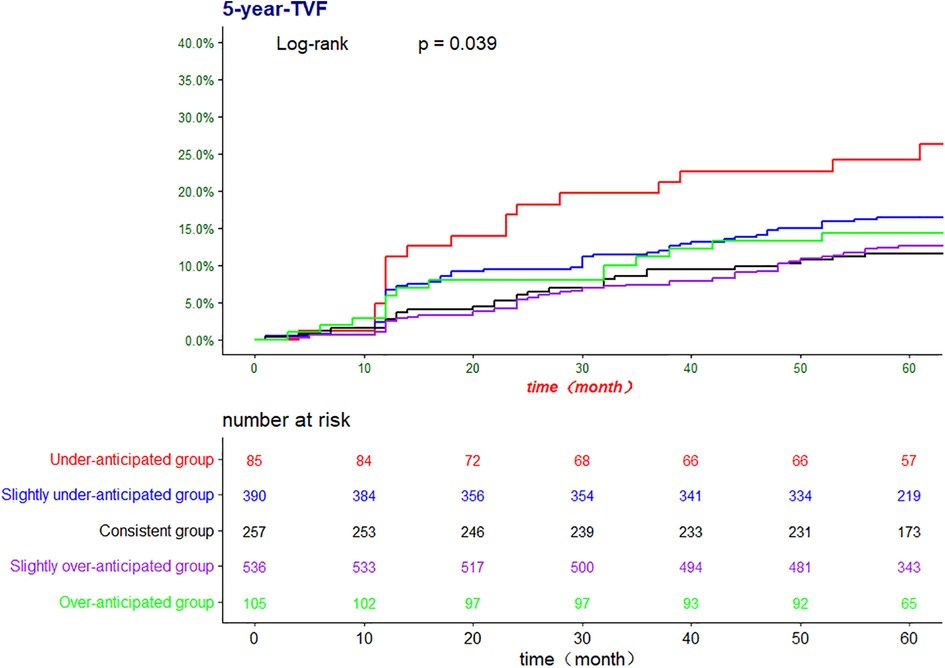
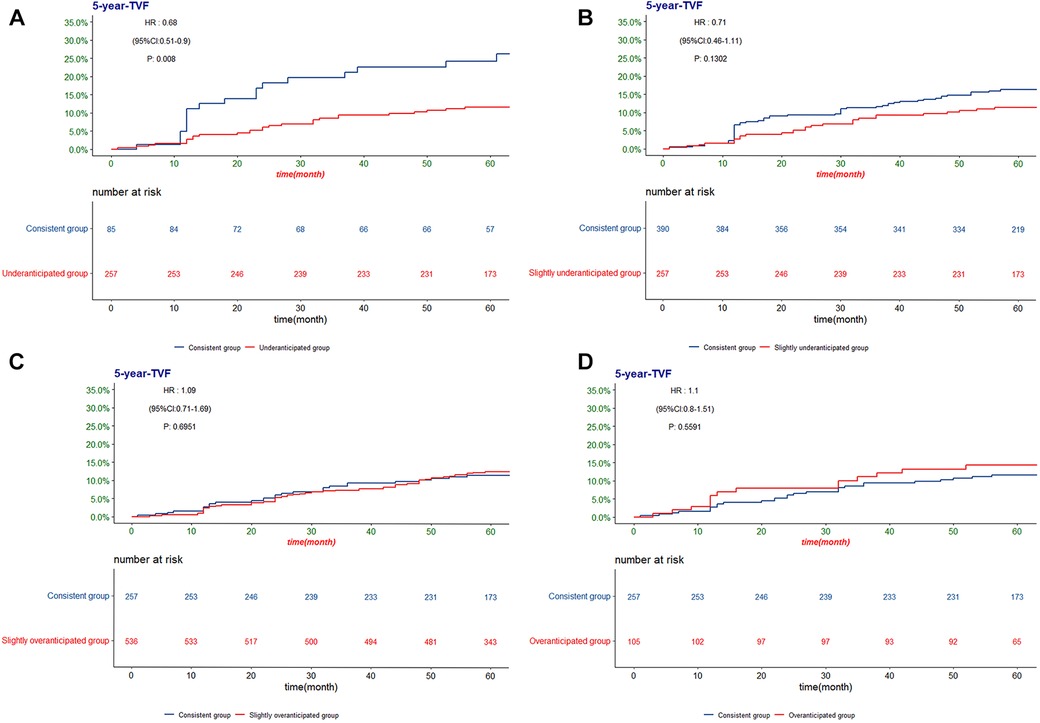
The Kaplan‒Meier method was used to further confirm the difference in the incidence of TVF among the five groups (Figures 2, 3). There was a significant difference in the risk of 5-year TVF among the five groups (log-rank P = 0.039). The incidence of TVF was lower in the consistent group than in the underanticipated group (HR = 0.068, 95% CI = 0.51–0.90, P = 0.008), while no significant differences were found between the consistent group and the remaining three groups.
Figure 2. The Kaplan-Meier analysis for TVF according to ΔQFR. TVF, target vessel failure; QFR, quantitative flow ratio; ΔQFR = post-PCI QFR—residual QFR.
Figure 3. The Kaplan-Meier analysis of TVF according to the difference between post-PCI QFR and residual QFR for the (A) consistent group and underanticipated group; (B) consistent group and slightly underanticipated group; (C) consistent group and slightly overanticipated group; (D) consistent group and overanticipated group. TVF, target vessel failure; QFR, quantitative flow ratio.
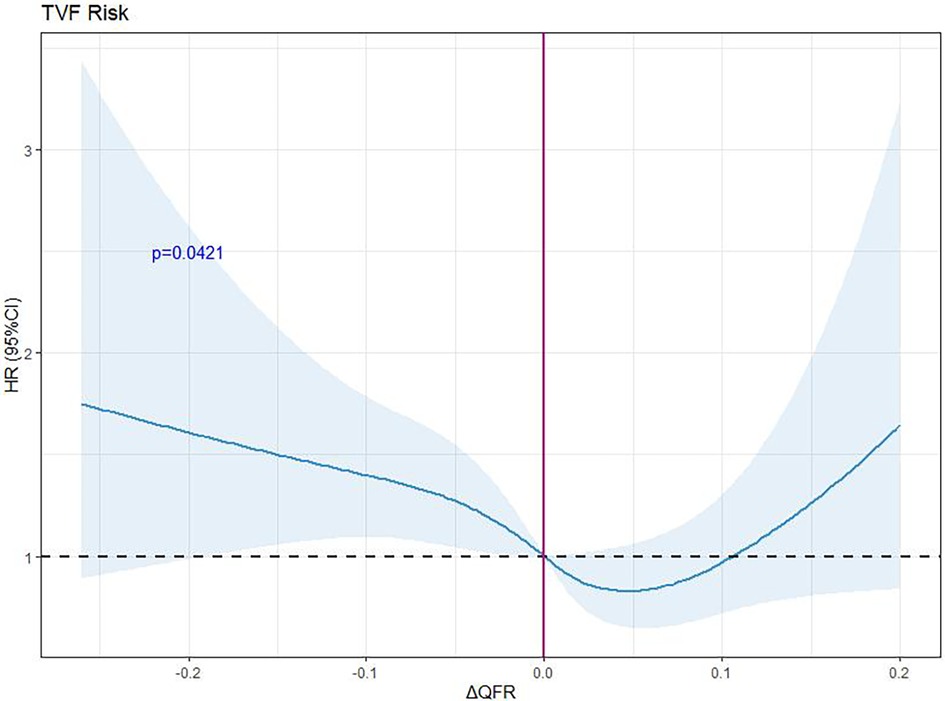
Restricted cubic spline regression analysis was used to analyze and visualize the association between ΔQFR and TVF (Figure 4). As the ΔQFR increased, the hazard ratio of TVF first decreased and then gradually increased.
Figure 4. Hazard ratios for the TVF based on restricted cubic spline. The purple line represents the reference hazard ratio, and the blue area represents the 95% confidence interval. RCS, restricted cubic spline; HR, hazard ratio; ΔQFR, postoperative QFR minus preoperative residual QFR.
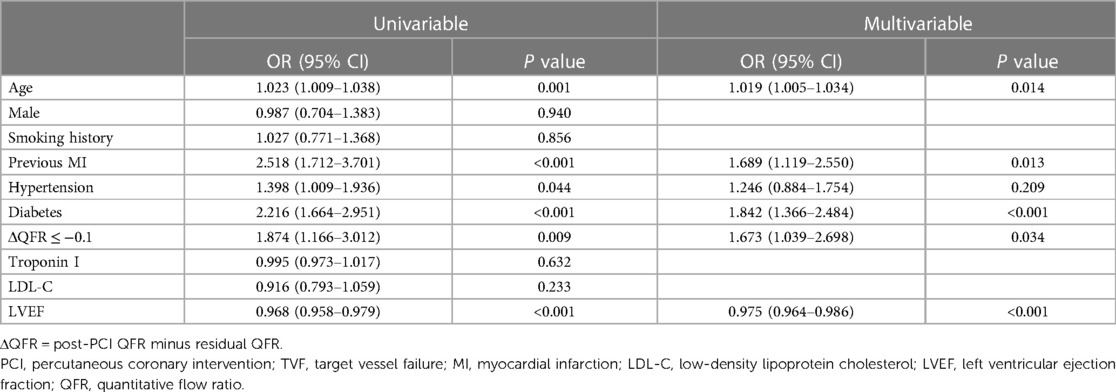
Predictive performance of the ΔQFR for 5-year TVFUnivariate analysis and multivariate Cox regression analysis were performed to evaluate the predictive performance of the ΔQFR for the 5-year TVF (Table 5). After screening via univariate Cox regression (P < 0.05), ΔQFR ≤ −0.1, age, previous MI, hypertension, diabetes, creatinine, and LVEF were included in the multivariate analysis. The multivariate analysis revealed that a ΔQFR ≤ −0.1, old age, previous MI, and diabetes were independent risk factors for TVF, and a high LVEF was an independent protective factor.
Table 5. Univariate and multivariate Cox regression analyses of factors influencing the TVF.
DiscussionThe present study was the first to evaluate the prognostic value of the consistency between the residual QFR and post-PCI QFR in TVF. The main findings are as follows: (1) The incidence of TVF in the consistent group was significantly lower than that in the underanticipated group, whereas it was similar to that in the overanticipated group, suggesting that the consistency between the residual QFR and post-PCI QFR is associated with the long-term prognosis of patients. (2) This study provides a new perspective on the residual QFR to further explore the potential of the QFR in clinical practice.
Despite successful revascularization, some patients with CAD still experience symptoms of angina pectoris or recurrent cardiovascular adverse events (19, 20). Previous studies suggest that plaque burden rather than stenosis is one of the main predictors of cardiovascular adverse events (21), which may partly explain the uncertain association between the degree of luminal stenosis and the severity of myocardial ischemia. Previous landmark studies have demonstrated the instrumental value of the QFR in guiding the PCI procedure and further improving the clinical prognosis (10–12). The residual QFR is a predicted QFR value based on coronary angiographic imaging that simulates successful stent implantation in the culprit lesion, correlates well with the post-PCI FFR and QFR, and predicts the occurrence of adverse events after revascularization (13, 14, 16, 22). A retrospective analysis of the PANDA III trial showed that the predicted clinical outcome of residual QFR-guided PCI was superior to that of angio-guided PCI (15, 23). In addition, the ability of the residual QFR to distinguish functional stenosis was confirmed (16). Compared with the post-PCI QFR, the residual QFR can predict post-PCI coronary function in advance and provide anticipated post-PCI vascular information on the culprit lesion segment, further delaying revascularization in lesions with anticipated insignificant functional benefit. The number and length of stents that are assigned to be implanted in the coronary arteries can be reduced by knowing the stenoses with relatively high treatment benefits and the coronary lesions with potentially low treatment benefits in the index PCI.
In our study, the post-PCI QFR was significantly lower than the residual QFR in the underanticipated group, with a greater incidence of TVF than in the consistent group (22.4% vs. 11.3%, P = 0.003). A multivariate Cox regression model revealed that a ΔQFR ≤ −0.1 (OR: 1.673, 95% CI: 1.039–2.698 P = 0.034) was an independent risk factor for TVF, which indicates the potential for consistency between the residual QFR and post-PCI QFR to predict adverse events; namely, a QFR significantly lower than the residual QFR is prone to be associated with TVF after successful revascularization. Accumulating evidence suggests that a poor physiological outcome may be indicative of stent malapposition, an uncovered stent, a stent under expansion, or incomplete postdialation (24). The residual QFR was calculated as the maximum QFR outside the stent segment of the entire vessel, which may lead to an inadequate assessment of stent malapposition or under expansion. A suboptimal stenting strategy may increase in-stent restenosis and endothelial hyperplasia (25), further increasing the incidence of repeat revascularization, which may explain the high incidence of TVF in the underanticipated group. The stent diameter in the underanticipated group in this study was smaller (2.96 ± 0.41 vs. 3.11 ± 0.44, P = 0.004) than that in the consistent group, supporting the previous hypothesis. A low residual QFR suggests that the target vessel may have a limited or diffuse lesion that the operator is unaware of or that the benefit of intervention for this coronary lesion is low, and this information may help to modify the PCI strategy (14). In addition, compared with the consistent group, the overanticipated group had a greater mean number of stents implanted (1.65 ± 0.62 vs. 1.23 ± 0.45, P < 0.001) and a longer total stent length (43.42 ± 17.47 vs. 30.80 ± 13.66, P < 0.001), which may have contributed to the greater post-PCI QFR than residual QFR in the overanticipated group. According to the RCS regression analysis, the risk of VTVF was nonlinearly related to the ΔQFR and had a V-shape. Although patients in the underanticipated group had a higher risk of TVF, the incidence of TVF was not reduced in the overanticipated patients. This may indicate that a more aggressive PCI strategy leads to a higher post-PCI QFR but prolongs the operation time, and too many stents may increase stent-related risks. Furthermore, the post-PCI QFR was significantly greater than the residual QFR in the overanticipated group, while the incidence of TVF was not lower than that in the consistent group (13.3% vs. 11.3%, P = 0.559), which confirms the ability of the residual QFR to discriminate less functionally beneficial coronary lesions and indicates that aggressive treatment does not reduce the incidence of adverse events in such lesions.
This study has several limitations. First, the current study was a single-center, retrospective, observational study. These findings need to be further validated by prospective, multicenter studies. Second, some patients were excluded due to the lack of optimal angiographic images for QFR analysis, which led to selection bias. In addition, the residual QFR is a novel index that provides vascular information for PCI treatment, but the accuracy and feasibility of a treatment strategy based on the residual QFR need to be further confirmed.
ConclusionsThe consistency between the residual QFR and post-PCI QFR may be associated with the long-term prognosis of patients. Patients whose post-PCI QFR is significantly lower than the residual QFR may be at greater risk of TVF. An aggressive PCI strategy for lesions anticipated to have less functional benefit may not result in a better clinical outcome.
Data availability statementThe raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statementThe studies involving humans were approved by the Ethics Committee of Union Hospital, Fujian Medical University. The studies were conducted in accordance with the local legislation and institutional requirements. The human samples used in this study were acquired from primarily isolated as part of your previous study for which ethical approval was obtained. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributionsLC: Writing – original draft, Writing – review & editing. JZ: Writing – original draft, Writing – review & editing. RH: Writing – original draft, Writing – review & editing. YC: Writing – original draft, Writing – review & editing. BL: Writing – review & editing, Data curation, Visualization. LW: Writing – original draft, Writing – review & editing. YY: Writing – original draft, Writing – review & editing. LC: Writing – review & editing. QC: Writing – original draft, Writing – review & editing. YL: Writing – original draft, Writing – review & editing.
FundingThe author(s) declare financial support was received for the research, authorship, and/or publication of this article.
This work was supported by Joint Funds for Fujian Provincial Health Technology Project (2021GGBO04); Fujian Provincial Health Technology Project (2022CXBO05). The Innovation of Science and Technology, Fujian province (Grant number: 2020Y9098).
Conflict of interestThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's noteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary materialThe Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2024.1297218/full#supplementary-material
References1. El-Hayek GE, Gershlick AH, Hong MK, Casso Dominguez A, Banning A, Afshar AE, et al. Meta-analysis of randomized controlled trials comparing multivessel versus culprit-only revascularization for patients with ST-segment elevation myocardial infarction and multivessel disease undergoing primary percutaneous coronary intervention. Am J Cardiol. (2015) 115:1481–6. doi: 10.1016/j.amjcard.2015.02.046
PubMed Abstract | Crossref Full Text | Google Scholar
2. Sethi A, Bahekar A, Bhuriya R, Singh S, Ahmed A, Khosla S. Complete versus culprit only revascularization in acute ST elevation myocardial infarction: a meta-analysis. Cathet Cardiovasc Intervent. (2011) 77:163–70. doi: 10.1002/ccd.22647
Crossref Full Text | Google Scholar
3. Al-Lamee R, Thompson D, Dehbi H-M, Sen S, Tang K, Davies J, et al. Percutaneous coronary intervention in stable angina (ORBITA): a double-blind, randomised controlled trial. Lancet. (2018) 391:31–40. doi: 10.1016/S0140-6736(17)32714-9
PubMed Abstract | Crossref Full Text | Google Scholar
4. Sugiyama T, Kanno Y, Hamaya R, Kanaji Y, Hoshino M, Murai T, et al. Determinants of visual-functional mismatches as assessed by coronary angiography and quantitative flow ratio. Cathet Cardio Intervent. (2021) 98:1047–56. doi: 10.1002/ccd.29388
Crossref Full Text | Google Scholar
5. Toth G, Hamilos M, Pyxaras S, Mangiacapra F, Nelis O, De Vroey F, et al. Evolving concepts of angiogram: fractional flow reserve discordances in 4000 coronary stenoses. Eur Heart J. (2014) 35:2831–8. doi: 10.1093/eurheartj/ehu094
PubMed Abstract | Crossref Full Text | Google Scholar
6. De Maria GL, Garcia-Garcia HM, Scarsini R, Hideo-Kajita A, Gonzalo López N, Leone AM, et al. Novel indices of coronary physiology: do we need alternatives to fractional flow reserve? Circ: Cardiovasc Intervent. (2020) 13:e008487. doi: 10.1161/CIRCINTERVENTIONS.119.008487
Crossref Full Text | Google Scholar
7. Tonino PAL, Siebert U, Manoharan G, Maccarthy PA. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention. N Engl J Med. (2009) 12.
8. Neumann F-J, Sousa-Uva M, Ahlsson A, Alfonso F, Banning AP, Benedetto U, et al. 2018 ESC/EACTS guidelines on myocardial revascularization. Eur Heart J. (2019) 40:87–165. doi: 10.1093/eurheartj/ehy394
PubMed Abstract | Crossref Full Text | Google Scholar
9. Xaplanteris P, Fournier S, Pijls NHJ, Fearon WF, Barbato E, Tonino PAL, et al. Five-year outcomes with PCI guided by fractional flow reserve. N Engl J Med. (2018) 379:250–9. doi: 10.1056/NEJMoa1803538
PubMed Abstract | Crossref Full Text | Google Scholar
10. Tu S, Westra J, Yang J, von Birgelen C, Ferrara A, Pellicano M, et al. Diagnostic accuracy of fast computational approaches to derive fractional flow reserve from diagnostic coronary angiography. JACC Cardiovasc Interv. (2016) 9:2024–35. doi: 10.1016/j.jcin.2016.07.013
PubMed Abstract | Crossref Full Text | Google Scholar
11. Westra J, Andersen BK, Campo G, Matsuo H, Koltowski L, Eftekhari A, et al. Diagnostic performance of in-procedure angiography-derived quantitative flow reserve compared to pressure-derived fractional flow reserve: the FAVOR II Europe-Japan study. J Am Heart Assoc. (2018) 7. doi: 10.1161/JAHA.118.009603
PubMed Abstract | Crossref Full Text | Google Scholar
12. Xu B, Tu S, Song L, Jin Z, Yu B, Fu G, et al. Angiographic quantitative flow ratio-guided coronary intervention (FAVOR III China): a multicentre, randomised, sham-controlled trial. Lancet. (2021) 398:2149–59. doi: 10.1016/S0140-6736(21)02248-0
PubMed Abstract | Crossref Full Text | Google Scholar
13. Rubimbura V, Guillon B, Fournier S, Amabile N, Chi Pan C, Combaret N, et al. Quantitative flow ratio virtual stenting and post stenting correlations to post stenting fractional flow reserve measurements from the DOCTORS (does optical coherence tomography optimize results of stenting) study population. Catheter Cardiovasc Interv. (2020) 96:1145–53. doi: 10.1002/ccd.28615
PubMed Abstract | Crossref Full Text | Google Scholar
14. van Diemen PA, de Winter RW, Schumacher SP, Bom MJ, Driessen RS, Everaars H, et al. Residual quantitative flow ratio to estimate post-percutaneous coronary intervention fractional flow reserve. J Interv Cardiol. (2021) 2021:1–11. doi: 10.1155/2021/4339451
Crossref Full Text | Google Scholar
15. Zhang R, Xu B, Dou K, Guan C, Zhao Y, Wang X, et al. Post-PCI outcomes predicted by pre-intervention simulation of residual quantitative flow ratio using augmented reality. Int J Cardiol. (2022) 352:33–9. doi: 10.1016/j.ijcard.2022.01.054
PubMed Abstract | Crossref Full Text | Google Scholar
16. Guan S, Gan Q, Han W, Zhai X, Wang M, Chen Y, et al. Feasibility of quantitative flow ratio virtual stenting for guidance of serial coronary lesions intervention. J Am Heart Assoc. (2022) 11:e025663. doi: 10.1161/JAHA.122.025663
PubMed Abstract | Crossref Full Text | Google Scholar
17. Authors/Task Force members; Windecker S, Kolh P, Alfonso F, Collet JP, Cremer J, Falk V, et al. 2014 ESC/EACTS guidelines on myocardial revascularization: the task force on myocardial revascularization of the European society of cardiology (ESC) and the European association for cardio-thoracic surgery (EACTS) developed with the special contribution of the European association of percutaneous cardiovascular interventions (EAPCI). Eur Heart J. (2014) 35:2541–619. doi: 10.1093/eurheartj/ehu278
PubMed Abstract | Crossref Full Text | Google Scholar
18. Garcia-Garcia HM, McFadden EP, Farb A, Mehran R, Stone GW, Spertus J, et al. Standardized end point definitions for coronary intervention trials: the academic research consortium-2 consensus document. Circulation. (2018) 137:2635–50. doi: 10.1161/CIRCULATIONAHA.117.029289
PubMed Abstract | Crossref Full Text | Google Scholar
20. Stone GW, Ellis SG, Gori T, Metzger DC, Stein B, Erickson M, et al. Blinded outcomes and angina assessment of coronary bioresorbable scaffolds: 30-day and 1-year results from the ABSORB IV randomised trial. Lancet. (2018) 392:1530–40. doi: 10.1016/S0140-6736(18)32283-9
PubMed Abstract | Crossref Full Text | Google Scholar
21. Mortensen MB, Dzaye O, Steffensen FH, Bøtker HE, Jensen JM, Rønnow Sand NP, et al. Impact of plaque burden versus stenosis on ischemic events in patients with coronary atherosclerosis. J Am Coll Cardiol. (2020) 76:2803–13. doi: 10.1016/j.jacc.2020.10.021
PubMed Abstract | Crossref Full Text | Google Scholar
22. Li Z, Zhan J, Han J, Fu G, Jin C. Comparison of diagnostic accuracy of immediate angiography derived residual quantitative flow ratio after bioresorbable scaffold and drug eluting stent implantation. Rev Cardiovasc Med. (2022) 23:059. doi: 10.31083/j.rcm2302059
Crossref Full Text | Google Scholar
23. Xu B, Gao R, Yang Y, Cao X, Qin L, Li Y, et al. Biodegradable polymer-based sirolimus-eluting stents with differing elution and absorption kinetics. J Am Coll Cardiol. (2016) 67:2249–58. doi: 10.1016/j.jacc.2016.03.475
PubMed Abstract | Crossref Full Text | Google Scholar
24. Wolfrum M, De Maria GL, Benenati S, Langrish J, Lucking AJ, Channon KM, et al. What are the causes of a suboptimal FFR after coronary stent deployment? Insights from a consecutive series using OCT imaging. EuroIntervention. (2018) 14:e1324–31. doi: 10.4244/EIJ-D-18-00071
PubMed Abstract | Crossref Full Text | Google Scholar
25. Song H-G, Kang S-J, Ahn J-M, Kim W-J, Lee J-Y, Park D-W, et al. Intravascular ultrasound assessment of optimal stent area to prevent in-stent restenosis after zotarolimus-, everolimus-, and sirolimus-eluting stent implantation: IVUS optimization of stent area. Cathet Cardiovasc Intervent. (2014) 83:873–8. doi: 10.1002/ccd.24560
留言 (0)