
記住我

One-hundred sixty-six papers were eligible for full text analysis and 68 were considered relevant as they provided original, non-redundant information on VN treatment. Among the relevant papers, 28 were clinical trials, 6 were post-hoc analyses and 34 described real-world experience (Fig. 1).
Fig. 1: PRISMA flow diagram of the paper selection process.
Graphical summary of the paper screening process, with the number of articles found by the different databases and the selection process. Numbers of articles are recorded at the different stages.
Findings of cross-sectional and longitudinal natural history studies: patients’ age, clinical characteristics and disease severityRPE65-associated IRD phenotypes are described in the literature with different terms, as shown by the data charting (Supplemental material).
Visual function degeneration is assessed by best-corrected visual acuity (BCVA), kinetic VF, dark-adapted perimetry and, more recently, full filed sensitivity threshold (FST). The pupillary light reflex assessment was an endpoint only in the phase 1 trial [26]. Recently the evaluation of chromatic pupil campimetry (CPC) has been introduced (see below) [27].
Overall, BCVA is severely compromised since childhood and worsens with age [8]. Consistent findings were provided by different groups [8,9,10]. A broad inter-individual visual acuity (VA) variability is observed in the first decades of life, and tends to stabilise in early adulthood with progression toward blindness [9], as highlighted by Testa et al., through a time-to-event analysis, predicting a median age of blindness within the fourth decade of life [10].
Similarly, Goldmann VF worsens with age [8, 9, 28], while no clear relationship between age and residual rod function is reported for FST [28]. Although age appears associated with worsening of functional parameters, its role as an absolute criterion for patient eligibility is not confirmed yet. Residual rod function is likely related to preserved photoreceptors rather than age.
We analysed phenotypes and disease severity based on eye fundus, outer nuclear layer (ONL) thickness and age in cross-sectional and longitudinal studies to gather a more comprehensive overview of the patient population and identify the stage that may preclude the treatment.
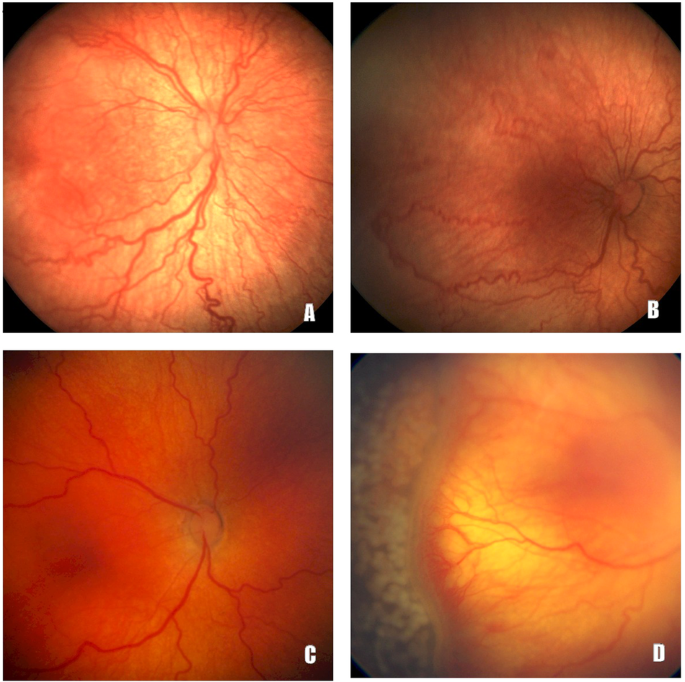
Fundus abnormalities worsen from the second decade of life, as reported in cohorts of either paediatric or adult patients with LCA or EOSRD (age range 1–54 years), and are more pronounced in older patients [8, 29]. However, in the assessment of age-related fundus abnormalities, ethnicity should be considered. In a Chinese cohort of 30 LCA or EOSRD patients aged 1–45 years, age-dependent phenotypes were slightly different from Caucasian patients: maculopathy and bone spicules commonly reported in Caucasian patients at any age were, instead, described only in adulthood in the Chinese cohort [30].
A longitudinal observation of 43 LCA or EORD patients over 5 years showed no changes in fundus appearance; patients with retinitis pigmentosa (RP) fundus appearance were significantly older [10]. An assessment of disease severity by VF and retinal function may give more sensitive information to characterise patients’ eligibility for VN treatment.
Evaluation of ONL thickness may also be useful. However, ONL thickness mapping revealed variability [31], as foveal ONL thickness in a group of 11 patients aged 11–53 years showed normal thickness in ~50% of subjects, despite an abnormally reduced vision. ONL thickness was greater than expected for the level of dysfunction. In a group of 9 paediatric RPE65-LCA patients, ONL thickness topography showed that superior-temporal regions appeared to be the least affected by the degeneration, likely due to the higher rod density, making this area a preferential target for vector delivery. Nevertheless, a broad inter-individual difference was reported. To assess disease severity, the authors recommended a detailed cross-sectional retinal imaging regardless of patient age [31].
Further analysis of ONL thickness was performed in natural history studies over a mean of 1.9 years and 3.9 years by Chung and Testa, respectively [8, 10]. Again, age was not associated with disease severity when ONL thickness by optical coherence tomography (OCT) B-scans were considered in 32 out of 70 patients of 6–38 years of age [8]. This finding is consistent with a non-significant decline in central foveal thickness (CFT) over almost 4 years of follow-up in 25 Italian patients. Furthermore, ONL and CFT thinning were reported in the majority of patients, as well as a more frequent alteration of the ellipsoid zone in extrafoveal areas with a minority of eyes having signs of RPE atrophy [10].
In another longitudinal study [9], 12 patients aged 5–19 years and 8 adults showed a mean reduction of retinal thickness and of ONL and outer retinal layers thickness, while the ganglion cell layer was preserved. Retinal architecture resulted well preserved in the youngest patient.
Dark-adapted static perimetry was evaluated in 17 patients to provide a disease staging: the visual deterioration occurs in sequence, starting with uniform vision loss in the periphery, followed by a more prominent loss in the mid-peripheral area eventually culminating in a complete scotoma within the 30° to 60° range, which expands to involve the central field of vision [28].
As emerged from natural history and cross-sectional studies, RPE65-LCA or EOSRD patients deal with progressive functional and structural deterioration since birth or infancy but in the meantime, disease progression rate and severity might widely differ regardless of age. This should be considered when assessing eligibility for treatment: multiple functional and structural parameters are needed to characterise each patient and to determine the potential for functional rescue. Disease severity staging and progression have been analysed in patients within their fifth decade, but elder patients might be encountered in real life.
Psychophysical tests and imaging performed pre-and post-treatment for RPE65 patients’ evaluationEighty-nine patients, ranging from 4 to 44 years, diagnosed with LCA or EOSRD caused by RPE65 biallelic mutation were included in clinical trials investigating the safety and efficacy of 3 types of vectors [15, 26, 32,33,34]. In these studies, functional and structural disease severity overlapped. To avoid bias when interpreting real-world treatment results, we analyse only VN clinical development, which included 41 patients with 81 eyes: Table 1 lists inclusion criteria for VN clinical development.
Table 1 Main inclusion criteria for VN phase1/2 and 3 clinical trials [7, 15].Clinical trials demonstrated the beneficial effect of VN treatment [7, 15]. One of the major challenges in the clinical development of a therapy for IRD patients with severe visual impairment is the definition of the therapeutic efficacy. Functional vision improvement, measured by a validated multi-luminance mobility test (MLMT), was the primary endpoint in the clinical trials [15]. Patients in phase 1 and 3 trials presented a similar MLMT improvement [15, 26, 35]. Moreover, the improved score at day 30 remained stable during follow-up (4 years) [36]. FST was also used as an endpoint assessment and was improved after one year and stable up to 4 years after treatment [36]. MLMT is not routinely used in the majority of clinics, while FST change over time can be considered a marker of functional vision improvement [37].
Noteworthy, the analysis of individual subject data reported in the follow-on study [35] showed that out of the 10 subjects who received treatment in both eyes, only two patients (CH06 and CH12) experienced minimal benefit in the second eye. Specifically, for patient CH06, an additional mutation in the RH12 gene was discovered. Patient CH12 was the eldest (46 years old) with the worst visual acuity score (Hand Motion). However, the first two patients treated in the phase 1 study had Hand Motion visual acuity in their most affected eye and improved visual acuity score, central VF and pupillometric response as described in the initial report of the phase 1 study [7]. The analysis of single patient data from the phase 3 study showed that the only patient for whom the MLMT score did not improve (nor FST, VA, or VF) was the one with the most severe clinical phenotype (unable to undergo MLMT at the highest brightness level before treatment) [15]. These data suggest that the marked reduction in functional parameters is associated with more advanced retinal degeneration and may indicate lower therapeutic benefit. However, from the available information is not possible to evaluate whether this difference in efficacy is related to the different preservation of the retinal structure, as the morphological information provided was limited due to the poor quality of the OCT scans acquired with time-domain technology, and to the presence of nystagmus in several patients [7]. The lack information related to the retinal layers condition does not allow to evaluate treatment impact on disease progression over time.
Following VN marketing authorisation, patients treated in clinical settings are in total 103. They are affected by LCA or EOSRD with ages ranging between 2–44 years. Their clinical features are similar to those described in clinical trials (see Table 1), likely due to the adoption of the same eligibility criteria, despite the different treatment reimbursement policies among countries. In Italy, Health Authority set eligibility criteria as follows: age ≥3 years, VA ≥ 0.5LogMAR and retinal thickness >100 µm. These parameters alone cannot be considered fully reliable biomarkers of a sufficient number of viable cells and cannot distinguish between RPE and photoreceptors’ conditions [4]. Furthermore, VA worsening over time is not considered as a criterion despite in some cases the disease can progress faster than what observed in the natural history study [8].
Table 2 reports the summary of patients’ characteristics and the main results obtained in five real-world studies with at least four treated patients [16, 17, 27, 38, 39]. Patients’ baseline characteristics were not homogeneously reported, which hinders the comparison, but eligibility criteria reflected those used in the VN phase 3 trial: a wide range of BCVA and Goldman VF data were reported in only three studies [16, 17, 38]. In addition, only three studies [16, 17, 38] evaluated light sensitivity threshold with FST in response to white colour stimulus, but only Sengillo et al. described the autofluorescence patterns at baseline [16].
Table 2 Summary of real-world data from a retrospective analysis of cohorts comprising at least four patients.Treatment outcomes were also reported based on different parameters: 2 studies [16, 27] reported VA stability and three VA improvement [16, 17]. Two studies [16, 17, 38] showed improvements in Goldmann VF and four in FST light sensitivity [16, 17, 27, 38].
Age dependence of therapy efficacy has been controversial when comparing VN phase 1 results to other vectors: Maguire et al. found a correlation between age and pupillary light reflexes response in the phase 1 trial with VN, and FST improvement was noteworthy in the youngest patients [7]. On the contrary, in 15 patients treated with another RPE65 vector, age did not influence FST, transient pupillary light reflex and VA [32].
Different relationships between functional parameters and age have been found in real-life: in a group of five patients aged 14–36 years, dark-adapted campimetry (DAC) cyan stimuli correlated strongly with the age of the patients, while the increase of the average macular scotopic CPC response showed poor correlation [27]. On the contrary VN effect on BCVA seems not to be influenced by age or even by pre-treatment value [16]. Most importantly, the FST consistently improved across all studies and VA improved in the paediatric cohorts [16, 17, 27, 38].
Information on retinal morphology by OCT scans was heterogeneous: reduced central retinal thickness before the treatment was described in three studies [10, 16, 17], and reduced total retinal thickness was observed in 70% of patients by Sengillo et al. [16], while Deng et al. reported a decrease in the mean value of total retinal thickness [17]. Testa et al. reported a significant thickening of ONL in the perifoveal area measured by Spectral Domain (SD)-OCT after treatment, supporting ONL thickness as a marker of efficacy and treatment impact on disease progression [39].
Paediatric patients seem to benefit more from treatment despite functional testing being frequently unreliable. Recent works attempted to list all the tests used across IRD centres for the diagnosis and follow-up and tried to find an agreement for children’s assessment without any appreciable indication so far [3, 40].
New imaging techniques could help in overcoming the difficulties in the early-age paediatric population [41]. In 2020, Levi et al. reported the case of a 9-year-old girl displaying autofluorescence along the VN-treated area confirming treatment efficacy [42]. Despite being promising, quantitative autofluorescence and other advanced imaging techniques are still poorly diffused, not affordable for wide clinical pre- and post-operative assessment, and their utility for young children is still to be demonstrated [43]. Gerhardt et al. reported that FST was reliable as a marker of function in the assessment of only two out of four children. However, the authors reported that these two eyes showed a partial recovery on electroretinography (ERG) that was undetectable before treatment [38].
Finally, the increased interest in patient-reported outcomes and the need for functional tests encouraged the assessment of patient perspective [44, 45].
Overall, gene therapy provided positive results for the treated patients, supporting the validity of clinical trials’ inclusion criteria. However, with some exceptions of very young patients, the age range and phenotypes considered do not represent the heterogeneity of all cases and might exclude potential eligible patients.
Advanced non-routine tests to evaluate treatment outcomesBesides the measurements of visual function and retinal structure described above, some authors have attempted to carry out alternative tests to assess visual or retinal structure pre- and post-treatment.
Concerning visual function, functional magnetic resonance imaging (fMRI) objectively demonstrated that the visual cortex recovers function in specific areas of the retina with prolonged visual deprivation, when exposed to AAV2-hRPE65v2, confirming that gene augmentation therapy is effective for brain function [46]. Notably, fMRI can assess the visual function improvement durability [47]. In a clinical trial involving ten LCA2 patients unilaterally treated with VN, a non-invasive multimodal neuroimaging protocol evaluated the potential impact of gene therapy on structural transformations in the brain. The treated eyes showed a remyelination of geniculostriate fibre axons and local modifications within the primary visual cortex, underscoring gene therapy’s involvement in inducing structural changes that contribute to the overall enhancement of visual capabilities [48].
Some studies used peculiar imaging and functional tests to describe treatment outcomes: for instance, Stingl et al. reported improvements in CPC and DAC. CPC is an objective measure of retinal area that has undergone sensitivity improvement, while DAC provides differential maps of rods and cones sensitivity [27]. Both methods could enable a precise determination over time of the treatment effects.
OCT B-scan is currently recognised as the standard procedure to determine the state of retinal layer degeneration in RPE65 patients and of photoreceptor viability [4, 19,
留言 (0)