We experienced two cases of strangulated SBO after LLND in laparoscopic and robot-assisted surgery for rectal cancer. In both cases, emergent operations were necessary. The band in the first case was the left obturator nerve, whereas the other was the right umbilical cord. The two cases both had a closed-loop in the pelvic cavity, but with different symptoms. It was difficult to speculate on the cause of the SBO. Especially in the first case, the patient presented with atypical symptoms for a SBO, including severe pain in the left thigh without abdominal pain. Symptoms of the first case were thought to have a background of Howship–Romberg sign (HR sign). If we had had experience with cases of internal hernias after LLND, we might have been able to keep this possibility of internal hernias in mind and could have accurately assumed the pathogenesis of the hernia preoperatively.
The most common cause of SBO is surgical adhesions. Internal hernias account for approximately 0.5–5.8% of all cases of intestinal obstruction. More than 90% of all internal hernias are caused by natural or artificial orifices built by the intestine [1]. Internal hernias are an uncommon cause of an SBO, but it is more uncommon that an exposed blood vessel and nerve after pelvic lymphadenectomy (PL) form an internal hernia and cause of an SBO.
PL including LLND is one of the standard procedures performed for several malignant diseases, such as ovarian, cervical, endometrial, prostate, bladder, and rectal cancers [2,3,4,5,6,7]. We searched the PubMed database using the key words “internal hernia”, “pelvic lymphadenectomy (or lymph node dissection)” between 1978 and 2022. 21 cases have been described in 18 reports, including ours (Table 1) [8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24]. Strangulated internal hernia involving the right common iliac artery after PL in a patient with testicular cancer was first reported in 1978 [8]. No report for 30 years thereafter described strangulated internal hernia related to skeletonized vessels or nerves after PL. In 2008, Kim et al. reported strangulated internal hernia involving the right external iliac artery in a patient with cervical cancer [9]. Since then, case reports of PL-related strangulated SBO are increasing in recent years. Ten cases were reported in gynecology, six in urology, and three in gastrointestinal surgery. In previous reports, the external iliac artery and common iliac artery were the most common causes of SBO. In general, PL in gynecology and urogynecology involves an intensive dissection for the lymph nodes whole around the common iliac artery and external iliac artery [2, 3, 5]. On the other hand, these lymph node dissections can be omitted in rectal cancer [7]. Therefore, there are few reports in rectal cancer.
Table 1 Reported cases of strangulated small bowel obstruction after pelvic lymphadenectomySBO caused by adhesions is significantly less common with laparoscopic surgery [25]. However, in our cases, the laparoscopic and robot-assisted surgery may have reduced adhesions and preserved the mobility of the intestinal tract, which may have facilitated the small intestine to fit into the gap formed by the nerves and blood vessels exposed by the lymph node dissection. Nine of ten cases previously reported in gynecology were postoperative laparoscopic cases. Except for the first report, in urology, five cases were performed laparoscopically or robot-assisted surgery. This may be due to the fact that postoperative adhesions are less likely to occur in these cases.
The 2014 JSCCR Guidelines for Treatment of Colorectal Cancer list total mesorectal excision (TME) or mesorectal excision (ME) with LLND as the standard procedure for lower rectal cancer in Japan [26]. In the JCOG0212 study, ME with LLND had a lower local recurrence, especially in the lateral pelvis, compared to ME alone [27]. As for the approach method, the usefulness of laparoscopic or robot-assisted rather than open approaches have been reported [28, 29]. In our hospital, LLND has been performed laparoscopically since 2013 and robot-assisted since 2018, and we experienced two cases of this disease. In previous reports, both cases of rectal cancer were performed laparoscopic or robot-assisted surgery [15, 18]. Although LLND is not standard in Western countries, technical improvements in minimally invasive surgery have resulted in rapid technical standardization of this complicated procedure [30]. Laparoscopic and robot-assisted approaches to LLND for rectal cancer are becoming ordinary, so it is very important to be aware of this disease.
In previous reports, most of the patients complained of abdominal symptoms, but when the obturator nerve forms an internal hernia and caused intestinal obstruction, some patients, including the case 1, complained of inguinal or thigh pain.[18, 24]. Therefore, it is necessary to be very careful when examining the patient with a history of PL.
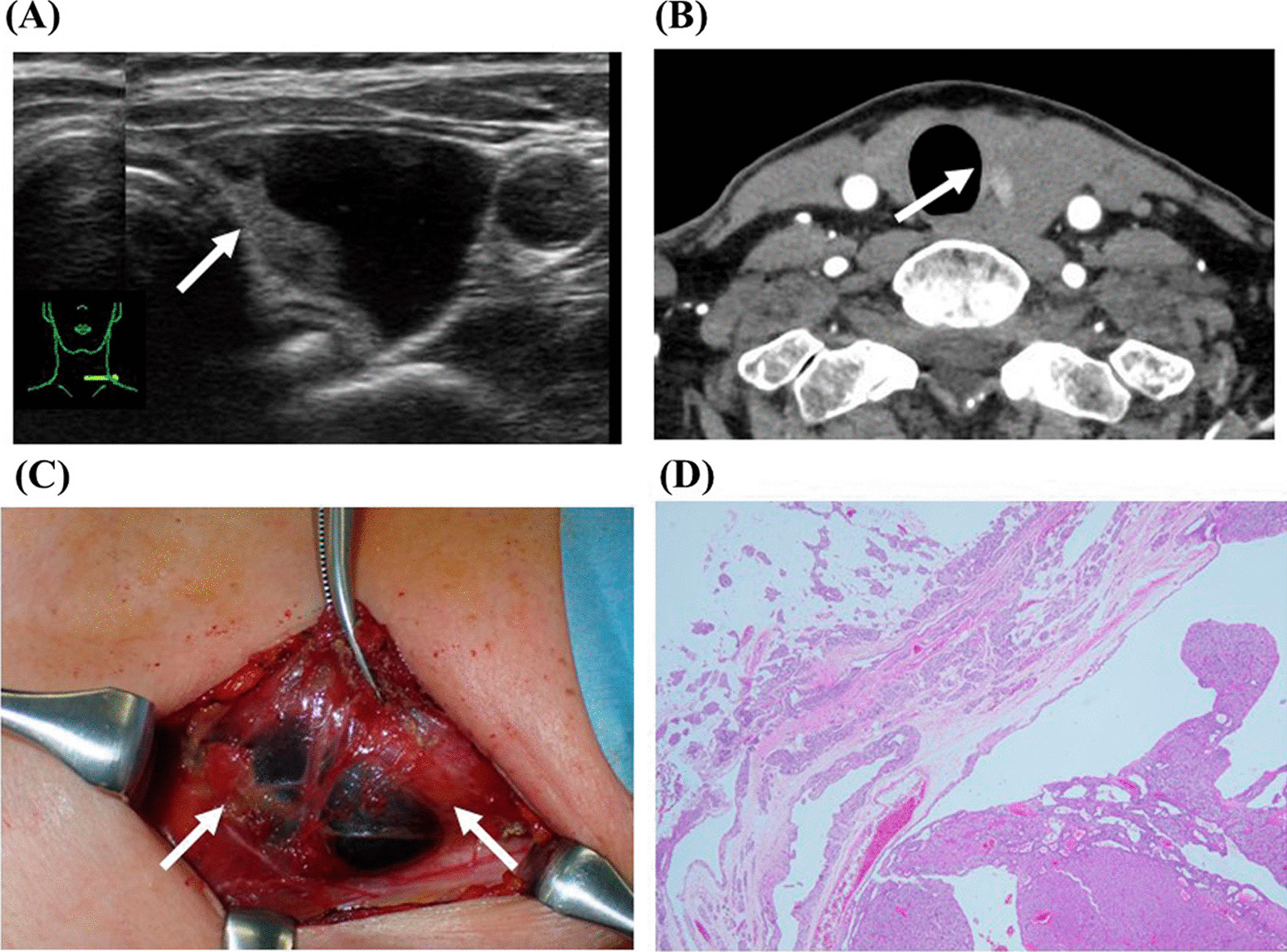
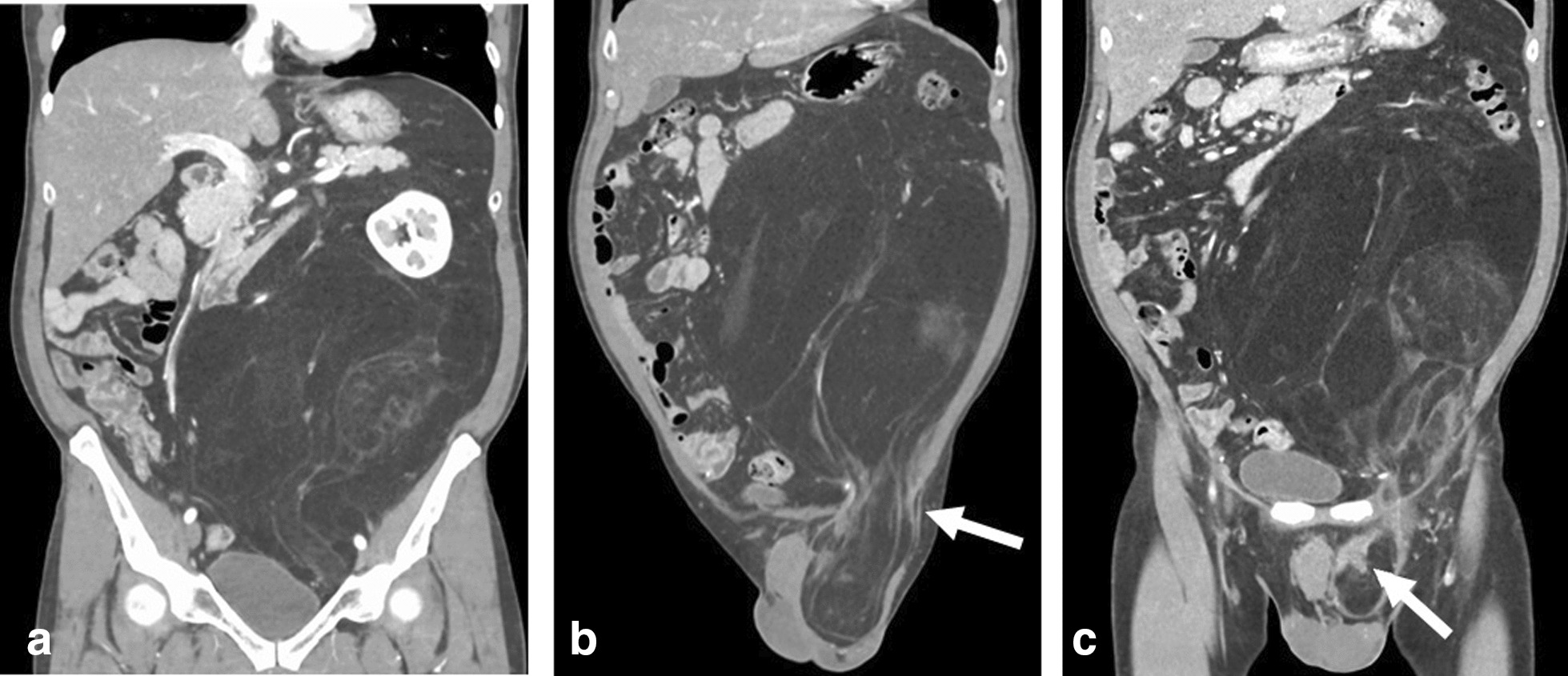
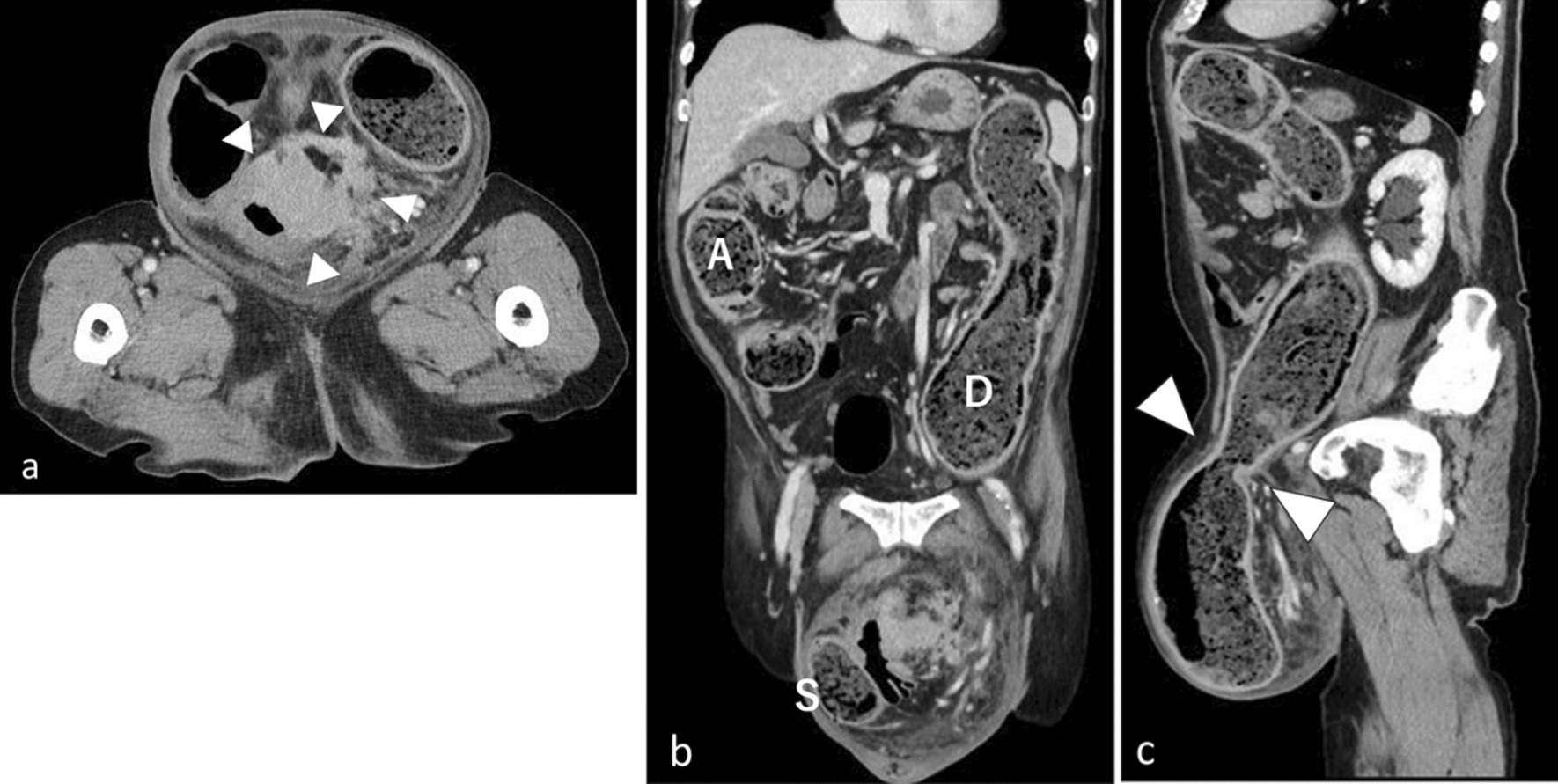
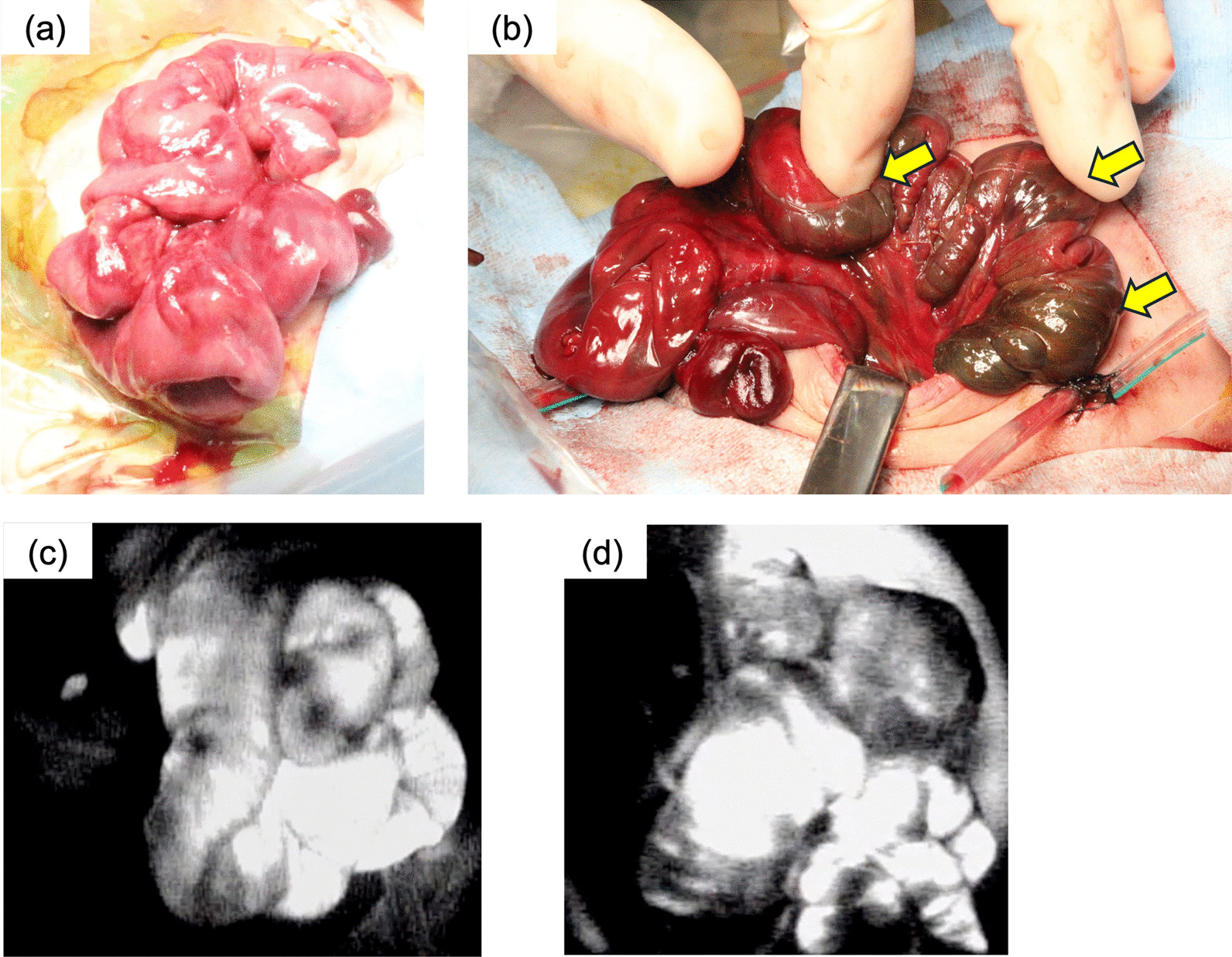
In both of the two cases, we found characteristic findings in the pelvis on CT. The small intestine strangulated by internal hernia is seen in the pelvis, and the starting point of the intestinal obstruction is located in the lateral pelvic wall in both cases. Similar CT findings have been seen in several previous reports [15, 16, 24]. If a patient with a history of PL presents with symptoms of SBO, physical findings, or HR sign, and we find characteristic CT findings in the pelvis, we need to consider this disease as a SBO formed by an internal hernia with exposed vessels and nerves in the pelvis. As in the second case, there was a case reported in the past in which the diagnosis of internal hernia was not made, and it took a long time before surgery was performed [24]. If we diagnose this disease, the internal hernia is unlikely to be resolved, so we should perform surgery as soon as possible.
Based on our experience with only two cases of SBO due to an internal hernia in the pelvis, we can expect little or no intra-abdominal adhesions in cases of bowel obstruction. Therefore, a more minimally invasive laparoscopic approach should be considered. However, the second case could have been performed laparoscopically, the dilated small intestine obstructed the development of the surgical field, making surgical manipulation difficult in some situations. As a countermeasure, in order to secure the best possible surgical field and to perform the laparoscopic surgery more reliably, if there is no intestinal ischemia and there is time to spare before the surgery, a nasogastric tube or ileus tube should be implanted before the surgery to decompress the intestinal tract and reduce intestinal dilatation.
Prevention of internal hernias at the time of initial surgery is also an important issue, but there is no clear consensus on this issue. Prevention of internal hernia by peritoneal closure at the time of initial surgery or by covering with an artificial material may be considered. However, peritoneal closure may cause pelvic lymph fistula, and artificial covering may cause infection. So far there is no effective internal hernia prophylaxis at the time of initial surgery. Therefore, we believe it is important to keep this disease firmly in mind and to respond promptly and appropriately if a patient with this condition is seen.






留言 (0)