
記住我
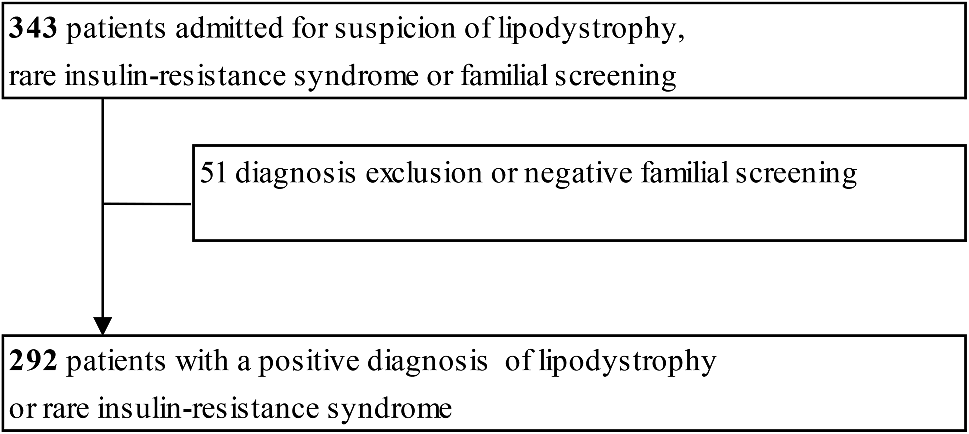








This qualitative study consisted of semi-structured interviews with all nine of the principal investigators who participated in the idursulfase-IT phase 2/3 trial (HGT-HIT-094; NCT02055118) and extension trial (Fig. 1, SHP609-302; NCT02412787) [13, 14]. These investigators enrolled the 56 patients with neuronopathic MPS II who qualified for the extension phase of the trial.
Interviews were conducted at or 36 months after patient enrollment into the initial phase of the trial. The primary objective of the interviews was to understand better, from an expert perspective, the overall treatment effects observed by the clinicians that may not have been captured by the instruments (DAS-II and Vineland Adaptive Behaviors Scale [VABS-II]) used in the idursulfase-IT trials.
Fig. 1
Overview of patient flow for the study and timing of interviews
Phase 2/3 idursulfase-IT trial designThe design of the phase 2/3 idursulfase-IT trial and extension have been described previously [13]. Briefly, the phase 2/3 trial was a 52-week, controlled, randomized, two-arm, open-label, assessor-blinded, multicenter study, in which eligible patients (n = 49) were randomized (2:1) to receive monthly idursulfase-IT 10 mg or no IT treatment, respectively, in addition to weekly intravenous idursulfase. Participants were males aged from 3 to under 18 years, with diagnosed MPS II and cognitive impairment. Idursulfase-IT was administered via a SOPH-A-PORT Mini S intrathecal drug delivery device or lumbar puncture in the event of device malfunction. In parallel to the phase 2/3 trial, a separate, 52-week, open-label, single-arm substudy was conducted in boys aged under 3 years (n = 9), in which all patients received monthly idursulfase-IT in addition to weekly intravenous idursulfase [15].
Patients who completed the phase 2/3 trial (n = 47) or substudy (n = 9) were eligible for enrollment into the open-label, non-randomized extension trial. All 56 patients in the extension phase received monthly idursulfase-IT in addition to weekly intravenous idursulfase. Treatment groups were defined according to treatment received before the extension phase: the early-IT group received idursulfase-IT in the phase 2/3 trial or substudy, whereas the delayed-IT group did not receive idursulfase-IT until entering the extension.
The primary endpoint in the pivotal phase 2/3 trial was change from baseline in DAS-II GCA at 52 weeks [13]. The DAS-II GCA score is a measure of verbal, non-verbal and spatial clusters of the DAS-II that provides an overall score of cognitive performance, in which higher values indicate better cognitive function (mean, 100; standard deviation [SD], 15). The DAS-II GCA score was assessed with one of two overlapping, age-based batteries in the DAS-II: the early-years battery (for children aged from 2 years 6 months to 6 years 11 months) and the school-age battery (for children aged from 7 years 0 months to 17 years 11 months). These batteries are fully co-normed for ages 5 years 0 months through to 8 years 11 months [16]. In the substudy, the Bayley Scales of Infant Development, Third Edition (BSID-III) was utilized as a measure of cognitive function until the patients reached 42 months of age, when their cognitive function was assessed with the DAS-II instrument if a neuropsychologist determined the child could be evaluated using this instrument [15]. The substudy patients were assessed with two of the five scales in the BSID-III instrument (cognitive and language). A score of 90–109 is considered to be average, 80–89 low average, 70–79 borderline, and 69 and below extremely low [17]. In both, adaptive behavior was assessed using VABS-II. The VABS-II Adaptive Behavior Composite score provides an overall measure of adaptive behavior ability in children and is a composite score of four domains (communication, daily living, socialization and motor skills [only included for children younger than 7 years]; mean, 100; SD, 15).
Interview methodologyVerbal consent to participate and to be audio recorded was given by each investigator prior to the start of the interview. Each investigator was reminded that the interviews would be audio recorded and that these recordings would be transcribed for use in preparing a written summary report of the interviews. Interviews lasted approximately 90 min and were conducted in the investigator’s native language over the telephone by RTI Health Solutions (Research Triangle Park, NC, USA) or Global Perspectives (Calle General Yagüe 3, Oviedo, Spain). Interviews were conducted in English for investigators in the USA, UK, Canada and Australia; in Spanish for investigators in Spain and Mexico; and in French for investigators in France.
Each interview followed a semi-structured interview guide, which was developed by RTI Health Solutions in collaboration with the study sponsor, Takeda. This guide served as a topic guide that encouraged spontaneity of responses and fostered a relaxed tone throughout the interview, and was not intended to be followed in a verbatim question format. The interview started with general questions about the investigator’s experience with neuronopathic MPS II, followed by an examination of the investigator’s clinical impressions and opinion-based assessments of: (1) the applicability, relevance and interpretation of the DAS-II and VABS-II tests; (2) caregivers’ opinions on the treatment effects of idursulfase-IT; (3) the disease status/progression of their patients or patients from other sites; and (4) the general efficacy and safety of idursulfase-IT. Interviewers were trained on the interview process to ensure consistency of data collection across interviews.
Investigators’ global ratings of disease status of their own patientsFor the status/progression of patients’ disease, a rating was assigned to each patient by the investigator. Ratings were pre-defined as ‘stabilized’, ‘slowing of progression’ (relative to expected decline) or ‘worsening/anticipated decline’, based on the investigators’ knowledge of the natural history of MPS II and accounting for the expected progression of disease over time without treatment. During the interviews, however, it was evident that additional ratings were needed based on the investigators’ responses; these included ratings of ‘improved/improving’, ‘stabilized or slowing progression’ and ‘slowing progression or worsening’.
Investigators’ blinded review of profiles of patients from other study sitesProfiles were selected from 18 patients who had IDS deletions that resulted in large or significant protein or structural loss because it was hypothesized that these variants were more likely to result in severe neuronopathic disease phenotypes [3, 4, 18]. Patient profiles included: (1) age at time of enrollment; (2) DAS-II and VABS-II scores; (3) clinical markers (CSF GAG levels); and (4) anti-drug and neutralizing antibody levels in the serum and CSF. Clinicians rated each patient profile as stabilized, slowing progression (compared with anticipated decline), or worsening/anticipated decline after reviewing the blinded profiles of patients from other sites. Patients from their own site were not included in their blinded set of profiles.
Data analysisFollowing completion of the interviews, RTI Health Solutions identified, characterized and summarized patterns across all interview responses. Dominating trends in each interview were identified and then compared across interviews to collate overall themes and the relative importance of different findings. Descriptive analyses are presented for the overall population and for participants under 6 years of age stratified by IDS genotype (missense versus other variant types), to align with post hoc subgroup analyses conducted on data from the main studies [13]. No formal statistical analyses were performed.
留言 (0)