Study design and population
Unselected patients hospitalized with COVID-19 between February 2020 and June 2020 were included in Patient-Related Outcomes and Lung Function after Hospitalization for COVID-19 (PROLUN), a prospective multi-center cohort study at six major hospitals in Norway [17,18,19]. Inclusion criteria were age > 18 years, admission lasting for ≥ 8 h with a diagnosis of COVID-19, or a positive SARS-CoV-2 PCR test combined with viral pneumonia. All included patients were invited to a follow-up visit approximately 3 months (median 102 days) and 12 months (median 387 days) after their index hospitalization. The follow-up visits were performed by dedicated study personnel at each study center from June 1 to August 28, 2020 (3 months visit) and from February 26 to June 29, 2021 (12 months visit).
A subgroup of PROLUN participants was concurrently included in another prospective, observational study (COVID-MECH; NCT04314232) where they were invited to a cardiac magnetic resonance (CMR) examination approximately 6 months (median 175 days) after the COVID-19 hospitalization (between June 24 and November 18, 2020) [20].
Echocardiography
Echocardiographic imaging was performed according to standard guideline recommendations by five experienced operators following a predefined protocol [17, 18]. All images were recorded using Vivid E95 GE. The images were later analyzed by a single investigator to reduce inter-reader variability. Left ventricular (LV) global longitudinal strain and right ventricular (RV) free wall strain were measured with software from GE imaging systems, and measurements are presented in absolute values.
LV hypertrophy was defined as left ventricular mass index (LVMi) > 115 g/m2 for men and > 95 g/m2 for women [21]. Systolic dysfunction was defined as LV global longitudinal strain < 18% and LV ejection fraction < 50% [22]. Diastolic dysfunction was defined as ≥ 2 of 3: Indexed left atrial (LA) volume ≥ 34 ml/m2, lateral E’<10 cm/s or septal E’ <7 cm/s, and E/e’ >14. Impaired RV function was defined as tricuspid annular plane systolic excursion (TAPSE) < 1.8 cm or RV free wall strain < 20% [21].
Cardiovascular magnetic resonance imaging (CMR)
All patients in the COVID-MECH study were invited to the CMR substudy and 58 (45%) completed the examination, as previously described [20]. All CMR examinations were performed at Akershus University Hospital, using a 1.5 Tesla MRI scanner (Achieva; Philips Medical Systems, Best, The Netherlands) [20]. Myocardial scar was defined as the presence of late gadolinium enhancement (LGE) on CMR. LGE was obtained using phase-sensitive inversion recovery LGE imaging after injections of gadoterate meglumine (Clariscan® Gé, GE Healthcare). Minor myocardial scars were defined as the presence of scars without a concomitant reduction in LV ejection fraction (< 50%). Images were captured using 10 mm short-axis slices all through the ventricles, in addition to three long-axis views.
Blood sampling and troponin measurements
Blood samples were collected and analyzed at several time points during the index hospitalization, and peak hs-cTnT was defined as the highest concentration recorded during the hospital stay. hs-cTnT was also measured in blood samples drawn at the visits 3 and 12 months after discharge. Blood samples were centrifuged at 4 °C, and the plasma was frozen and stored at each study site. At all locations, the analysis of cTnT was performed on a Cobas e801 platform with the high-sensitivity assay (cTnT hs STAT, Roche Diagnostics, Penzberg, Germany), except Trondheim University Hospital where it was analyzed on Cobas e602. This assay has an analytical range from 3 to 10 000 ng/L, a limit of detection (LoD) of 3 ng/L, and the upper reference limit (99th percentile in the general population) is 14 ng/L on both platforms [23]. Following the recommendations of the International Federation of Clinical Chemistry and Laboratory Medicine (IFCC), hs-cTnT values are reported in whole numbers.
We used a hs-cTnT threshold of 5 ng/L to stratify patients. This was adopted from the recommended cut-off used to rule myocardial infarction in suspected acute coronary syndrome, as recommended in the current European Society of Cardiology Guidelines [24].
Assessment of dyspnea
Dyspnea was classified by the modified Medical Research Council (mMRC) dyspnea scale at the 3- and 12-month visits. The mMRC is a self-rating tool to measure the degree of disability that breathlessness poses on day-to-day activities on a scale from 0 (no dyspnea) to 4 (maximum dyspnea) [25]. We performed separate analyses with dyspnea defined as mMRC ≥ 1 (i.e. ‘dyspnea when hurrying or walking up a slight hill’) and mMRC ≥ 2 (‘Walks slower than people of the same age because of dyspnea or has to stop for breath when walking at own pace’).
Sub-group analysis
In an attempt to study troponin in relation to disease severity, we stratified the patients based on whether they had been treated in the intensive care unit (ICU; with or without respiratory support) or admitted to the medical ward. Admission to the ICU was determined based on clinical assessment in the emergency department. ICU stay was registered retrospectively after inclusion in the study through review of the medical records.
We defined the severity of the COVID-19 infection based on whether the patient received treatment in the ICU (severe infection) or not (moderate infection).
Statistical analysis
Continuous variables are presented as means ± standard deviation (SD). Since hs-cTnT is not normally distributed we used geometric mean (95% CI) to describe the distribution of concentrations. All other variables were investigated with histograms and found to be normally distributed, except creatinine which is presented as median (25th -75th percentile). Categorical variables are presented as absolute numbers and percentages. Groups were compared using the t-test, chi-square test, or Fisher’s exact test, as appropriate. Delta values for change in variables from 3 to 12 months were generated by subtraction of the first value from the last value. Patients were categorized according to hs-cTnT levels above or below 5 ng/L and compared using logistic regression in univariable and multivariable models including age, sex, and a history of cardiovascular disease. Log-transformed hs-cTnT concentrations were also analyzed as a continuous variable in multivariable linear regression models with effect estimates and 95% CI. Patients with hs-cTnT below the LoD (< 3 ng/L) were assigned the value of 1.5 ng/L for analytical purposes. Changes in hs-cTnT from hospitalization to 3 months and 12 months were analyzed by the Wilcoxon signed-rank test for paired samples. Comparisons between groups were determined using the Mann-Whitney U test.
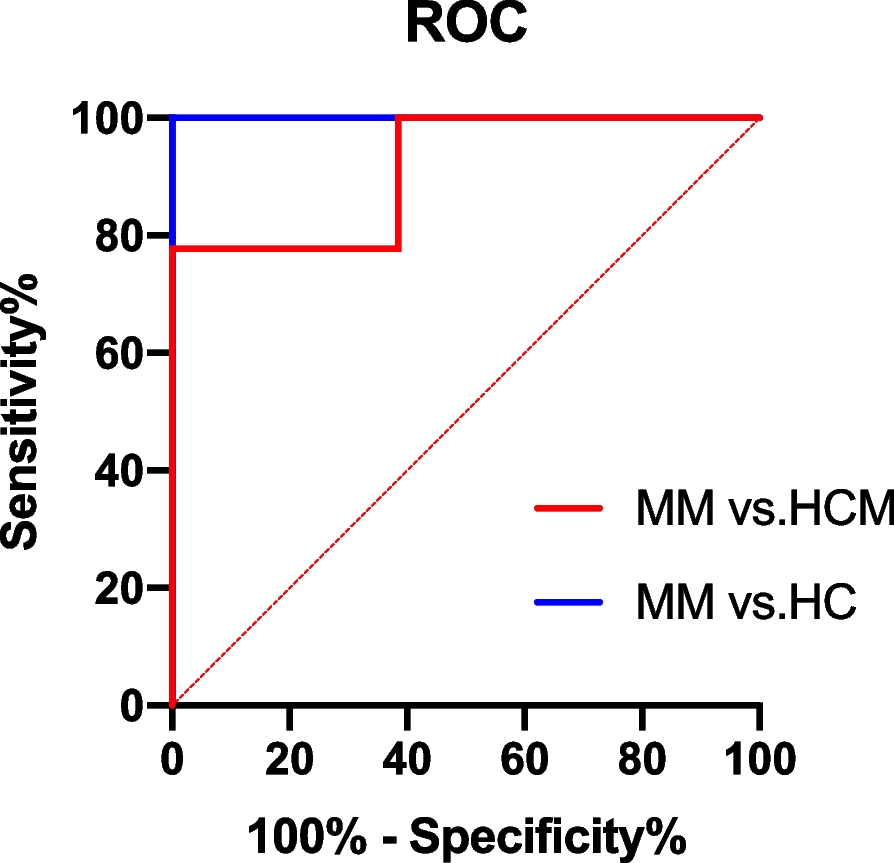
We calculated the receiver operating characteristic area under the curve (ROC AUC) for hs-cTnT, and sensitivity, specificity, negative predictive (NPV), positive predictive value (PPV) and Likelihood ratio (LR) for the performance of hs-cTnT in detecting cardiac pathology when using a cut-off of 5 ng/L. We performed this analysis separately for participants with and without persistent dyspnea 3 months after COVID-19, defined as mMRC ≥ 1 and ≥ 2 in separate models. Statistics were performed using Stata version 16.1. P-values are 2-sided, and values less than 0.05 are considered significant.









留言 (0)