This study was conducted to identify the factors associated with extraocular muscle enlargement in patients with TED. To this end, the effects of age, sex, smoking history, TSH, thyroid hormone, TRAb, TSAb, ATPO, and ATG on the muscle thicknesses of 10 extraocular muscles and the number of enlarged muscles was investigated by use of MRI. Age and TSAb were found to be significantly associated with the total extraocular muscle thickness and number of enlarged muscles, respectively.
Diplopia and compressive optic neuropathy are significant symptoms of TED that occur because of extraocular muscle enlargement. TED is thought to be an autoimmune disorder in which the autoantigen acts on the TSH receptors of CD34-positive fibroblasts in the orbital tissue [17,18,19,20]. Activated fibroblasts and lymphocytes infiltrating the orbit produce cytokines. In addition, activated fibroblasts produce glycosaminoglycans, such as hyaluronic acid, and are presumed to cause inflammatory hypertrophy and fibrosis in extraocular muscles and retrobulbar tissues. However, the mechanism of extraocular enlargement remains unclear owing to the difficulty in obtaining extraocular muscle tissue, treatment-induced alterations in the tissue, and the lack of a useful animal model of TED. A previous study on extraocular muscles revealed infiltration of lymphocytes and plasma cells and deposition of glycosaminoglycans [21]. The lymphocytes were mainly CD4-positive T lymphocytes, which have been reported to produce various cytokines, such as interleukin-4 [22]. Therefore, the present study focused on the factors associated with extraocular muscle enlargement in patients with TED.
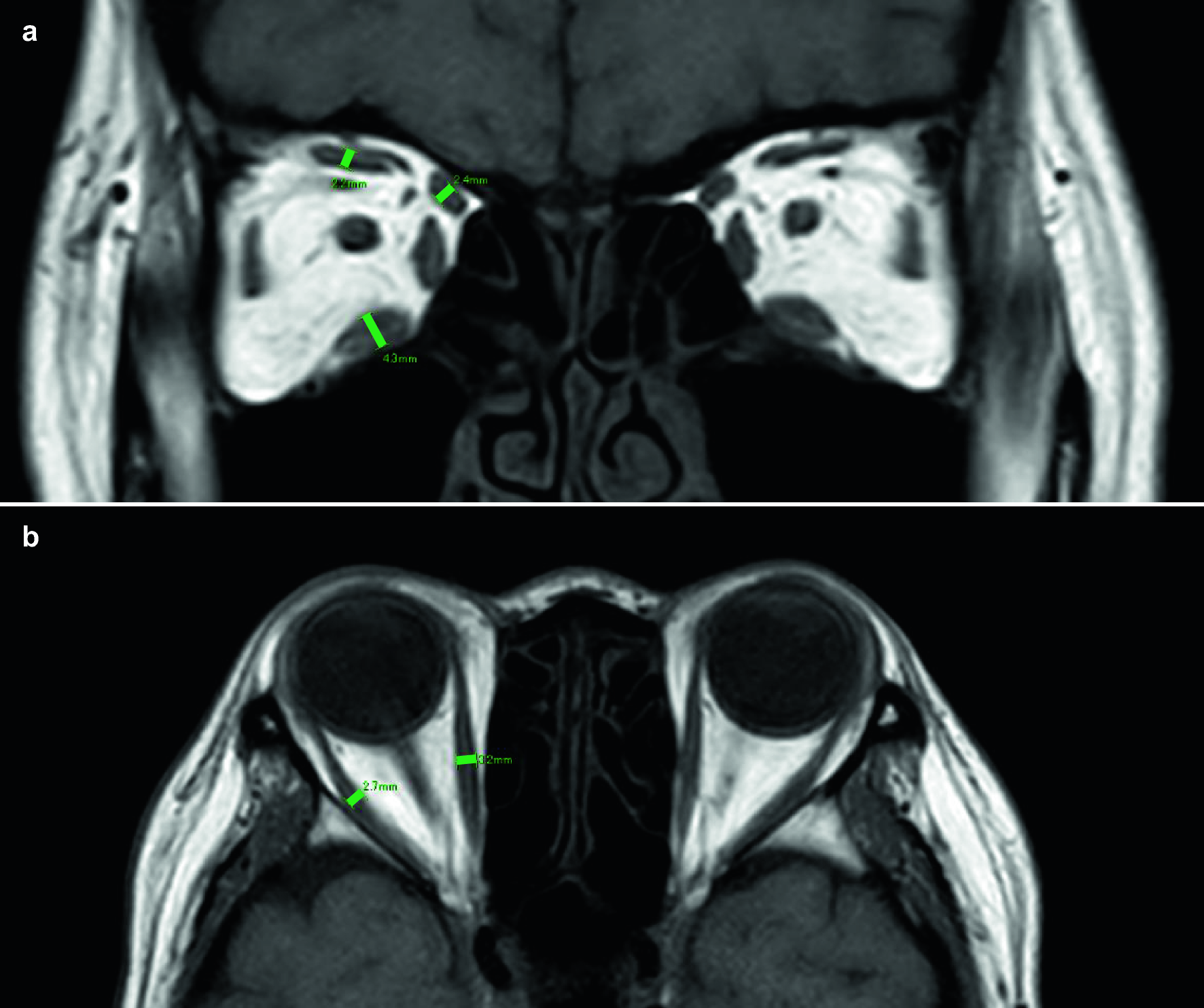
Various methods are available for evaluating extraocular muscle enlargement by use of MRI and CT images, such as measurements of muscle volume, cross-sectional area, and muscle thickness [15, 23,24,25,26,27,28,29,30]. The muscle thickness was measured and examined in the present study [15, 29, 30]. The thickness of the extraocular muscles varies from person to person, making it difficult to identify pathologic enlargement of the muscles. Therefore, the mean+2 SD thickness of each muscle in the control group was used as a cutoff point to determine muscle enlargement [15]. In the present study, the IR was the most frequently affected muscle, followed by the SR and MR, which were affected almost equally. The IR and MR are the most commonly affected muscles in TED. However, reports have been published of the SR being affected more frequently than the MR [23,24,25,26,27].
Previous studies have assessed the presence or absence of diplopia in patients by using TRAb, TSAb, and the CAS and NOSPECS classification [3,4,5,6,7]. However, these studies mainly assessed the association between the clinical scores and autoantibodies. Moreover, these studies did not determine the number of extraocular muscles or the muscle enlargement quantitatively by measuring the thickness. Few reports have assessed the association between autoantibodies and muscle enlargement [8,9,10]. Kvetny and colleagues [8] analyzed the association of MR volume measured by using MRI with TRAb, ATPO, TSH, and thyroid hormone. A correlation was found between the MR volume and TRAb, but not ATPO, TSH, and thyroid hormone. The association of TSAb with MR volume was not investigated. Hiromatsu and colleagues [9] investigated the association between TSAb measured using CHO cells and the 4 rectus muscles using MRI and reported no correlation with the area and number of enlarged muscles. However, an association was observed with the signal intensity of the MRI. A detailed description of the method was not provided. Therefore, whether the area of the enlarged muscle was the sum of the 4 muscles remains unclear; the muscle targeted by the signal intensity is not known. In addition, the association between TRAb and muscle enlargement was not investigated. Choi and colleagues [10] categorized 65 cases of TED with extraocular muscle restriction due to muscle enlargement into improved (32 cases) and not-improved (33 cases) groups. Examination of the factors that affect eye movement restriction revealed that a significant difference was only observed in the TSAb level. In other words, the TSAb level before treatment was lower in the improvement group than that in the non-improvement group. Thus, they concluded that TSAb was superior to TRAb for evaluating restrictive myopathy. In the present study, the thicknesses of a total of 10 extraocular muscles (4 rectus muscles and superior oblique muscles on both sides) were measured by use of MRI images. The association between 2 indices of extraocular myomegaly, the total muscle thickness and number of enlarged muscles, and 4 autoantibodies and thyroid hormones were investigated. To the best of our knowledge, no such a study has been conducted previously. The findings of the present study show that among the 4 autoantibodies, only TSAb was significantly associated with extraocular muscle enlargement.
The symptoms of TED tended to differ according to age, and muscle enlargement is said to be common in patients aged 60 years or older [1]. This study evaluated the association of the total muscle thickness and number of enlarged muscles with age, sex, smoking history, TSH, thyroid hormone, and autoantibody levels and found significant associations with TSAb and age. However, no correlation was observed between age and TSAb. The causes of the variations in the TED phenotype according to age are unclear. Kazim and colleagues [31] reported that the fibroblasts of young patients with TED are prone to adipogenic differentiation. However, the adipogenic potential decreases with aging, and nonadipogenic fibroblasts are predominant in older patients with TED, which promotes inflammation and fibrosis.
Although most cases of TED are bilateral, unilateral cases and cases of laterality have been reported [1, 11,12,13,14], leading to a delay in TED diagnosis. The pathophysiology of unilateral and asymmetric cases is unknown. However, some studies have shown that the activity and severity of asymmetric or unilateral cases are higher than those of symmetric or bilateral cases [11,12,13], whereas some reports have shown no such differences [14]. In the present study, extraocular muscle enlargement was more common in bilateral cases than in unilateral cases. Similarly, extraocular muscle enlargement was more common in asymmetric cases than in symmetric cases. This study investigated the association of age and TSAb with bilateral/unilateral and symmetric/asymmetric muscle enlargement. However, no significant association was found. Unilateral cases may progress to bilateral involvement [32]. Therefore, further research must be conducted on the pathogenesis of unilateral and asymmetric TED.
Several studies have attempted to identify which of the 2 thyroid antibodies, TSAb and TRAb, is the superior biomarker for TED. However, the results have been inconsistent [2]. TRAb levels are measured by use of a competition immunoassay, which can detect its ability to compete with a labeled ligand (a monoclonal antibody to TSH receptor) for binding with the TSH receptor. In contrast, TSAb levels are measured by use of a bioassay, which can measure the production of cAMP using porcine thyroid cells with TSH receptors. The results of the TRAb analysis can be obtained within the same day at a hospital facility. In contrast, 5 to 7 days are required to obtain the results of the TSAb test because it is an outsourced test. Extraocular muscle enlargement has been observed on the MR images of patients with Graves disease who had no clinical ocular signs and symptoms may present [33]. TED with normal thyroid hormone levels (euthyroid Graves disease) is a rare entity. However, its incidence has been reported [34]. Thus, measuring the autoantibody levels, to ensure that the diagnosis of TED is not overlooked, is important. Although internists first measure TRAb, for which results are readily available, the findings of this study suggest that the primary measurement of TSAb is important for early detection and treatment of extraocular muscle enlargement in patients with TED.
This study has some limitations. First, it was a retrospective study with a small sample size. Second, this study did not consider the history of treatment for thyroid dysfunction. Owing to the small sample size, examining the effect of the presence or absence of treatment history for thyroid dysfunction separately was not possible. Third, this study evaluated extraocular muscle enlargement by use of MRI. The volume, cross- sectional area, and signal intensity, rather than the thickness, should have been measured to determine the activity to further evaluate the pathophysiology of extraocular muscle enlargement. However, measuring the volume and signal intensity of the images taken in this retrospective study was technically difficult. Further prospective studies with larger sample sizes must be conducted in the future.
In conclusion, the factors associated with extraocular muscle enlargement in patients with TED were older age and higher TSAb levels. Measurement of TSAb, rather than of TRAb, may be more suitable for diagnosing muscle enlargement in patients with TED.




留言 (0)