
記住我





The survey link was opened on 2511 instances, yielding 1970 complete responses, 1413 (73%) of them meeting the definition of SR. We excluded 85 (6%) responses completed by adult subjects who had suffered from SR in their childhood. The analysis included 1328 parental responses, with 1274 (96%) by mothers. We assessed the relevance of our definition of SR: among the 1328 responses included, 99% children displayed at least one criterion that distinguishes SR from other SAPs (i.e., anxiety, panic attacks). Genders were equally distributed (49% female). At the time of questionnaire completion, mean subject age was 14.7 ± 3.2 years, 887 subjects (67%) had partnered or married parents, and 907 (69%) lived with both parents at the time of SAP onset. Parents’ education level was higher than the national average: 679 (51%) had a diploma equivalent or more than 2 years of post-graduate study, compared to 22% in the general French population, ages 25–64 [22]. Most families (n = 1231, 93%) only spoke French at home.
Mean age of SR onset was 13 ± 4 years. During the two years preceding onset, 323 children (24%) had experienced serious illness or the death of a loved one, 311 (23%) a change of school, 213 (16%) a move, and 157 (12%) a change in family organization. Additionally, 823 (62%) experienced some form of pressure from school, their parents, and/or themselves, 634 (48%) been victims of bullying, insults, or threats, and 206 (16%) of physical violence. Prodromal presentations such as oppositional, depressive, anxious, or somatic symptoms were first evident upon or in anticipation of attending school, at a mean age of 8 ± 4 years. 730 (56%) children had taken an IQ test, and 575 (44%) were gifted children (IQ ≥ 130). Risky screen use was reported by 691 participants (52%). SR was associated with at least one other diagnosis among 1,167 children (88%). The most frequent conditions were depression (n = 425, 33%) and social phobia (n = 367, 28%). See Table 1 for further details.
Table 1 School refusal characteristics in the survey sample (n = 1328)Regarding school adaptations, 759 children (61%) had adjusted school schedules (such as reduced timetables or personal support plans), and 354 parents (27%) felt rejected or criticized by school professionals. Half of the children (n = 681, 54%) received at least one pharmacological treatment, and for 546 (44%), the first health professional consulted was their family doctor. Half of the families spent more than 150 euros/month in non-reimbursed care (min ≤ med ≤ max: 0 ≤ 150 ≤ 3000), and 912 (69%) parents adjusted their work schedules to adapt to their child’s SR.
Trajectories of school refusal during the first three years after onsetRetrospective recall of school attendance during the first three years after SR onset was provided for 729 (55%) subjects. Individual trajectories of SR during this time are represented in Supplementary Fig. 1 using dendrograms, tree diagrams depicting taxonomic relationships. Absences of less than two weeks or between two weeks and one month were observed among 211 (29%) and 175 (24%) children during the second and third year after SR onset, respectively. Complete return to school and return to school with discomfort were observed among 124 (17%) and 146 (20%) children during the second and third years, respectively.
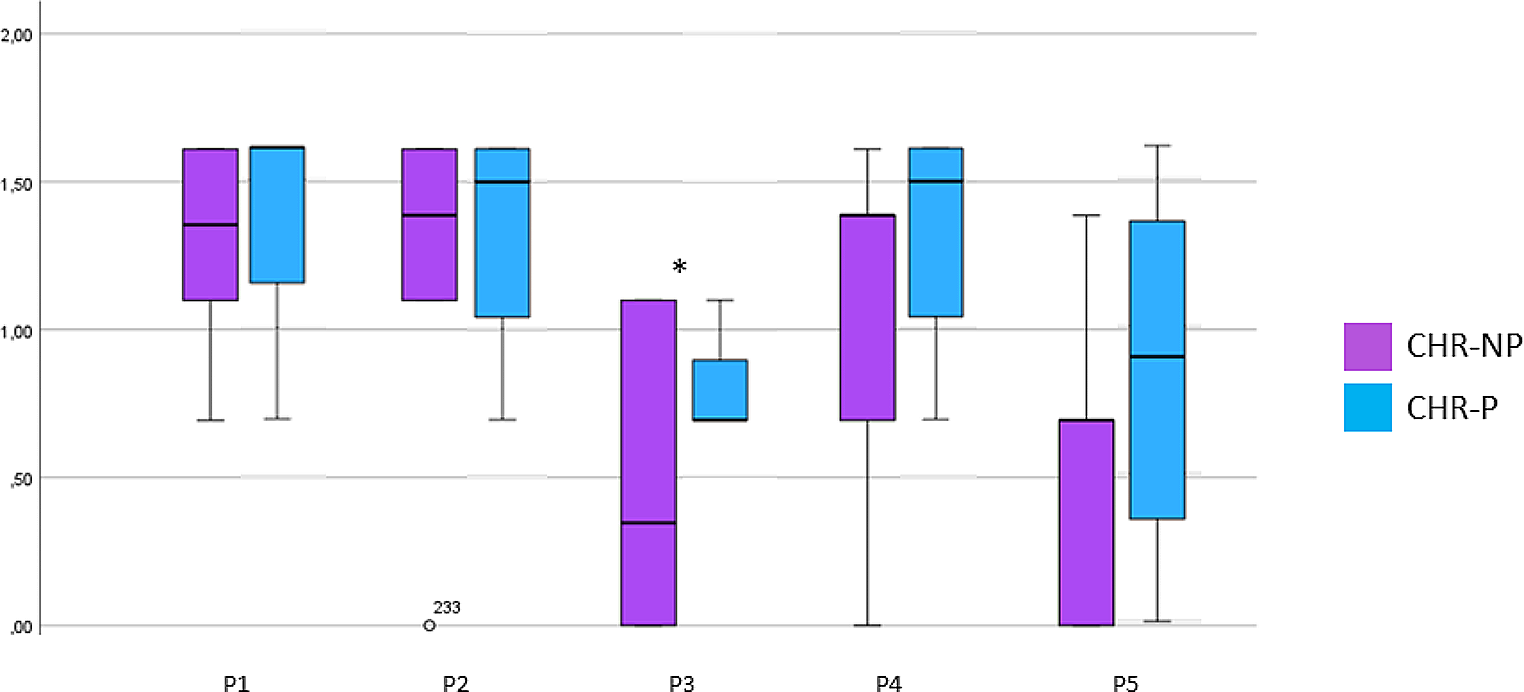
We set the optimal number of clusters at five, following the optimal matching algorithm (Supplementary Fig. 2). An HC of 0.1 confirmed the robustness of fit for these five clusters. Children’s individual trajectories of SR according to each cluster are depicted in Fig. 1.
Fig. 1
Five trajectories of school refusal during the first three years after onset
Characteristics of five SR trajectory clustersTable 2 shows socio-demographic characteristics, SR characteristics, associated diagnoses, characteristics of care and school flexibility across the five clusters. Age of onset was lower in Clusters 1 and 2, “children,” than in clusters 3, 4, and 5 “adolescents” (p < 0.001).
Table 2 Sample characteristics, clinical care, and school flexibility across five school refusal trajectories (n = 729)Clusters 1 and 2: young childrenThe average age of onset for children in clusters 1 and 2 was respectively 9 ± 3 years and 10 ± 3 years, the youngest clusters in this study (p < 0.001). These children were more likely to have a diagnosis of learning disabilities (OR = 1.78, p < 0.001) than participants in clusters 3, 4 and 5. They were less likely to receive follow-up by a psychiatrist or a child psychiatrist (p < 0.001), antidepressants (p < 0.001) and multiple psychotropic medications (p < 0.001), than children in clusters 3, 4 and 5.
Cluster 1: beaded absencesThis cluster, the largest (n = 272, representing 37% of all respondents), describes a moderate, stable course over the first three years, with young children presenting with only short-term absences. Almost all children in cluster 1 (n = 267, 98%) had at least one somatic symptom. They were more likely to experience stomachaches (n = 289; 91%, p < 0.001, OR = 2.57) and headaches (n = 189; 70%, p = 0.001, OR = 1.66) than the four other clusters. The latter were more likely to benefit from school accommodations (OR = 1.67, p = 0.001) or a change of school (OR = 1.66, p = 0.001), than children in cluster 1.
Cluster 2: rapid recoveryThis profile encompasses a high proportion of children with existing medical problems who tended to return to school by the second year of follow-up. In this cluster (n = 132), SR was associated with a worsening of preexisting medical conditions more frequently (17%) than in the four other clusters (n = 23, p < 0.001). The three most common preexisting medical conditions were asthma, rare and/or chronic diseases, and digestive problems. Compared to the four other clusters, parents in cluster 2 reported more frequently not having met the education officer (OR = 1.72, p = 0.003) and feeling rejected by the school (n = 54, 41%, OR = 1.71, p = 0.005).
If considered together with cluster 4, participants in cluster 1 and 2 reported higher levels of complaints toward school (OR = 1.83, p < 0.001), teachers (OR = 2.48; p < 0.001), and classmates (OR = 2.56; p < 0.001) than participants in clusters 3 and 5.
Cluster 3, 4, and 5: adolescentsIn clusters 3, 4 and 5, encompassing older children, participants were more likely to receive psychiatric follow-up (OR = 2.16, p < 0.001), a diagnosis of social phobia (OR = 1.87, p < 0.001), antidepressant medication (OR = 2.06, p < 0.001) or multiple medication (OR = 1.8, p < 0.001) than children in clusters 1 and 2. A separation of children from parents was more likely to be suggested for these three clusters (OR = 2.19, p < 0.001) than for participants in clusters 1 and 2.
Cluster 3: prolonged recoveryFor this cluster, SR onset was on average at age 12 ± 3. Children in the four other clusters were more likely to display oppositional behavior than the ones in cluster 3 (OR = 1.92, p = 0.003). Contrary to clusters 4 and 1, children in clusters 2, 3 and 5 were more likely to question their gender identity, although still infrequently (OR = 4.32, p = 0.004). Participants in cluster 3 obtained a formal SR diagnosis more often than other clusters (87%, n = 81, OR = 2.54; p = 0.001) and were more likely to perceive medication as helpful (n = 24, 26%, OR = 2.11, p = 0.005). These children may have benefited from an intensive healthcare response: 35% of them had at least one care appointment per week (n = 33, p = 0.02, cluster comparison = ns) and they were less likely to forego care for financial or organizational reasons (n = 41, 44%, ns).
Cluster 4: gradual declineSR started on average at 11 ± 3 years for the children in this cluster (n = 89, representing 12% of respondents). They maintained partial school attendance during the first two years, followed by cessation during the third. In comparison to the four other clusters, children in this cluster were more frequently angry about going to school (n = 36, 40%, OR = 2.2, p = 0.001), and more likely to express oppositional behavior (n = 52, 58%, OR = 1.78, p = 0.008). As mentioned above, participants in clusters 1, 2 and 4 complained more frequently about their school, teachers, and classmates than children in clusters 3 and 5.
Cluster 5: rapid declineIn this profile, with an age of onset at 12 ± 2 years, school absenteeism persisted despite accommodations and medical monitoring. This cluster was the most likely to report social phobia, 44% (n = 63, OR = 1.88, p = 0.001). Children in this group had an intensive healthcare response. Compared to the four other clusters, participants in this cluster were more likely to receive more than one type of psychotherapy (44%, n = 63, OR = 2.15, p < 0.001), to having been hospitalized in a psychiatry or pediatric unit (38%, n = 54, OR = 1.95, p = 0.001), and to receive antipsychotic prescriptions (10%, n = 15, OR = 3, p = 0.002). This cluster featured the highest frequency of homeschooling, for 38% of participants (n = 55, OR = 2.4, p < 0.001). Among these adolescents, a separation from parents was more likely to be suggested than in the four other clusters (OR = 2.28, p < 0.001).
If considered together, participants in clusters 4 and 5 were more likely to feature homeschooling (OR = 2.75, p < 0.001) and to be subject to judicial or social services report (OR = 2.1, p = 0.001) than children in clusters 1, 2 or 3.
留言 (0)