
記住我

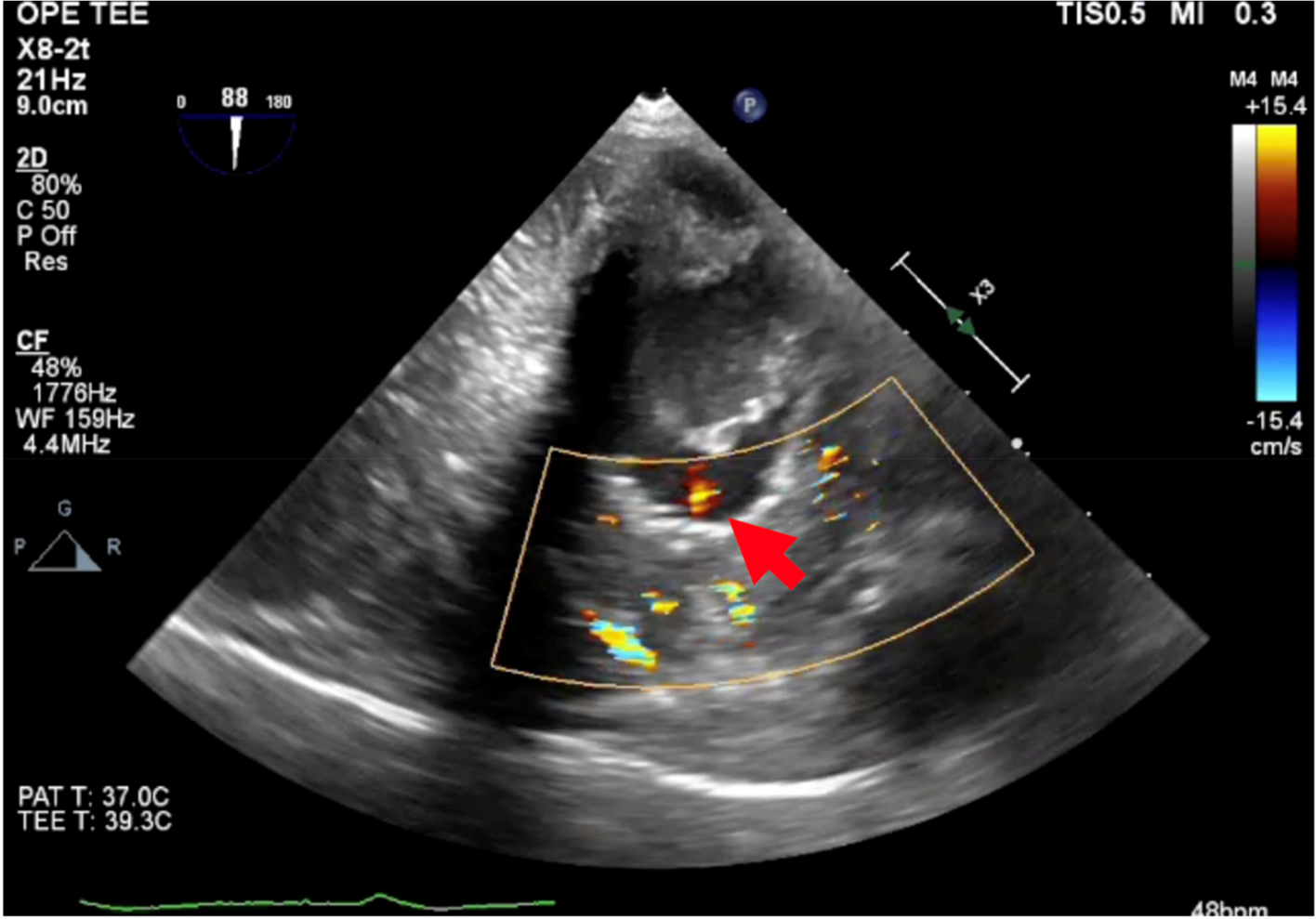
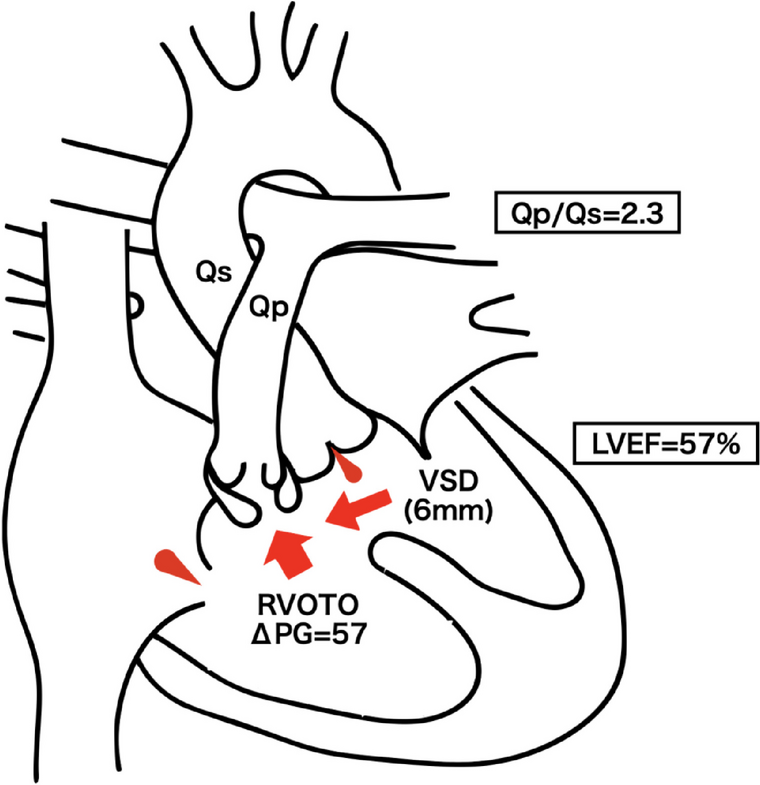


A 72-year-old Japanese man: height, 159 cm; weight, 57.4 kg with bowel obstruction who underwent a laparoscopic right colectomy for ascending colon cancer was reported. The patient was diagnosed with TOF and underwent repair surgery at 19 years of age; however, he had a residual ventricular septal defect and right ventricular outflow tract obstruction. The surgical records from that time are not available and procedure details are unknown. He often experienced paroxysmal atrial flutter, which exacerbated heart failure with dyspnea, and was treated with the angiotensin-converting enzyme inhibitors spironolactone, digoxin, and flecainide for heart failure. Chest radiography revealed mild cardiomegaly, with a 50% cardiothoracic ratio; sinus arrhythmia at 93 beats per minute was observed on electrocardiography. Blood tests showed adequate hemoglobin; 15.4 g/dL, mildly elevated liver enzymes; aspartate aminotransferase, 52 U/L; alanine aminotransferase, 44 U/L, normal coagulation function, and elevated brain natriuretic peptide; 72.6 pg/ml, suggesting heart failure. Renal function was normal, with no electrolyte abnormalities. Echocardiography revealed that the diameter of the residual VSD was approximately 6 mm with left-to-right ventricular shunting; Vmax, 2.8 m/s and mild aortic and tricuspid regurgitation. Left ventricular wall motion was preserved using Simpson’s method with an ejection fraction of 57.3% (Fig. 1). The right ventricular function was slightly reduced, right ventricular fractional area change (RVFAC); 26%, tricuspid annular plane systolic excursion (TAPSE); 18 mm. Preoperative pulmonary artery catheterization revealed a pressure gradient of 57 mmHg between the right ventricle and the pulmonary artery, suggesting residual right ventricular outflow tract obstruction; HR 90 bpm, BP 105/57 mmHg, pulmonary artery pressure (PAP) 28/12 (19) mmHg, right ventricular pressure (RVP) 85/10 mmHg, right atrial pressure (RAP) 10 mmHg, pulmonary capillary wedge pressure (PCWP) 10 mmHg. The Qp/Qs was 2.3 (Fig. 2).
Fig. 1
Schema of heart structure in this patient. LVEF, left ventricular ejection fraction; Qp/Qs, pulmonary-to-systemic blood flow ratio; RVOTO, right ventricular outflow tract obstruction; VSD, ventricular septal defect
Fig. 2
The changes of Qp/Qs. The preoperative Qp/Qs ratio was 2.3. It was reduced to 1.47 after positive pressure ventilation and 1.13 after insufflation. Qp/Qs, pulmonary to systemic blood flow ratio
After inserting an epidural anesthetic catheter and establishing arterial pressure-based cardiac output (FloTrac; Edwards Life Sciences, CA, USA), general anesthesia was induced using midazolam; 3 mg, remifentanil; 0.3 μg/kg/min, rocuronium; 50 mg, following which endotracheal tube and transoesophageal echocardiography (TEE) probe were inserted. We used pressure-regulated volume control ventilation to ventilate the patient with a tidal volume of 500 mL, 10–12 breaths/min, and positive end-expiratory pressure (PEEP) of 5 cmH2O. Noradrenaline and dobutamine were administered continuously to avoid undesirable hypotension. Transient tachycardia with a 2:1 atrial flutter conduction ratio was observed immediately after induction, and the heart rate was controlled with landiolol. General anesthesia was maintained using desflurane. Four milliliters of 0.25% levobupivacaine, 180 ml of 0.25% levobupivacaine, and 20 ml of fentanyl were administered continuously via epidural anesthesia at 4 ml/h. The intraperitoneal pressure was maintained at 10–12 mmHg and was not changed according to pulmonary artery pressure.
Pulmonary artery catheters were inserted through the right internal jugular vein under fluoroscopic guidance. Qp/Qs was calculated using a blood gas analysis of arterial, pulmonary arterial, and mixed venous blood, assuming the oxygen saturation in the pulmonary veins to be 100%. The pressure gradient at the right ventricular outflow tract was 32 mmHg (pulmonary artery pressure, 25/17 mmHg; right ventricular pressure, 57/10 mmHg), and Qp/Qs was 1.47, which was significantly lower than those preoperative values (Fig. 2). After abdominal insufflation, the pulmonary artery pressure increased to 36/20 mmHg; however, the right ventricular pressure also increased slightly, 63/17 mmHg, resulting in a slight decrease in the pressure gradient to 27 mmHg. Qp/Qs further decreased to 1.13 (Fig. 2). The systemic vascular resistance index was 1852 dynes*sec/cm5/M2 after anesthesia induction and 1472–1714 dynes*sec/cm5/M2 after abdominal insufflation.
The dose was adjusted in the range of 0.05–0.2 μg/kg/min of noradrenaline to maintain blood pressure, 1–2 μg/kg/min of dobutamine to assist cardiac contractility, and 1–5 μg/kg/min of landiolol to control heart rate. Intraoperative hemodynamics were stable, with a cardiac index of 2.0–2.5 L/min∙m2 (Table 1). After surgery, the patient was extubated in the operating room. The anesthesia and operation duration were 315 and 215 min, respectively. Blood loss was 310 ml, urine output was 500 ml, infusion volume was 2250 ml, and transfusions were not needed. Continuous epidural anesthesia was administered for postoperative analgesia. The patient had a good postoperative course and was discharged from the intensive care unit on the 4th postoperative day and from the hospital on the 12th day.
Table 1 Hemodynamic parameters
留言 (0)