
記住我



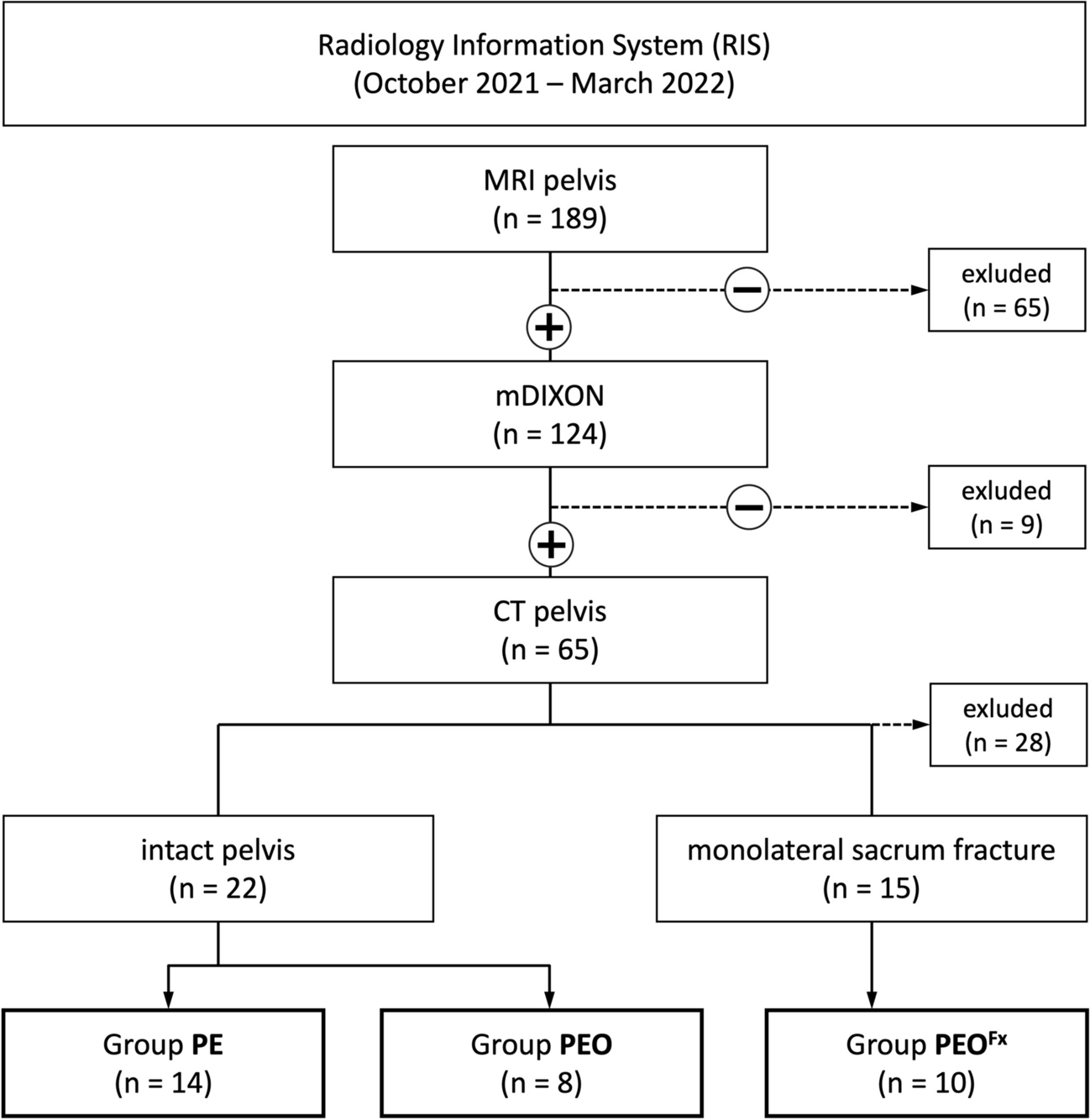
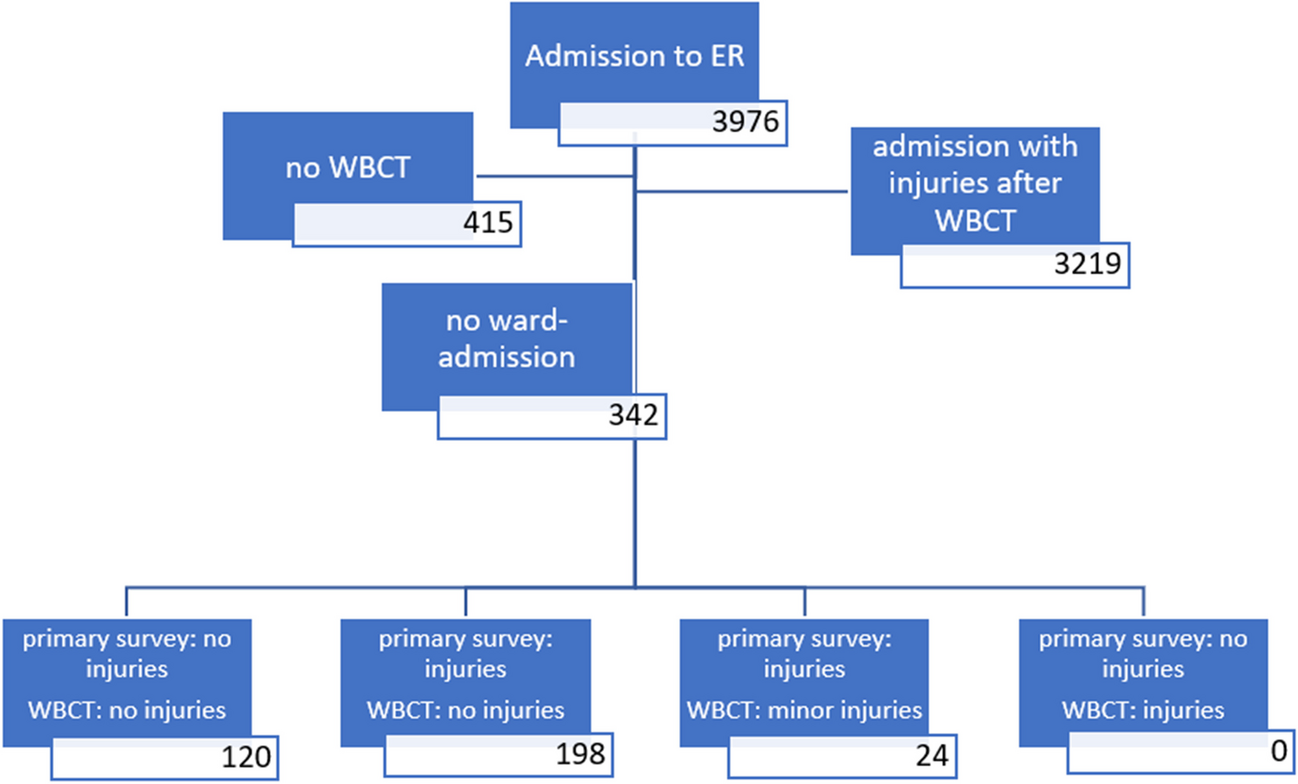
Out of 3932 eligible patients, 1068 met the inclusion criteria. Forty-eight patients (4.5%) had E-bike (E)-related injuries, 740 (69.3%) had bicycle (B)-related injuries, and 280 (26.2%) had motorcycle (M)-related injuries (Fig. 1).
Fig. 1
The E-bike group was significantly older at the time of accident with a mean age of 54.96 (± 16.34) years compared to the bicycle group (42.5 ± 16.69 years) and the motorcycle group (40.19 ± 16.10 years; E vs. B: p < 0.006; E vs. M: p < 0.006). The distribution of age groups (young, adult, elderly) differed significantly between patients using E-bikes and bicycles (p < 0.006) as well as E-bikes and motorcycles (p < 0.006). Elderly people (≥ 60 years) were mostly represented in the E-bike group with 41.7%, less in the bicycle (17.4%) and least in the motorcycle group (11.8%). On the other hand, we observed an overall tendency for young riders to use bicycles (29.6%) and motorcycles (31.4%), with only three young patients using an E-bike (6.2%). Adults were distributed equally among the three groups (E, 52.1%; B, 53.0%; M, 56.8%). The sex distribution showed a predominance of male patients in the motorcycle group (89.3%), whereas sex distribution was more balanced in the bicyclist (male, 69.1%) and E-biker group (male, 64.6%, E vs. M: p < 0.006; E vs. B: p = 0.946). The body mass index (BMI) was highest in patients using the motorcycle (BMI 25.29), followed by E-bikers (BMI 24.83) and bicyclists (BMI 23.65, E vs. B: p = 0.0807; E vs. M: p = 0.816). Helmet usage differed significantly (E vs. B and E vs. M: p < 0.006) among the three vehicle groups with motorcyclists using a helmet in 91.8%, E-bikers in 68.8%, and bicyclists only in 33.8% of cases (Table 1, Fig. 2). Further injury circumstances are presented in the supplements (S1).
Fig. 2 Overview of traumatic craniocerebral injuries
Overview of traumatic craniocerebral injuriesThe mean severity of traumatic brain injuries (TBI) according to the Glasgow Coma Scale (GCS) did not differ significantly between groups (E vs. B: p = 0.419; E vs. M: p = 0.849). Most patients suffered a mild TBI (E, 77.1%; B, 85.7%; M, 73.2%), followed by moderate (E, 14.6%; B, 6.1; M, 10.0%) and severe TBI (E, 4.2%; B, 4.6%; M, 11.1%). However, the median GCS at admission was lower in patients with an E-bike-related injury compared to bicycle injuries without statistical significance after adjustment for multiple testing (GCS: E = 13.27 ± 2.88; B = 14.05 ± 2.27), and was comparable to the motorcycle group (M, 13.16 ± 3.41).
Overall, intracerebral bleeding occurrence (subdural hematoma [SDH], epidural hematoma [EDH], subarachnoid hemorrhage [SAH], and intracerebral hemorrhage [ICH]) did not differ significantly between the three groups (E, 31.2%; B, 21.2%; M, 26.1%); however, the presence of an SDH was significantly higher (E vs. B: p = 0.0107; E vs. M: p = 0.0495) after suffering an E-bike-related traumatic brain injury, with a concomitant significantly higher mean AIS of the SDH. Other intracerebral or cranial injuries such as EDH, SAH, ICH, cerebral edema, diffuse axonal injury, vascular injuries (intracerebral venous sinus injuries, arterial injuries), presence of pneumocephalus, and osseous injuries did not differ between the three groups after adjustment for multiple testing (p > 0.05) (S2, Fig. 3).
Fig. 3
Occurrence of intracranial bleedings for each vehicle type
Influence of helmet usage on craniocerebral injury pattern and severityA subgroup analysis of the influence of helmet usage on the craniocerebral injury pattern and severity was performed for each vehicle class and compared between groups. TBI severity was significantly higher in the E-bike group (p = 0.0007), and the mean GCS was significantly lower (GCS: mean 11.27 vs. 14.18, p = 0.006) in the non-helmet (NH) E-bike subgroup compared to the helmet (H) E-bike subgroup or compared to bicyclists without head protection (TBI: p = 0.006; GCS, 14.0, p < 0.006) at the time of accident (S3). The GCS at admission and severity of TBI of E-bikers wearing a helmet was comparable to cyclists wearing a helmet (TBI: p = 1.0; GCS, 14.18 vs. 13.19, p = 1.0).
Overall, E-bikers without helmet suffered from any kind of intracranial bleeding in 60% of cases compared to 18.2% of patients with head protection (p = 0.0430). This rate is also significantly higher when compared to non-head-protected bicyclists, where intracranial bleedings occurred in 26.0% of cases (p = 0.0405). No difference was observed between head-protected accidents of E-bikers and bicyclists (E/H, 18.2%; B/H, 1.7%; p = 0.787). SDH was the most dominant (60%) and significantly most severe (AIS of 1.87) intracranial bleeding non-helmeted E-bikers suffered compared to helmeted (H) E-bikers (SDH, 9.1%, p = 0.006; AIS 0.27, p < 0.006) and non-helmeted (NH) bicyclist (SDH, 13.0%, p = 0.006; AIS, 0.4, p < 0.006). The occurrence of EDH and SAH did not differ significantly between helmeted and non-helmeted E-bikers after adjustment for multiple comparisons, even though the mean AIS for SAH in non-helmeted E-bikers was greater (p = 0.0208) than in non-helmeted bicyclists (AIS SAH: E = 0.93, B = 0.32). Also, a higher incidence of intracerebral hemorrhage of 46.7% with a mean AIS of 1.4 was present in the non-helmeted E-biker group compared to an incidence of 9.1% with a mean AIS of 0.27 in the helmeted group (ICH: p = 0.0430; AIS: p = 0.0107). Injury incidence and severity were higher in patients of the non-helmeted E-bike group compared to patients of the non-helmeted bicycle group (B/NH, ICH, 13.6%, p = 0.006; AIS, 0.41, p < 0.006). Cranial osseous injuries tended to be more severe in the non-helmeted E-bike group with a mean AIS of 1.2 than in the helmeted E-biker group (AIS, 0.36, p = 0.0813) and more severe than in non-helmeted bicyclists (AIS, 0.59, p = 0.129) but remained non-significant. Overall, craniocerebral injury occurrence and severity of the individual injury (AIS) were higher in the bicyclist group without helmet compared to helmeted bicyclists, which is explained in detail in the supplements (S4).
No significant differences in craniocerebral injury rate and bleeding severities could be found when comparing the non-helmeted and helmeted patients of the E-bike group with their equivalent of the motorcycle group (p > 0.05; S5-6). Motorcyclists without head protection had overall more frequent and more severe intracerebral injuries than patients wearing a helmet. More detailed information is presented in the supplements (S5-6).
Adjusted odds ratios for the occurrence of intracranial bleedings were calculated twofold. The odds ratios for all types of intracranial bleeding dependent on helmet use were adjusted for age (Table 2, Fig. 4). E-bikers without a helmet presented an OR of 6.0 (95% CI, 1.52 to 26.25, p = 0.00124) of suffering any kind of intracranial bleeding compared to bicyclists (OR, 3.29; 95% CI, 2.12 to 5.26, p < 0.00001) and motorcyclists (OR 9.13 95% CI, 3.63 to 25.36, p < 0.00001). Non-helmeted E-bikers presented an OR of 13.86 (95% CI, 2.96 to 85.55, p = 0.0017) for suffering an SDH (B = OR, 4.74; 95% CI, 2.41 to 10.46, p = 0.00003; M = OR, 5.40, 95% CI, 1.85 to 14.90, p = 0.0013). The OR for E-bikers without helmet protection was also significantly higher for SAH and ICH (Table 2). The odds ratios for epidural hematoma could not be calculated for the E-bike group due to little incidence. Age as a factor itself when adjusted to helmet use did not result in a significant finding in the E-bike group. Significant odds ratios for the parameter “Age” when adjusted for helmet use were solely found in the bicycle and motorcycle group but did not reach below an adjusted odds ratio of 0.96 in those cases, which might indicate a minimal clinical relevance despite statistical significance (Table 2).
Table 2 Adjusted odds ratiosFig. 4
Odds ratio for unhelmeted vehicle users to suffer intracranial injures (adjusted for age). Asterisks indicate significantly increased risk of corresponding hemorrhage
Matched pair subgroup analysisA subgroup analysis via propensity score matching for age, sex, and helmet use in between the bike and E-bike group in a 4:1 ratio was performed to confirm the previous findings respective the baseline differences. Matching was successful (S7-8) with no significant differences in between the relevant baseline characteristics. There was also no significant difference in between occurrence of bleedings overall, epidural hematoma, or subarachnoid bleedings. Yet, this analysis confirms the prior findings of a significantly increased occurrence of intracerebral bleedings (B = 8.9% vs. E = 20.8%, p = 0.037) and subdural hematoma in the E-bike compared to the bicycle group (B = 7.6% vs. E = 25.0%, p = 0.002) (Table 3).
Table 3 Matched pair subgroup analysis E-bike vs. bike (1:4 ratio) (matching according to age, helmet usage, and sex)Cervical spine injuriesDifferent accident and injury patterns to the cervical spine were compared in between the vehicle groups. After adjustment for multiple testing, no significance was reached in terms of accident mechanisms as hyperextension/flexion, distraction, distortion, and contusion; there was no difference in between the groups except injuries to the processus transversi when comparing E-bikers and motorcyclists (E = 1.1% vs. M = 0%; p = 0.006). In addition, incidence and severity of spinal cord and osseous injuries on the cervical level did not show significant differences to the bicyclist and motorcycle group (S9).
Craniomaxillofacial injuriesInjury severity in terms of AIS and osseous injuries to the midface were analyzed. Injuries to the facial soft tissue were significantly elevated in the E-biker group compared to motorcyclists (AIS: E = 0.35 vs. M = 0.16, p = 0.011). Further information can be found in the supplements (S0).
OutcomeOutcome parameters defined as ICU admission, rehabilitation, and mortality have been analyzed. Motorcyclists had a significantly higher rate of ICU admission (45.7%) compared to E-bikers (27.1%) which remained not significant after adjustment for multiple testing. Performed rehabilitation showed significant differences (M = 36.4% vs. E = 16.7%, p = 0.0495). Mortality was comparable between all groups (B = 1.9%, E = 2.1%, M = 3.6%) (Table 4).
留言 (0)