Literature review
As expected, case reports from countries in Asia (e.g. Taiwan, Hong Kong, China) demonstrated a markedly higher number of CB suicides as a proportion of total suicides compared to most other countries (Appendix A, Table A.1). In contrast, countries throughout Europe and North America reported significantly lower proportions, ranging from < 1–6% and was highest in the United States (US).
The mean age of decedents was approximately 45 years, and the largest proportion of decedents were male (75–87%). Unfortunately, very few articles reported on the ethnicity of the decedents. Most decedents from the US were “white” (88%) while most decedents from Canada were Asian (92.8%).
Source of CO
Between 2000 and 2019, 4117 suicides occurred in SA. Over this period, 11.5% of all suicides were attributed to CO poisoning (n = 472). For specific CO suicide methods, VE and CB accounted for 10.6% (n = 438) and 0.4% (n = 18) of all suicides in SA respectively.
Among all cases of CO poisoning, 97.6% of VE deaths were suicides (438/449) and 90% of CB deaths were suicides (18/20). However, in cases where the source of CO was either unknown (n = 5) or “other” (n = 28), the proportion of cases that were suicides were 60% and 46.4% respectively (Fig. 1).
Overall, the leading sources of CO toxicity in CO-related suicides were inhalation of VE followed by CB, ‘other’ sources of CO toxicity (n = 13) and cases where the source of CO was unknown (n = 3). ‘Other’ sources of CO included inhaling exhaust from a fuel generator, products of combustion, a CO cylinder, and exhaust from a garden trimmer and collectively comprised less than 3% of all cases. Cases where the source of CO was unknown were confined to the first five years of the study period, influenced by less detailed reporting of scene findings during the earlier years.
While VE was the most common method of CO suicide compared to all other sources, there was a significant, quadratic decrease in the number of VE suicides over the study period indicated by the corresponding dashed line in Fig. 1 (see Appendix A, Table A.2 for full statistical analyses). This decrease was observed to be more rapid in the early years, which began to plateau toward a natural baseline as cases approached zero. The rate of change from year to year can be calculated using the equation:
$$}\,}\,}\,}\,}}\, \times \,}\,}\,}}$$
For example, in 2002 the average number of deaths decreased by 2.12, compared to a decrease of 0.41 deaths in 2014. As illustrated in Fig. 1, the equation above suggests that VE suicides have consistently decreased over time in a parabolic shape, finally reaching a plateau towards the end of the study period. However, the equation should not be used as a prediction tool for future years (i.e. 2020 onwards) as it is unlikely that the trend will continue towards and reach zero but rather follow a more natural pattern of peaks and troughs as is reflected by the raw numbers.
While there were almost no CB suicides in the first 10 years of the study period (0.2 per year average), the rate of deaths increased significantly from 2010 onwards to an average of 1.6 suicides per year as indicated in Fig. 1 by the corresponding dashed lines (p < 0.001, see Appendix A, Table A.3 for full statistical analyses). Using the first 10-year period as a baseline, a Poisson distribution with rate \(\lambda =0.2\), the probability of seeing 2, 3 or 4 deaths in any one year would be 0.017, which is extremely low. In the second 10-year period (2010–2019), 50% of the time case numbers of 2 or greater were observed, providing strong evidence of a significant increase in the rate of CB suicides.
Demographic profile
Most decedents who used CB to commit suicide in SA were male and adults (78% and 72% respectively) (Table 1). For VE suicides, most decedents were also male (83%) and adults (82%). However, compared to CB suicides, there was a greater proportion of elderly persons in the VE cohort (12% compared to 6%). Conversely, a larger proportion of decedents who used CB were young persons (22% compared to 6%). A two-sample t-test showed that the mean age of decedents for CB and VE suicides (37.2 and 45.8 years respectively) was significantly different (p = 0.017), where CB decedents were, on average, between 1.5 and 15.8 years younger than VE decedents (see Appendix A, Table A.4 for full statistical analyses).
Table 1 Decedent characteristics and proximal risk factors for intentional self-harm for CB and VE suicidesDecedents had varied racial profiles compared to studies from the US and Canada [21, 25]. For CB suicides, the majority of decedents in the current study were described as being of Caucasian appearance or “white” (n = 8, 44%). Less than five decedents were reported as being from Asian or African decent, with the ethnicity of the remaining decedents not stated. For VE suicides, most decedents were Caucasian or “white” (n = 324, 74%). Fewer than five decedents were Asian, and ethnicity was not stated in the remaining cases.
Circumstances of death
An analysis of risk factors for CB and VE suicides revealed differences (Table 1). CB suicides were more closely associated with a history of a psychological or psychiatric condition and financial problems compared to VE suicides (72.2% vs. 43.2% and 16.7% vs. 1.8% respectively). However, for VE suicides, there was a larger proportion of cases where the decedent was suffering from some form of physical problem (e.g. cancer, neurodegenerative condition), or where the decedent had contact with the criminal justice system prior to death compared to CB suicides (5.5% vs. 0% and 2.9% vs. 0%).
While there were no cases of CB suicides involving more than one individual, seven cases of VE suicide involved two individuals in various contexts (i.e. murder-suicide, double-suicide etc.). There were several risk factors identified in the histories of the decedents in such cases including deteriorating health and contact with the legal justice system.
Toxicology
The COHb level for CB suicides ranged from 37 to 85% (mean = 69.7%) and from 6 to 98% for VE suicides (mean = 74.4%), yet the difference was not significant (p = 0.25, see Appendix A, Table A.5 for full statistical analysis). However, it is worth noting that the average COHb level for CB suicides where decedents were found in a vehicle (n = 10) was 74.6% which was much closer to the mean COHb level in VE suicides.
Of the 18 CB suicides, only one case was associated with toxicity of other substances in conjunction with CO (i.e. mixed substance toxicity). This case involved the ingestion of several opioid, benzodiazepine and antihistamine sedatives (morphine, codeine, clonazepam, nitrazepam, chlorpheniramine) resulting in additive fatal respiratory depressant effects. The CO level in this case (83%) was not, however, significantly different to other cases.
Of the 438 VE suicides, only 15 (3.4%) were associated with mixed-substance toxicity (Table 2). The mean COHb level in cases attributed to mixed-substance toxicity was markedly lower compared to those attributed to CO toxicity alone (48% and 75.4% respectively). The substances co-implicated in cases of mixed-substance toxicity included various opioid, benzodiazepine and other sedatives with no demonstrable trends between cases. Cases with COHb levels of less than 30% were often seen in combination with significant cardiorespiratory disease (e.g. emphysema, lung carcinoma, coronary artery atherosclerosis) and/or a significantly elevated drug level(s).
Table 2 Toxicology findings for cases of mixed-substance toxicity in VE suicidesFor both CB and VE suicides, there was no correlation between the presence of pre-existing cardiopulmonary disease and death at lower COHb levels. On average, there was only a 1.5% difference in the COHb level between decedents with both cardiovascular and respiratory disease and decedents without any disease.
External examination
There were no significant external findings in cases of CB and VE suicide other than “cherry-red” lividity which was observed in most cases (> 89%, Table 3). Of note, this could be observed for a considerable time after death, up to 32 days for one case. For cases of VE suicide, soot or dirt staining was identified on the hands of 81 decedents (18%) and its absence was only documented in nine cases (2%). However, the presence or absence of soot staining on the hands was not reported in the largest proportion of cases (80%).
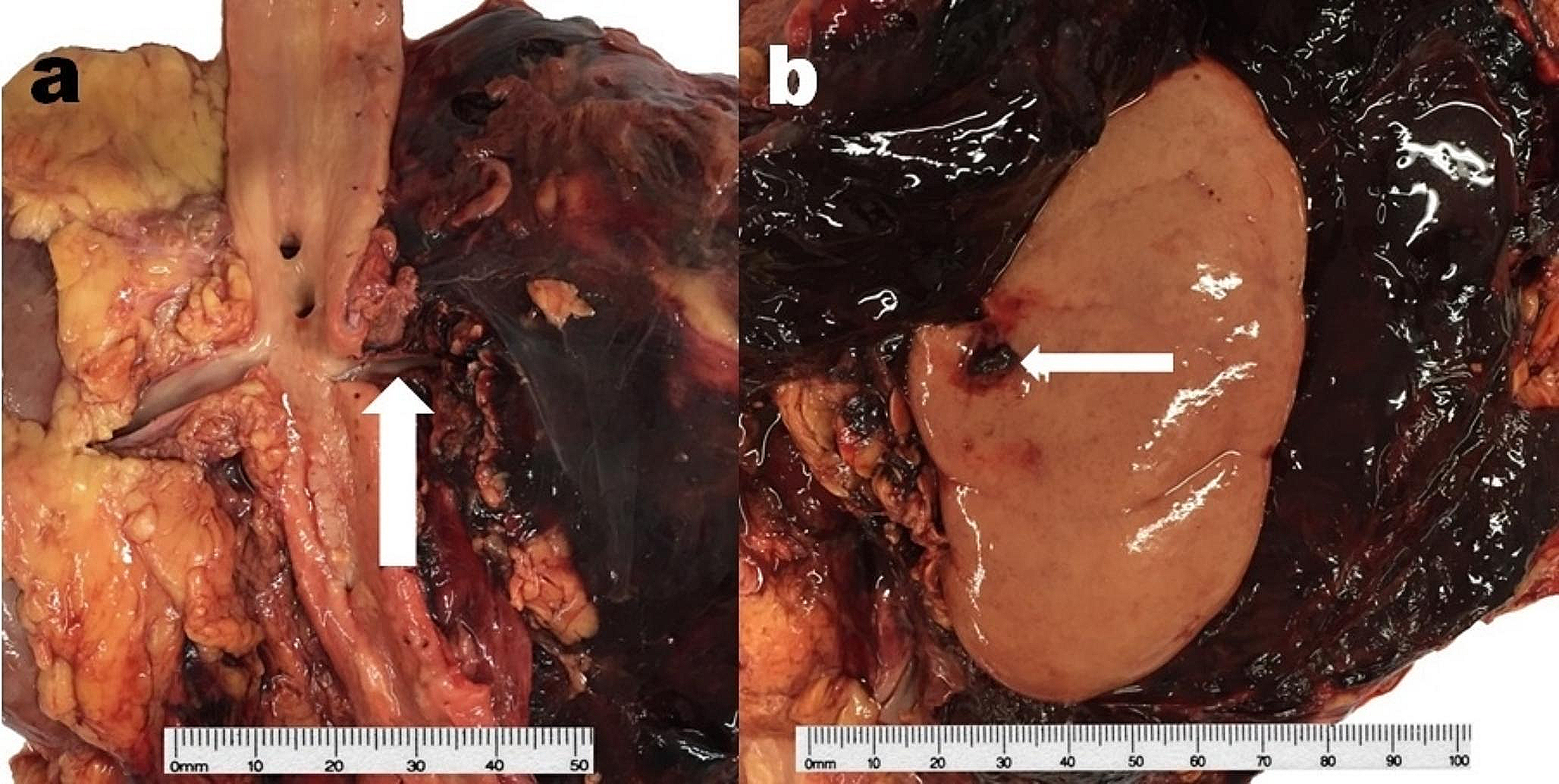
Internal autopsy findings
Internal autopsy findings for CB and VE suicides were also consistent with the literature and are summarized in Table 3. For both methods, pulmonary congestion was consistently observed (> 81% of cases) except for those with marked putrefaction.
Table 3 External and internal autopsy findings for CB and VE suicidesScene findings
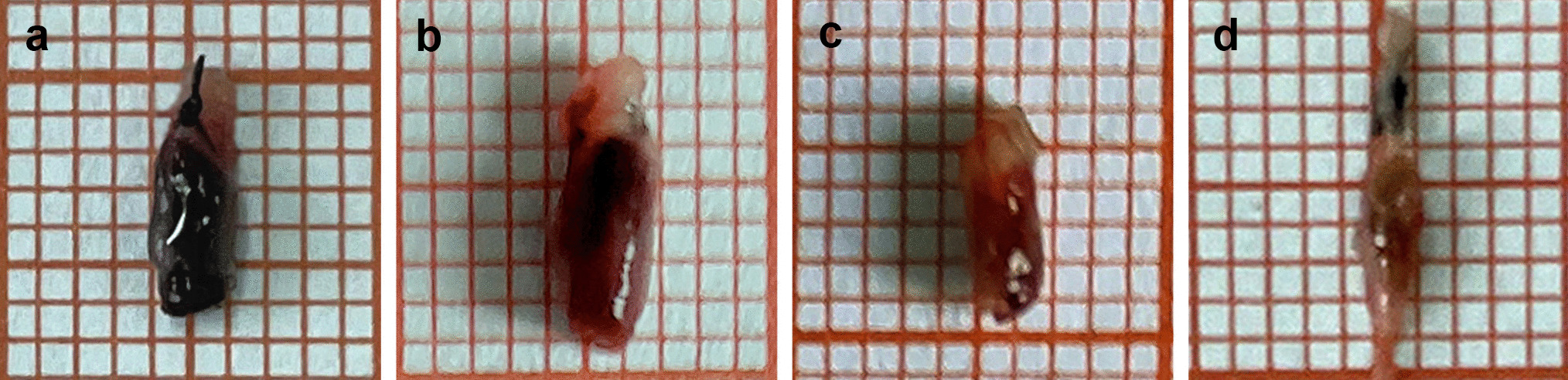
A suicide note was found in 61.1% and 35.8% of cases for CB and VE suicides respectively (Table 1). In all cases of CB suicide, the method used was indicated by burning (or burned) charcoal in some form of BBQ apparatus. More than 50% of CB decedents (n = 10) were found inside a vehicle. The remaining decedents were found in various locations in their homes (e.g. bedroom, bathroom). Conversely, for VE suicides the exhaust of a motor vehicle was diverted either to the interior of a vehicle or into a sealed room using piping.








留言 (0)