While prostate cancer is common in patients >65 years of age, median survival after diagnosis can reach several years to even decades, and patients with PC usually live with tumor for several years after diagnosis [1, 6]. Complications such as hematuria, BOO, urinary retention, bladder stone, and hydronephrosis are common in men with end-stage PC, and up to 20% of advanced PC patients suffer from acute urinary retention (AUR) in their last year of life [24, 25]. Even though patients can choose radiotherapy and androgen blockade, most demonstrate a strong desire to quickly relieve LUTS and improve their QoL. Current approaches include taking α1-blocker monotherapy, intermittent catheterization, suprapubic cystostomy, and pTURP. While α1-blocker monotherapy comes with class-specific adverse events, including postural hypotension, relief of symptoms in patients suffering from BOO due to concomitant PC may be limited. However, long-term intermittent catheterization or suprapubic cystostomy are not capable of significantly improving QoL and are not acceptable for patients. Thus, pTURP for BOO secondary to PC has been adopted by urologists for several decades [5]. However, and to the best of our knowledge, data on treatment of patients suffering from LUTS/BOO and concomitant PC is still scarce [3, 5, 18]. Thus, our patients were offered TURP or HoLEP in addition to guideline-conforming PC treatment [22]. Current guidelines aim to evaluate and recommend different treatment options for LUTS/BOO, and in case of an obstructive prostate recommendation is mainly based on prostate size, and treatment modality (TURP vs HoLEP vs OP) [7]. Since its introduction, HoLEP has shown to be a size-independent method with efficacy and safety even outranking TURP and OP [8, 10, 13, 26]. With recent introductions of different HoLEP techniques, such as the en-bloc enucleation technique, HoLEP challenges OP, especially for larger prostates [15]. However, the increasing number of patients suffering from LUTS/BOO and concomitant prostate cancer prompted us to investigate the feasibility of TURP and HoLEP and its potential benefits in patients with biopsy-proven locally advanced prostate cancer in large propensity score-matched cohorts.
While HoLEP was previously shown to be feasible in patients suffering from BOO secondary to PC [18], there is no current study matching patients for age, prostate size and preoperative IPSS, comparing intraoperative performance, complications, and postoperative outcomes. Primarily, our results show that TURP and HoLEP are both feasible procedures in patients with LUTS/BOO secondary to PC. This is in line with the current, scarce literature [3, 5, 18]. The intraoperative course in both our patient cohorts was uneventful, and a low rate of postoperative complication was observed, not exceeding those so far reported for standard HoLEP [8, 13, 26].
As patients were propensity score-matched, we found no difference in age, IPSS, or prostate volume in the pTURP vs TURP and the HoLEP vs pHoLEP cohort. However, PV was almost two-fold in the HoLEP cohorts. Although the age difference between HoLEP and TURP cohorts was not clinically significant, this may reflect the age-dependency of prostate size observed by various studies before [8, 27]. As this was a retrospective analysis, the aim was not to compare the two procedures, rather patients were selected for HoLEP or TURP based on prostate size, according to the current guidelines on the management of male LUTS, and later compared [21]. Additionally, we found no difference in preoperative Qmax, observed unsatisfying QoL scores of 4 points throughout our patient cohorts, as well as a clinically relevant and equally dissatisfying PVR, without any difference between groups. As anticipated, we observed a significantly higher median PSA in patients with prostate cancer, with concomitant difference in PSA density between groups. However, with larger prostates in the HoLEP cohorts, this difference was not statistically significant, supporting the hypothesis that PSA also correlates with prostate size. Thus, confirming to our previous data [28].
While we observed no significant difference in patients presenting with an ASA score ≥III between groups, with equal numbers of patients presenting with an IDUC prior to surgery in the palliative groups [24, 25]. With >95%, we found significant prostate cancers (Gleason grade ≥7) throughout our PC cohorts. Only few patients had Gleason grade 6 prostate cancers, making them eligible for AS. However, locally advanced, histologically more aggressive tumors may account for LUTS/BOO secondary to PC, corresponding to tumor burden [3, 5].
While there was no significant difference in preoperative hemoglobin value, there was a difference in 24-h postoperative hemoglobin drop between the palliative cohort and the BPH cohort, albeit statistically significant only for the HoLEP procedure. However, there was no need for perioperative blood transfusion, corresponding to the data we gathered on the favorable perioperative safety profile of performing HoLEP in octogenarians [29]. However, angiogenesis is part of the neoplastic process in prostate cancer, and our data reflect the increased challenge of endoscopic LUTS surgery in patients suffering from BOO secondary to PC. To minimize adverse events, many surgeons prefer to perform a channel TURP in patients with PC and LUTS [5]. However, we did not perform channel TURP in PC patients, as evidenced by the amount of resected tissue, with no difference between PC patients and BPH patients. For our HoLEP cohort median hemoglobin drop did not differ from the corresponding TURP or pTURP patients, even though the prostates were twice larger. As prostate hyperplasic growth may be accepted as neoplastic process, involving angiogenesis, our HoLEP data are much more favorable [30]. Laser enucleation of larger glands results in a larger surface of the prostatic fossa, consequently influencing the amount of fluid absorption during HoLEP and increasing the risk of hemodilution over operating time [8, 17, 31]. Thus, hemodilution may well explain the increased – albeit clinically insignificant – blood loss in patients with enlarged prostates.
We report significantly prolonged surgery and enucleation time, for TURP and HoLEP procedures, respectively, comparing the BPH with the PC patient cohorts. This is corroborated by the corresponding efficacy (g/min) values, favoring BPH patients. In TURP procedures this may reflect the increased difficulty operating on PC patients, with markedly more vulnerable prostatic tissue. In HoLEP patients the surgical plain is obviously more challenging to follow in cancerous areas. However, morcellation time did not significantly differ in PC patients, following HoLEP. Considering the one-lobe technique not only circumvents the laborious protocol of repeatedly finding the surgical plane, as once the correct plain is entered, the adenoma is mobilized in an en-bloc fashion, it also prevents the obvious time lost between finding and morcellating three separate lobes versus one single lobe, especially in vulnerable PC tissue [15].
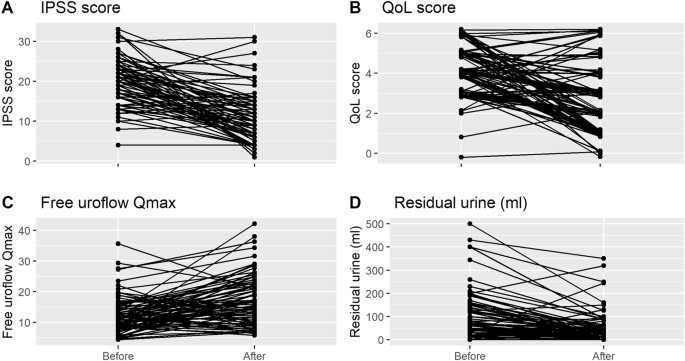
Although surgical efficacy parameters did not significantly differ between our patient cohorts (BPH vs PC), all patients in our study showed improvement of functional outcomes after TURP or HoLEP. There were distinct improvements of IPSS, Qmax, and PVR for all patients in our study with similar improvement throughout groups. There was no statistical difference favoring the BPH patient cohort, making both procedures eligible in PC patients. However, we observed markedly increased postoperative functional parameters in the HoLEP groups, highlighting the clinical benefits of laser enucleation, especially considering the twice enlarged prostates in the HoLEP cohorts. These findings correspond with international literature, and our previous results [8, 13, 15, 26]. Furthermore, QoL improved similarly for all patient cohorts.
Overall, 21 patients suffered a postoperative complication according to the modified CDC. Most of our complications were found to be CDC grade III, with persistent hematuria or clot retention, requiring surgical reintervention as the most common grade III complications. The rate of grade III complications (11.9% for pTURP and 10.4% for pHoLEP) did not significantly outrank those in the BPH cohort, and seems favorable, compared to other reports for pTURP [5, 32], pHoLEP data [3, 18], with postoperative voiding failure in up to 42%, need of repeated TURP in up to 29%, and permanent incontinence in up to 10% [5, 32]. Even though complications were more common in PC patients, there was no statistically significant difference to BPH patients, regarding overall or higher grade (≥II CDC) complications. Even though the risk of hemodilution due to a significantly larger surface of the prostatic fossa in larger glands may be higher, one of the many advantages of HoLEP and bipolar TURP includes using physiologic saline as irrigant. Thus, we found no life-threatening transurethral resection (TUR-) syndrome in our patient cohort. Thus, we report no CDC grade IV or grade V complications among our patient cohort.
Limitations of our study surely include its retrospective design and short post-operative follow-up period. Thus, limiting the power of our conclusion. Following up the patient at a tertiary referral center is problematic, preventing complete collection of data for more cases. However, a longer follow-up is required for complete appraisal of functional outcomes and the safety profile. However, Elshal and colleagues could show no significant difference in short-term (30 days) postoperative functional outcomes compared to follow-up after one year [33]. Taken together, we could show that there are no limitations to using TURP or HoLEP even in patients with PC.
Currently, there is no standard-of-care for patients with LUTS/BOO and locally advanced prostate cancer. However, our results show that TURP and HoLEP are both feasible procedures in patients with LUTS/BOO secondary to PC. HoLEP procedures were performed in patient cohorts with twice larger prostate size, showing that it is a feasible technique in a palliative setting in patients with prostate sizes, in which TURP may no longer be recommended. However, both procedures offer adequate and fast symptom relief with comparable safety profiles. and corresponding efficiency parameters resulting in two-fold higher surgical performance for both techniques in patients without prostate cancer. Taken together, the study covers an important gap in current literature, helping urological surgeons to make evidence-based decisions for the benefit of their patients. Thus, future research should focus on a multicenter approach to facilitate a guidelines recommendation for patients suffering from BOO due to locally advanced prostate cancer.



留言 (0)