
記住我








A 62-year-old woman underwent a series of operations for subarachnoid hemorrhage with a ruptured posterior communicating artery, including coil embolization, decompressive craniectomy, ventriculoperitoneal shunt, and cranioplasty with a titanium mesh (Fig. 1A). Following the operations, the patient was diagnosed with MCS, and her revised coma recovery scale (CRS-r) score was 3 (A0V0M2O0C0Ar1) [3]. One year later due to failure of emergence of MCS, attempts for non-invasive neuromodulation treatment to improve the patient’s level of consciousness were discussed. However, due to the skull defect and titanium implant, conventional neuromodulation with tDCS was not considered a treatment option [4].
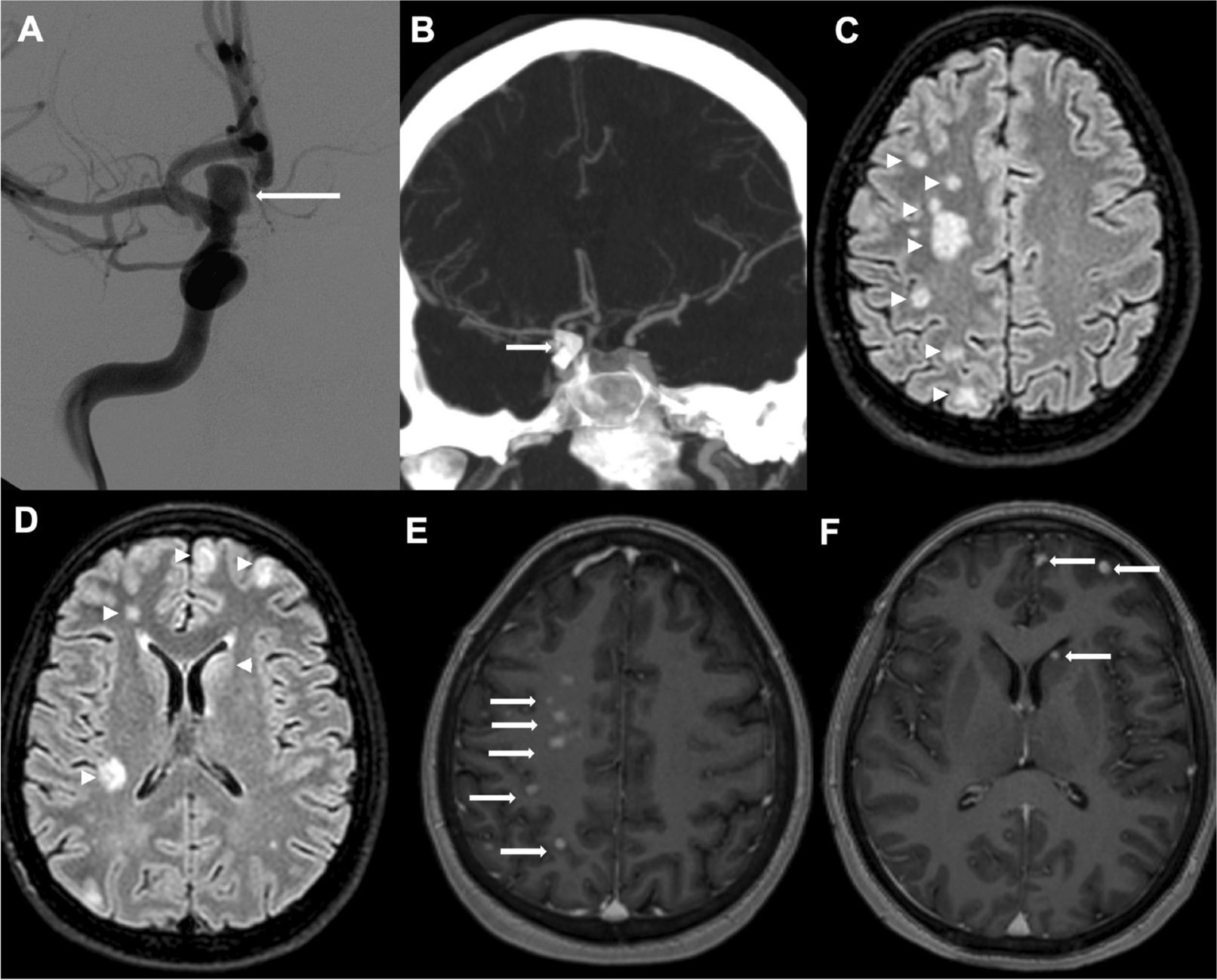
Fig. 1
Simulation and the locations by conventional and optimization for targetting the right dorsolateral prefrontal cortex. The red pad is the cathode, and the blue pad is the anode. A Anteroposterior and lateral plain X-rays. The X-rays demonstrate the titanium mesh covering the left cranium. B The simulation montages used to simulate the effects on cortical current flow from tDCS. C–E Simulation shows that the Enorm field values of the right dorsolateral prefrontal cortex were stimulated by tDCS via three methods. C Simulation via conventional stimulation with 10–20 system. D Simulation via bi-frontal cortex stimulation. E Simulation via optimization based on the patient’s MRI. A, anterior; P, posterior; R, right; and L, left
Under the consensus and agreement from all her legal guardians, she underwent treatment with tDCS to facilitate the dorsolateral prefrontal cortex (DLPFC). We simulated the electric field and locations of stimulation for targeting the right DLFCS via Neurophet®’s TesLab based on the patient’s MRI [5]. The simulation montages and electric field for stimulations with optimization based on 1-mm MRI resolution showed the proper Enorm of the right DLPFC (Fig. 1B–E). Treatment with tDCS was performed according to the following protocol; the cathode and anode were positioned as shown in Fig. 1F. A current intensity of 2 mA and a simulation time of 30 min were applied. Treatment with tDCS was performed according to the following protocol; the cathode and anode were positioned as shown in Fig. 1F. A current intensity of 2 mA and a simulation time of 30 min were applied. The tDCS intervention was performed 10 times for 2 weeks. The patient received in conjunction conventional rehabilitation therapy, such as physical and occupational therapy for 2–4 h per day (5 days per week). The therapies were performed passively, i.e., not in a goal-oriented manner, due to the debilitating nature of DOC. After the patient was treated with ten consecutive optimized tDCS sessions, the follow-up CRS-r score showed improvement to 17 (A2V4M3O3C2Ar1). Two months later, she showed dramatic neurological recovery, underwent successful nasogastric tube weaning, and was able to start full oral feeding. Six months later, she started walking with assistance.
留言 (0)