
記住我





A 69-year-old man was referred to our hospital with acute exacerbation of chronic obstructive pulmonary disease (COPD). Computed tomography revealed pneumonia in the right lower lobe and extralobular sequestration of the left lower lobe. His right lower lobe had a normally bifurcated bronchus and pulmonary arteriovenous system, and part of the lung parenchyma protruded beyond the mediastinum into the left thoracic cavity, in front of the vertebral body (Fig. 1). Abnormal vessels from the descending aorta flowed into the protruding lung. The protruding lung was distinguished from the normal left lower lobe by the pleura and was, therefore, in a state of left lower pulmonary sequestration. The patient was diagnosed with a congenital malformation of the horseshoe lung with pulmonary extralobular sequestration. Although the patient had been treated for pneumonia multiple times before, this was the first time a pulmonary abnormality was noted (Fig. 2). After the treatment was completed, we suggested surgery to remove the malformed lung. However, the patient declined because his symptoms were alleviated with medication. Over the next 2 years, the horseshoe lung repeatedly developed pneumonia. One year later, he was hospitalized for pneumonia, at which time Aspergillus was detected in his sputum for the first time. We determined that he had complicated chronic pulmonary aspergillosis. From this point on, he started taking itraconazole. He then experienced hemoptysis and underwent bronchial artery embolization twice; however, the hemoptysis was not completely cured. After repeated episodes of pneumonia and hemoptysis, his medicine was switched from itraconazole to voriconazole 3 months before the surgery. His pulmonary function gradually deteriorated owing to lung destruction. Home oxygen therapy was initiated 1 year later. Finally, at the age of 71 years, the patient requested surgery after a discussion with medical personnel and was referred to our department.
Fig. 1
A Computed tomography showing the protruding lung from the right to the left side in front of the descending aorta and behind the esophagus (dotted line). B An abnormal blood vessel from the descending aorta to the lung is confirmed (arrow)
Fig. 2
Computed tomography at 5 years (A), 3 years (B), and 1 year (C) before surgery. The horseshoe lung (dotted line) became rough because of repeated infections
At that time, the patient experienced frequent phlegmatic cough, with hemoptysis. He was receiving home oxygen therapy and required 2 L of oxygen at rest and 3 L during exertion. The vital capacity (1.27 L) and forced expiratory volume in 1 s (0.80 L) were measured, both of which were worse than those measured 2 years before. The surgical indication was discussed at a multi-professional conference, and we concluded that the removal of the swollen lung could alleviate the symptoms and improve the respiratory condition; thus, we decided to perform the surgery. One week before the surgery, the patient was hospitalized and underwent respiratory rehabilitation. Blood tests just prior to surgery showed that his white blood cell count was 8500 and CRP, 0.34.
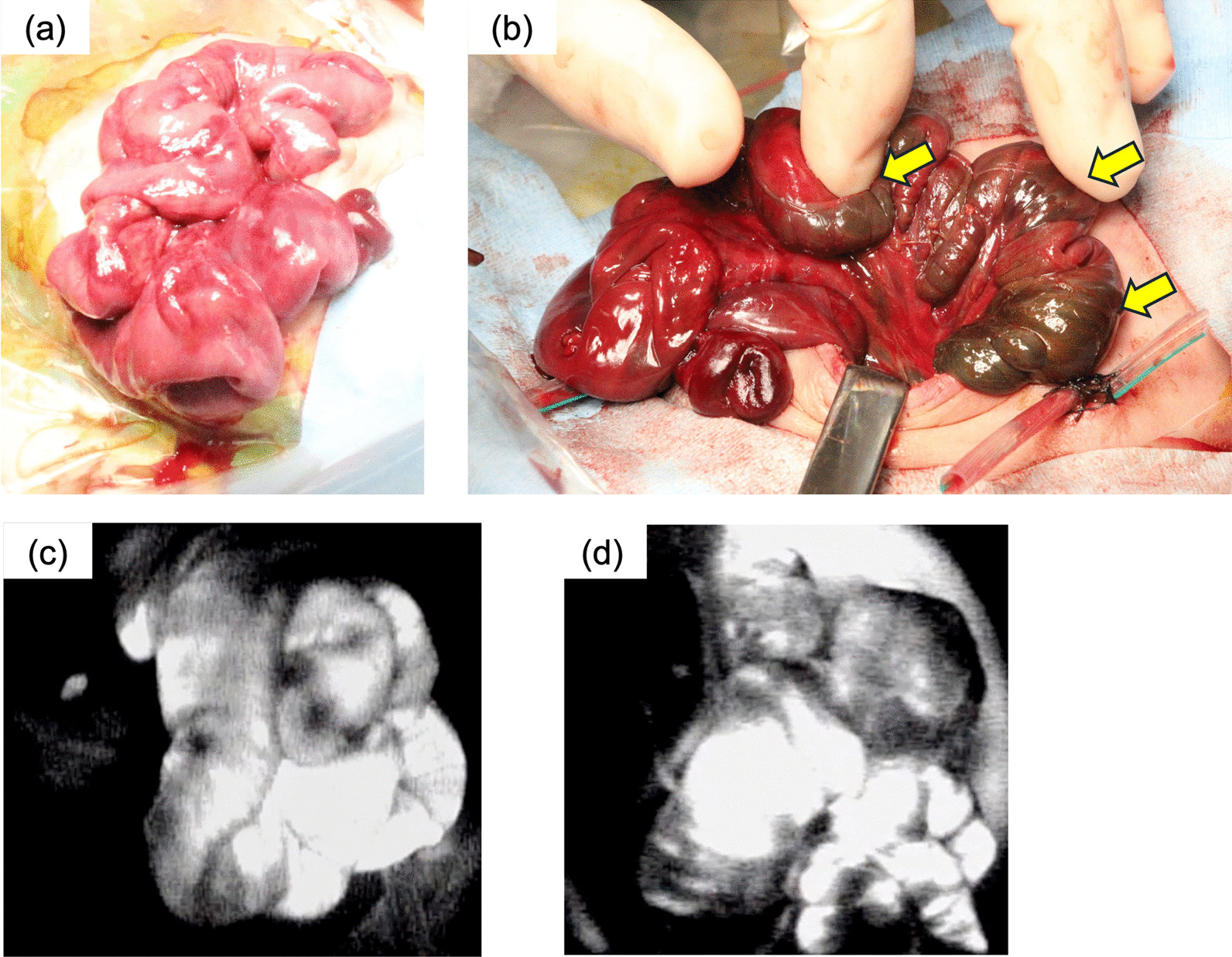
Surgery was performed in the following order: left thoracotomy, followed by right thoracotomy, with posterolateral thoracotomy performed bilaterally (Fig. 3A). From the left thoracic cavity, we observed a normal left lower lobe and extralobular sequestration. There was dense and extensive adhesion; therefore, we carefully detached the extralobular sequestration from the chest wall, normal left lower lung, and diaphragm (Fig. 3B). The sequestration lung extended continuously to the right thoracic cavity between the vertebral body and esophagus. An abnormal blood vessel flowing into the sequestration from the descending aorta was identified from the left thoracic cavity and excised using automatic sutures (Fig. 3C, D). A right lower lobectomy was performed via a right thoracotomy. Although the degree of adhesion was even worse in the right thoracic cavity, we successfully removed the horseshoe lung without breaking the capsule. The operating time was 8 h and 39 min and blood loss was 1600 ml, and he received a blood transfusion (red cell concentrate, 4 units; fresh frozen plasma, 4 units).
Fig. 3
Surgical findings. A Skin incision lines. B From left thoracotomy, we can identify the normal and protruding lung. C Abnormal blood vessels during left thoracotomy. D Removed lung
The patient was extubated on postoperative day (POD) 1, and rehabilitation was initiated. However, he had acute exacerbation of COPD and required a ventilator on POD 9. Aspergillus, which caused empyema, was detected in the right pleural effusion. A right open-window thoracostomy was performed on POD 46. The patient’s respiratory condition improved thereafter, and he was weaned off the ventilator on POD 91. The patient was discharged after thoracostomy on POD 133. Antifungal medications were continued postoperatively.
At the time of discharge, he received home oxygen therapy (1 L at rest and 3 L during exertion). The patient’s oxygen requirements were almost the same as those before admission. The subjective symptoms of bloody sputum improved. He was still able to walk several hundred meters, but his activities of daily living were reduced compared with those before admission. He recovered at home but developed severe pneumonia 4 months later. The patient was hospitalized again and received antibiotics and antifungal drugs. However, despite extensive pneumonia treatment, he died of respiratory failure.
留言 (0)