
記住我
Nowadays, aligners are among the main orthodontic options in both adolescents and adults, as the demand for esthetic orthodontic treatment is growing in both groups of patients.[1-4] Thanks to their esthetic properties and reduced emergency occurrence.[5,6] New aligner materials are in constant research and development,[7] and it is becoming possible to treat ever more complex malocclusions.[6,8] However, aligners still have significant biomechanical limitations that sometimes either preclude their use or oblige the patient to accept very long treatment times.[9,10] Among the least predictable movements are the rotation of conical teeth,[11,12] movements requiring root control,[13,14] and movements on the vertical plane.[15-17] In contrast, the literature agrees that aligners are particularly efficient and efficacious when performing tipping movements.[11,16]
To reconcile the esthetic demands of the patients with the predictability of results, it is now possible to offer hybrid treatments. These combine aligners with auxiliaries (e.g., simple buttons, sectional archwires and/or elastics) or more complex devices depending on the clinical requirements.[18,19]
Due to the biomechanical limitations of aligners,[9,10] one of the most complex cases to resolve using aligners alone is deep bite.[15-17] The literature reports several strategies for aligner-based correction of deep bite. These include the use of anterior bite ramp and vertical elastics to extrude the posterior sectors and overcorrection of the planned movements in the digital setup (i.e., intrusion of the frontal sector) in order to level the Spee curve. Furthermore, horizontal rectangular attachments on the premolars and first molars can be used to increase retention and transmit the necessary force to the teeth.[20,21]
However, as deep-bite correction involves proclination, leveling the Spee curve becomes even more complex when there is little crowding in the lower arch. In such cases, vestibularization of the frontal sector, which would facilitate bite opening,[15] must necessarily be limited in order to avoid opening spaces.
CASE REPORTThe following case report illustrates how innovative hybrid treatments that exploit the potential of both aligners and their setups and the advantages of skeletal anchorage enable the treatment of cases of severe deep bite with predictable outcomes and much reduced treatment times.
DiagnosisA 38-year-old male patient presented with a complaint of discomfort in the upper retroincisal area due to anomalous contact between the margins of the lower incisors and the palatal mucosa. In addition, he was unhappy with his smile esthetics and requested an esthetic treatment that would resolve his functional issues and improve the look of his smile.
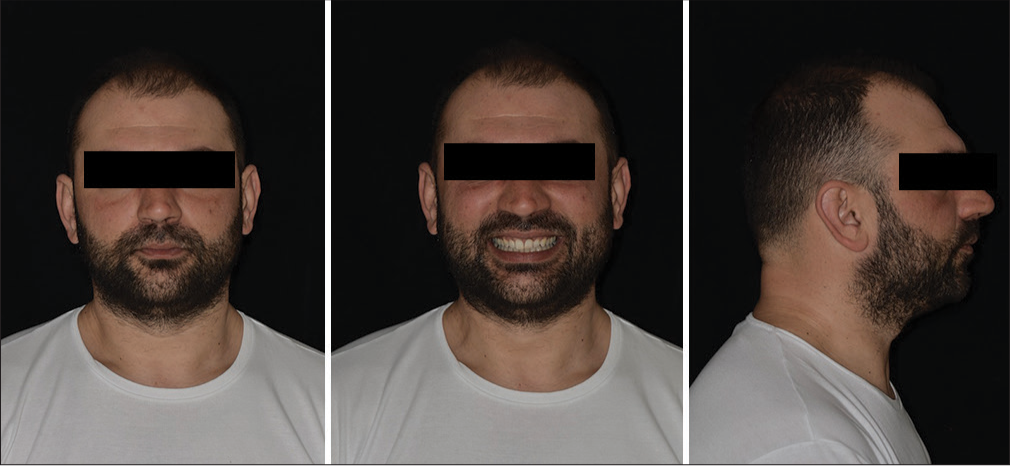
Extraoral examination showed excessive upper incisor exposure and wide buccal corridors. The upper midline appeared correctly centered in the face, but the profile had the convex appearance characteristic of Class II malocclusion [Figure 1].

Export to PPT
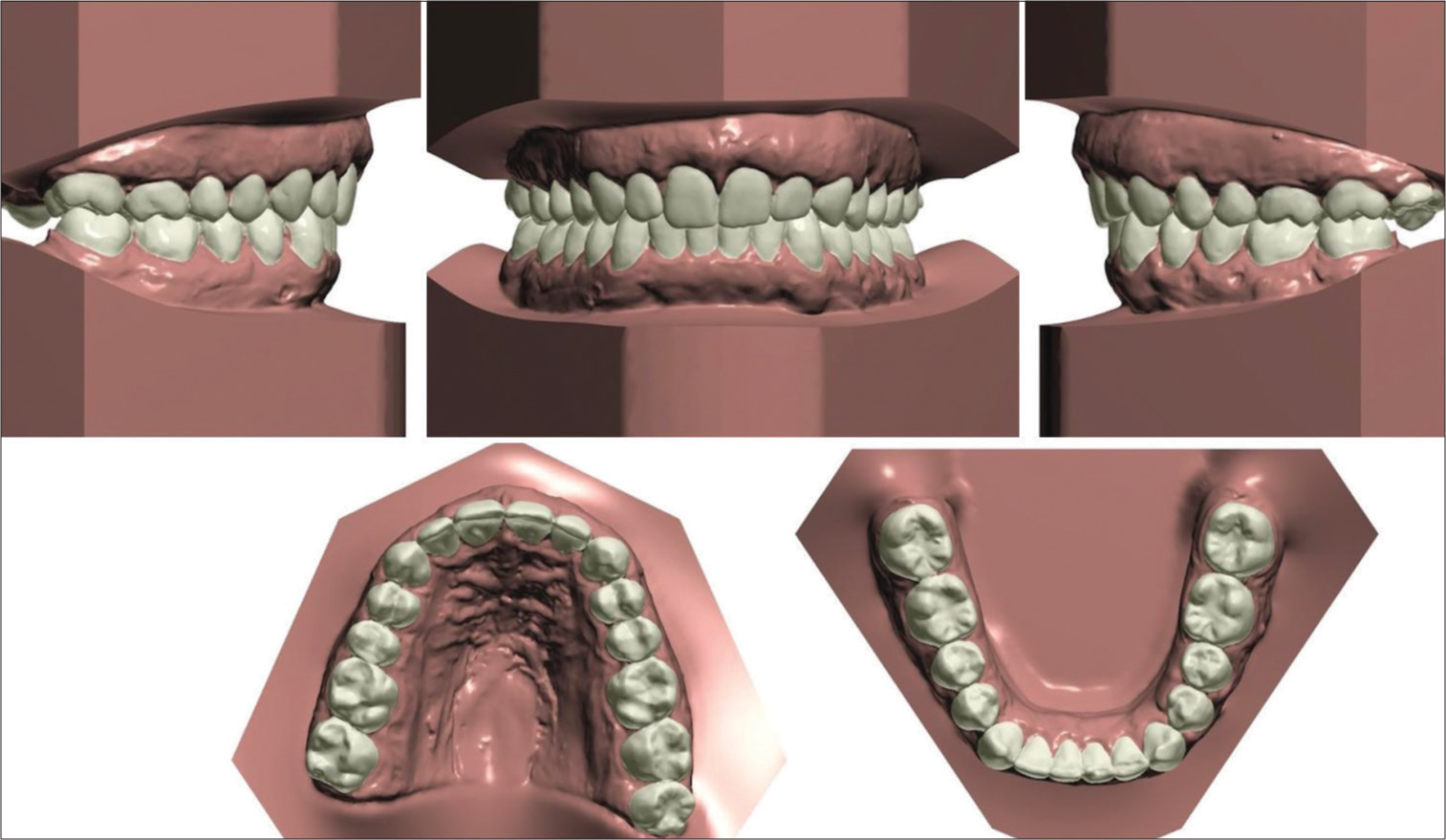
Intraoral examination revealed edge-to-edge dental Class II on both sides, slight crowding in both arches, severe deep bite, and a slight deviation (1 mm) of the lower midline towards the right with respect to the upper midline. The Spee curve was very deep due to overeruption of the lower front section, but the overjet was normal due to significant retroclination of the upper incisors opposing the normally inclined lower incisors [Figures 2 and 3].

Export to PPT
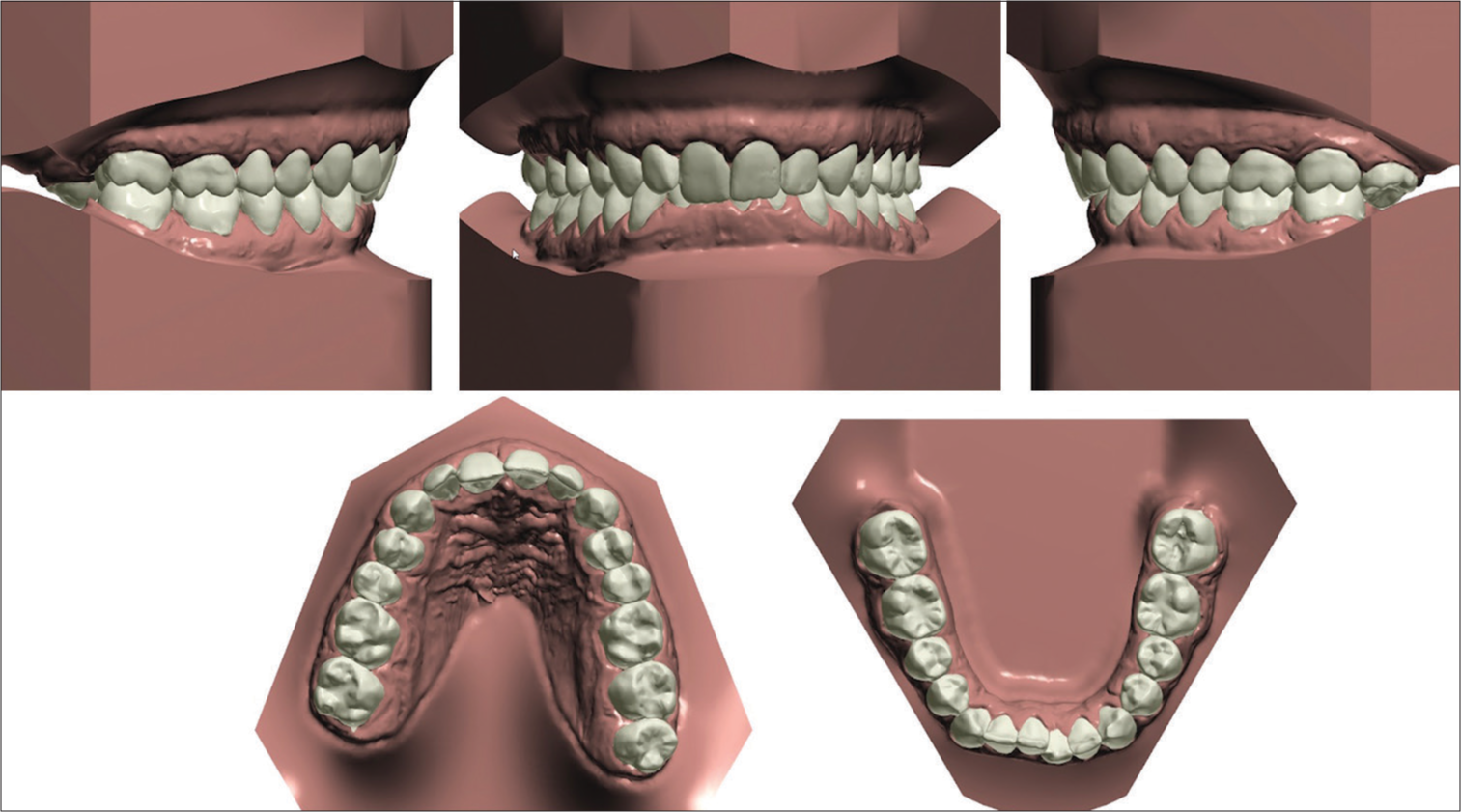
Export to PPT
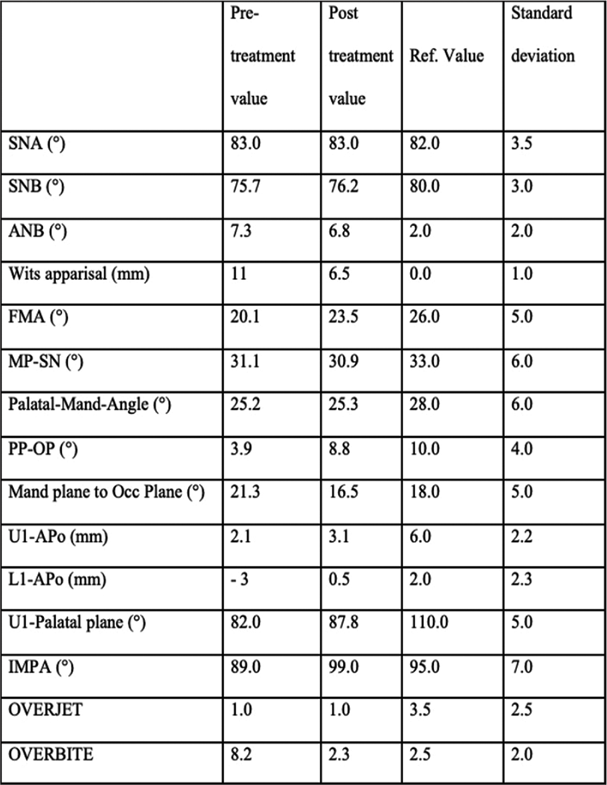
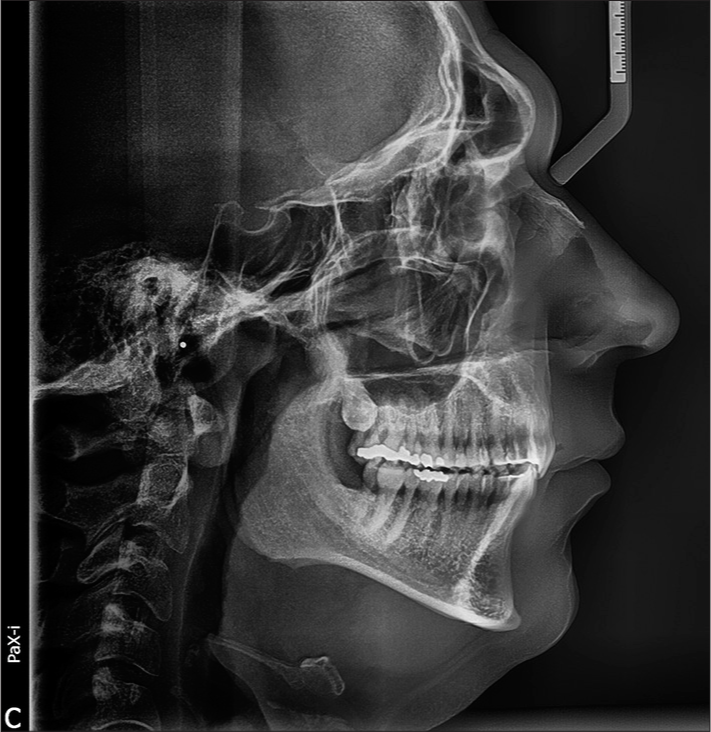
Cephalometric analysis [Figures 4 and 5] confirmed these clinical findings and showed a Class II relationship (A point, nasion, B point (ANB) 7.3°, distance between the projections of A point and B point on the occlusal plane (WITS) appraisal 11) due to a retrognathic mandible (sella, nasion, B point [SNB] 75.7°) in a short face (Frankfort mandibular plane angle [FMA] 20.1°). The maxillary central incisor to sella nasion (SN) angle was 87°, and the angle between mandibular plane and long axis of the lower incisor (IMPA) was 82°, as reported in [Table 1]. Overjet was normal, but overbite was wide.
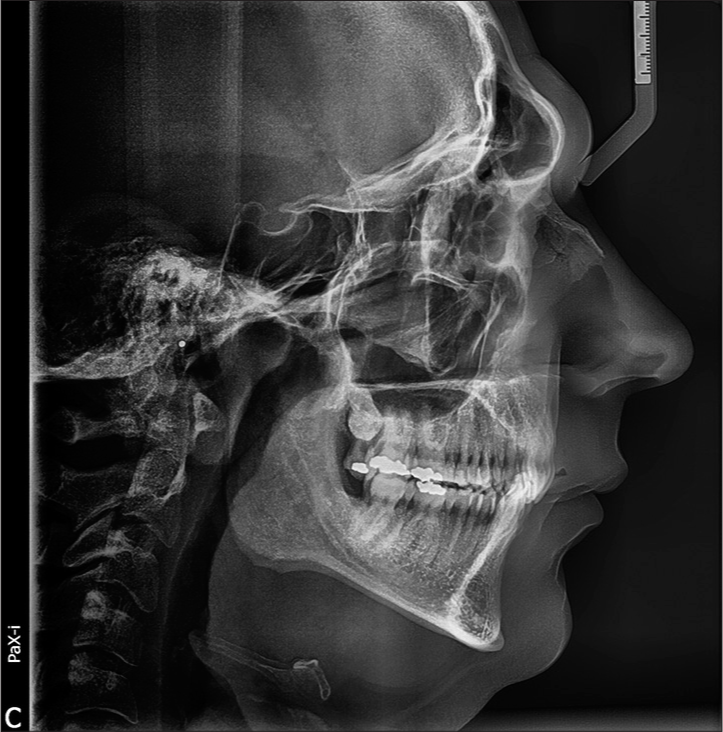
Export to PPT

Export to PPT
Table 1: Pre- and post-treatment cephalometric values.
Panoramic radiography revealed full dentition, a lack of bone defects, no infection, and no temporomandibular joint abnormalities. The periodontal biotype and oral hygiene were good [Figure 6].

Export to PPT
Treatment objectivesThe primary objectives were deep-bite correction and molar and canine Class I. Additional goals were to correct the crowding and obtain ideal overjet and overbite, centering the lower midline with the upper midline, improving facial esthetics, and reducing black buccal corridors during smile.
Treatment alternativesDue to the profile esthetics and severity of the cephalometric values, which revealed skeletal Class II with a WITS appraisal value of 11, the first treatment option proposed to the patient was a combined surgical and orthodontic approach. Specifically, two lower premolars would be extracted in association with bilateral sagittal split osteotomy and genioplasty. This option would have led to a significant improvement in not only the profile but also smile esthetics. However, the patient refused this option, as his main concern was resolving the discomfort in the upper incisal area, and, as far as possible, improving his smile esthetics by means of an esthetic and removable appliance.
Nevertheless, fixed multibracket treatment with extraction was considered, but was ultimately rejected due to potential worsening of the profile, and the patient’s insistence on aligner therapy. Other treatment options involving extraction, for example, fixed mandibular advancement, were also excluded. According to the literature,[9] aligners would not efficaciously control the necessary anterior torque. Furthermore, in an adult patient, fixed mandibular advancement would have led to exclusively dentoalveolar movement.
Hence, we elected for a non-extraction treatment, using aligners aided by miniscrews to level the Spee curve by intruding the lower frontal group with the maximum possible vertical control of the posterior sectors. Indeed, extrusion of the posterior sectors would have increased the divergence and consequently posteriorly rotated the mandible, ultimately worsening the profile and skeletal Class II.
Treatment progressThe pre-treatment setup involved a series of 16 aligners per arch (F22 Sweden and Martina, Due Carrare, Italy) to align the upper teeth by vestibular movement of the incisal sector and roughly 2.5 mm of intrusion of the frontal sector from canine to canine. To aid this intrusion movement, wide beveled attachments were positioned on the second premolars and first molars and horizontal rectangular attachments on the first premolars.[15] Furthermore, two miniscrews (Spider Screw Pin 1.3 × 8 mm) were inserted between the 12 and 13, and between the 22 and 23, to be used in conjunction with elastics [Figure 7]. As regards the lower arch, the setup involved 5.5 mm of intrusion and slight vestibularization of the frontal sector. As in the upper arch, wide beveled attachments were applied to the posterior sector to stabilize the aligner and counterbalance the vertical force in the anterior sector.[15] In the posterior sectors, a slight intrusion movement (1 mm) was planned to prevent any extrusion as a consequence of exerting anterior intrusive forces. Four miniscrews were inserted in the lower arch at the first sitting: two in the anterior region, between teeth 32 and 33 and between the 42 and 43 (Spider Screw Pin 1.3 × 8 mm); and two in the posterior sector, between the 35 and 36 and between the 45 and 46 (Spider Screw K1 1.5 × 8 mm). The posterior miniscrews were positioned bearing in mind that two more would be inserted in the premolar area once the anterior miniscrews had been lost due to the sizable degree of intrusion planned. Furthermore, if necessary, the posterior miniscrews could be used in combination with an elastic stretched between the miniscrews and the posterior sectors of the archwire to prevent their extrusion [Figure 8]. For biomechanical reasons, an intrusion force was applied directly to the aligners rather than the teeth to be intruded. This was made possible, thanks to the use of purpose-designed pliers (SmartPliers®), which are able to thermoform buttons in the required areas of the aligners.

Export to PPT

Export to PPT
After three months, the upper miniscrews were removed, and the lower anterior miniscrews were replaced with two miniscrews inserted between the 35 and 34 and the 43 and 44. Two sectional appliances were then created using 18 × 25 SS archwires passing through the slots of the homolateral miniscrews. This provided a point of application for the elastic in the anterior sector, and at the same time stabilized the system against the intermittent forces it exerted, without hindering the intrusion of the incisors and canines [Figures 9-11].

Export to PPT

Export to PPT

Export to PPT
After the first series of 16 aligners, the refinement phase commenced. This involved a series of four aligners and continuing the intrusive traction in the lower arch alone supported by miniscrews and elastics [Figure 11]. In addition, 6-oz elastics were applied directly to the aligners at the lower first molar and upper canine to perfect the Class I. After 20 pairs of aligners and months of active therapy, splinting was performed in both arches and post-treatment records taken. [Figures 12-14]. In order to improve esthetics and function, we also planned reconstruction of the margins of teeth 3.1 and 3.2.
Export to PPT

Export to PPT
Export to PPT
Treatment outcomesThe treatment was completed in nine months. The crowding had been corrected, the dental midlines centered, and the molar and canine class approached Class I on both sides; the overjet remained correct, there was good light contact in the anterior sector, and the overbite had been considerably reduced [Figures 13 and 14]. Cephalometric analysis [Table 1, Figures 15 and 16] showed that the treatment had been completed without altering the divergence, which remained largely stable. As regards the inclination of the lower incisors, the IMPA had been increased by 10° (from 89° to 99°), as a consequence of the mechanics of correcting the dental class and leveling the arches. The upper incisors had been proclined by roughly 6° (from 82° to 88°).
Export to PPT

Export to PPT
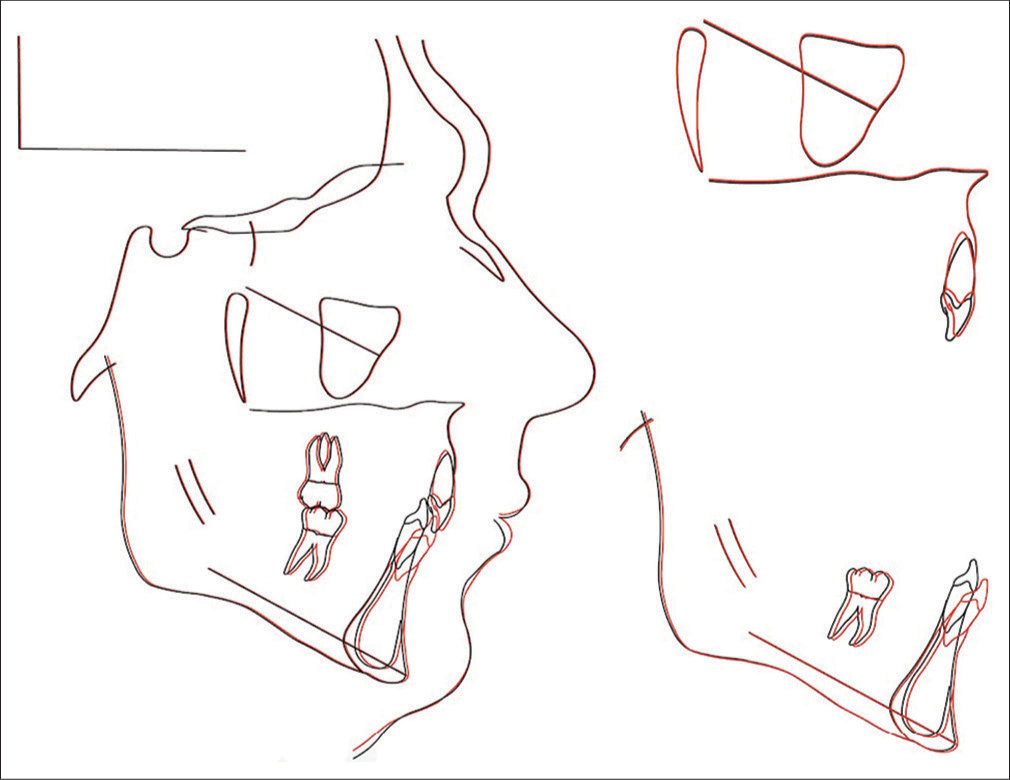
The extraoral photos [Figure 12] showed great improvement in the patient’s profile and increased lower lip prominence. Analysis of the panoramic radiograph [Figure 17] showed that the treatment had been completed with acceptable root parallelism and no signs of root resorption, despite the significant degree of intrusion achieved in the frontal sector. Superimposition of pre- and post-treatment cephalometric tracings [Figure 18], carried out according to the methodology described in the image captions (as developed by Professor Björk),[22,23] revealed that slight distalization of the upper molars had been achieved; this, in conjunction with the slight mesialization of the lower sectors, had improved the dental class. The superimpositions confirmed the significant degree of intrusion of the upper and lower frontal sectors. Checkup at one month confirmed the stability of the results achieved [Figure 19].

Export to PPT
Export to PPT

Export to PPT
DISCUSSIONAlthough aligners were once limited to the treatment of cases of slight to moderate complexity,[24,25] over time, they have become far more clinically reliable and can now be used in certain complex cases.[26-29] In this scenario, it is interesting to underline that some significant differences between orthodontists and general dentists have emerged regarding the experience and case selection of clinicians using aligners in their clinical practice.[30,31] However, as the severity of the malocclusion increases, so does the number of aligners in the series, which tends to reduce predictability.[9] In such cases, “hybrid” approaches that combine aligners with different types of auxiliary may increase predictability.[18,19] For example, this case report documents the resolution of a case of severe deep bite by exploiting the potential of both aligner setup and skeletal anchorage. In this case, skeletal anchorage was used to improve the predictability of intrusion of the frontal sector, a notoriously unpredictable orthodontic movement.[10,15-17].
This option was selected because the patient refused combined surgical and orthodontic treatment, which markedly increased the difficulties involved. Indeed, to correct the deep bite, it was necessary to level the Spee curve almost entirely via bodily intrusion of the lower frontal group, as extrusion of the premolar and molar sectors would have increased the divergence and further worsened the profile. This dual objective would be difficult to achieve via aligners alone[9,15-17] and it was therefore decided to exploit miniscrews for skeletal anchorage. In addition to providing an excellent outcome, this was expected to reduce treatment times.
Park and Kim[32] successfully used a different method for correcting deep bite, but in our case, the malocclusion was more severe, and the patient requested a treatment that would be as rapid and unobtrusive as possible. However, studies reported by Krieger et al. showed that overbite management by aligners alone requires overcorrection in the planning phase, and therefore a greater number of aligners in the series, and consequently an increase in treatment time.[17,19] To date, only a few studies[33,34] involving the use of miniscrews to intrude the lower frontal sector have been published, and among these, none have proposed a combined approach with aligners.
For the lower arch, our setup prescribed roughly 5.5 mm of intrusion and slight vestibularization of the frontal group. The ideal post-treatment proclination would have been greater than that planned in the setup, but this was limited in reality because the intrusion, aided by the miniscrews, would have provided a point of application of the vestibular intrusion force at the center of resistance of the frontal group, thereby considerably increasing the proclination tendency during treatment. This factor, associated with the amount of vestibularization provoked by the use of Class II elastics,[35] would have resulted in excessive proclination of the incisors and most likely opening spaces. Hence, a substantial amount of pure intrusion was planned as part of the setup, associated with a minimal amount of vestibularization for anchorage maintenance.
In order to best exploit the strategy provided for in the setup and reduce the risk of anchorage loss in the incisal sectors, the aligners would have to cover as much of the vestibular surface of the incisors and canines as possible. Therefore it was decided to apply the intrusive force directly to the aligners rather than the teeth to be intruded. This necessitated refinement of the gingival margins of the aligner and the application of buttons on the teeth. This was achieved via purpose-designed pliers (SmartPliers®, which are able to thermoform buttons in the required areas of the aligners; using this tool, it was also possible to vary the points of force application and the degree of tension in the elastics.
Thanks to a certain amount of lower incisor vestibularization, achieved through both intrusion and Class II elastics,[33] the lower lip prominence and therefore the profile improved. The combined use of aligners and miniscrews provided a rapid intrusion movement without unwanted side effects such as root resorption [Figure 17] or gingival inflammation. Moreover, as demonstrated by the superimpositions [Figure 18], a good amount of pure intrusion had been achieved. This type of orthodontic movement is difficult to achieve by means of aligners alone, which bring about deep-bite correction predominantly via proclination of the lower incisors and intrusion of the upper frontal sector.[16]
When planning any treatment involving miniscrews, particular attention must be paid to their implantation sites.[36] In our case, self-tapping and self-threading miniscrews were inserted in areas with adherent gum, except for that between the 43 and 44, which was positioned more apically due to a paucity of interradicular space.
After three months, we decided to replace the miniscrews in the anterior area with miniscrews positioned between the premolars to reinforce the skeletal anchorage system. This, together with two 18 × 25 SS sectional appliances, made the system more resistant and better able to withstand the intermittent forces exerted by the elastics. Indeed, the literature tells us that intermittent forces are poorly tolerated by orthodontic miniscrews, which rely solely on primary stability.[37]
As demonstrated by the superimpositions, the use of light Class II elastics, considerable intrusion, and stripping management resulted in dental movement, with no alterations to the basal bone. The hybrid aligner treatment was completed in only 20 steps per arch and nine months.
CONCLUSIONIt was not possible to achieve optimal esthetic and functional outcomes, as only combined surgery and orthodontics can provide full Class I and frontal sector torque correction. Nevertheless, our results show that with careful planning, temporary anchorage devices, and elastics, this hybrid aligner protocol can be used to correct deep bite.
留言 (0)