We propose a novel technique that uses a non-contact, low intensity, continuous wave energy source with minimal absorption by water to excite nanoparticles that generate thermal and acoustic energy on the surface of stones resulting in stone failure. In this proof-of-concept study, we have demonstrated for the first time the ability to successfully fragment common types of kidney stones using the described photonic lithotripsy. The NIR energy source used in this study is not directly responsible for the fragmentation of the stones but is used to excite the nanoparticles as confirmed by our control specimens.
Notably, the tested nanoparticles can fragment stones with the NIR energy being up to 20 mm from the stone surface (can be shorter), and at power settings of less than 5 W (compared to clinical lasers which use power settings up to 100 W) [6]. These findings are exciting in considering potential future applications.
To better understand how this technology fragments kidney stones, it was important to analyze the same stone pre- and post-treatment. This was successfully achieved using observational data and micro-CT analysis. The micro-CTs showed extensive cracking throughout the stone samples after treatment, which corresponded to an increase in surface area post-irradiation due to new surface creation. There was also a decrease in the Hounsfield units, for which we propose two different mechanisms. One is the breakdown and ultimate reduction in density as the stone fragments, and the other is a change in the mineral composition of the stone due to the thermal energy generated by the nanoparticles (this thermal degradation has been shown previously using FTIR [22]). Use of micro-CT in identifying mineral composition of stones has been reported in the literature, although it has not been used to determine mineral compositional changes pre and post stone treatment [23, 24]. Both compositional change and stone fragmentation can have a significant effect on HU and therefore, it is challenging to differentiate between the two mechanisms in a quantitative manner. The proposed mechanism of stone failure and the contribution of these effects has been outlined in more detail previously using scanning electron microscopy and thermal imaging during photonic lithotripsy [22]. Based on these studies, current byproducts of this technology appear to be predominantly thermal in nature, although these nanoparticles can be further engineered to enhance the acoustic or mechanical effect for fragmentation (and potentially decrease the thermal effect) as well as modified with ligands to directly target stones [11, 12].
The specific NIR energy source used had a noticeable effect on the effectiveness of photonic lithotripsy as did the duration of irradiation and type of nanoparticle used (Fig. 7). For example, there was a lower fragmentation rate with the gold nanoparticles when irradiated by the 1320 nm energy source. This may be attributed to the NIR wavelength used since these gold nanoparticles were designed to have peak absorption at 808 nm and therefore absorb significantly lower amounts of energy outside of this region.
It is encouraging to note that our proof-of-concept study on photonic lithotripsy demonstrated a 70% or greater fragmentation rate across both NIR energy sources, with the exception of the gold nanoparticles and the 1320 nm wavelength, as discussed above. The 785 nm energy source appears to perform the best across all the nanoparticles tested with the majority of stones fragmenting in the first 3-min time period. In the control groups (stones rehydrated with simulated urine but not treated with nanoparticles), none of the 20 stones tested across both wavelengths resulted in fragmentation, highlighting that the NIR energy sources excite the nanoparticles and do not contribute to the fragmentation of the stones.
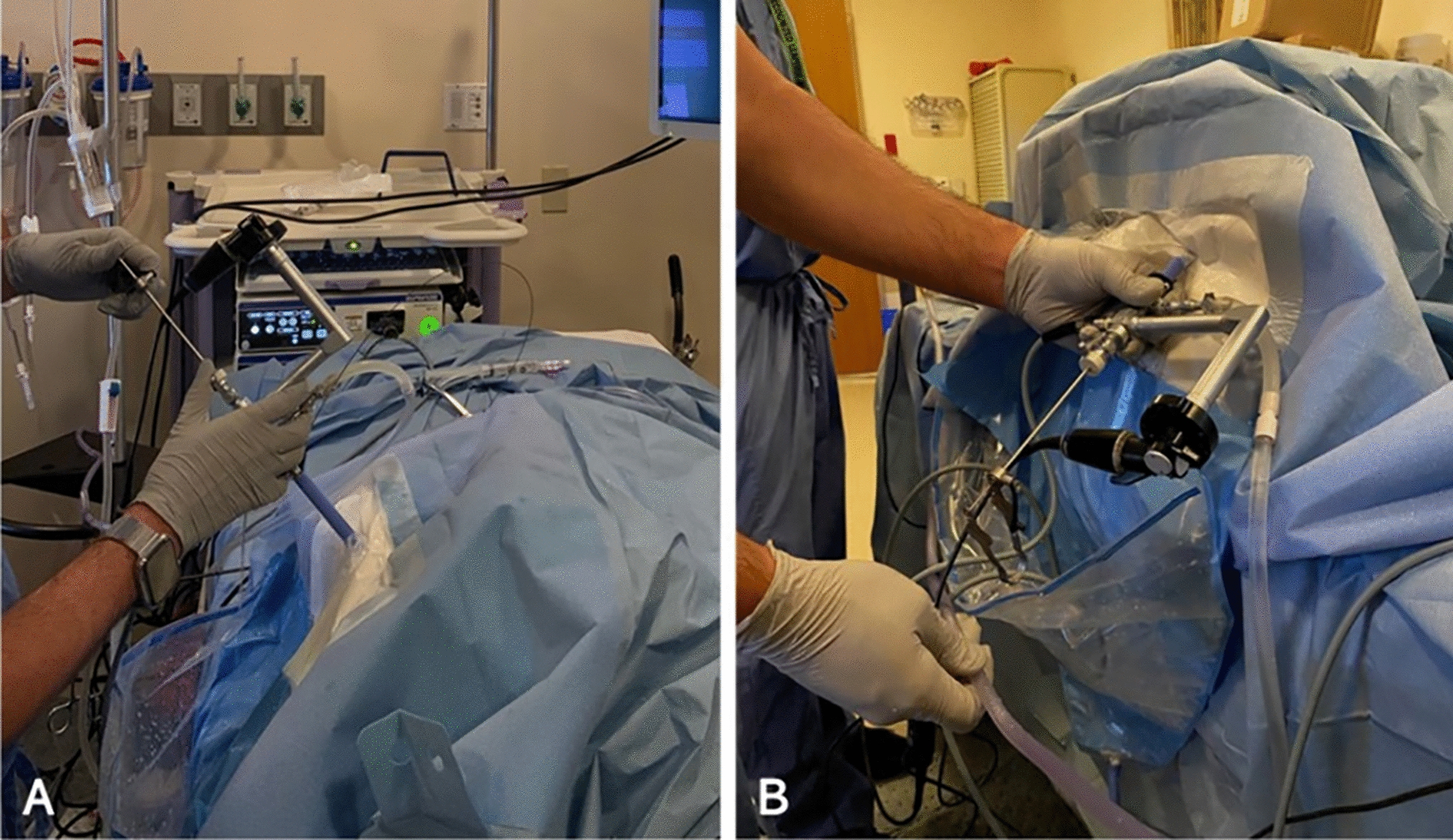
We envision initial trials with photonic lithotripsy to be performed similar to current clinical practice with patients under anesthesia and NIR energy delivered via a ureteroscope as there is a lack of data regarding potential pain during photonic lithotripsy. However, the wavelengths used in this study are minimally absorbed by water, unlike the current clinical lasers, which gives these NIR energy sources the ability to penetrate tissue with minimal adverse effects, suggesting the potential for this technology to be used extracorporeally. For example, nanoparticles could be delivered to the site of the stone and excited extracorporeally with a low intensity energy source that can penetrate tissue. Extracorporeal use with the current wavelengths would theoretically be for stones up to 3.5 cm from the skin surface, which would only be applicable to a limited number of circumstances [11, 12, 25, 26]. Future development of this technology would incorporate energy sources with deeper penetration capabilities, such as radio frequency energy (20–200 cm depending on the frequency used) [27].
The nanoparticles used in this study are electrostatically bound to the stones, but a stronger interaction between the nanoparticles and the stone’s surface would result in a more efficient transfer of energy from the nanoparticles to the stone, and theoretically, a quicker fragmentation rate. This could also reduce the risk of tissue damage through improved binding to the stone compared to the surrounding tissue. This concept has been proposed previously by Ramaswamy et al. with microbubbles functionalized with bisphosphonates to more effectively bind to kidney stone surfaces [28]. We are currently designing nanoparticles with ligands that will allow for such ‘targeting’ of stones.
Similar to this work and the microbubble-based technology referenced above, others also aim to disrupt the current standards for the treatment of urolithiasis. Perhaps the most developed at this time is Burst Wave lithotripsy (©Sonomotion, San Mateo, CA). In Burst Wave lithotripsy, stones are identified via ultrasound, and then fragmented using low pressure ultrasound waves [29]. Currently, this technology is being used in clinical trials as an investigational device. While results have been promising, a key limitation is the need to use ultrasound for pinpoint localization of stones as identification of stones via ultrasound is challenging [30, 31]. In photonic lithotripsy, we anticipate being able to use various modalities for intra-procedural imaging including fluoroscopy, ultrasound, and direct visualization.
While this study has successfully demonstrated the ability of nanoparticles to fragment human kidney stones using low energy, non-contact energy sources, several limitations must be noted. First, the tested stones were obtained during surgical procedures for stone treatment so there is a potential for stone alteration due to the lithotripsy technique used intraoperatively. However, we decided not to use simulated stones (such as Bego stones, BEGO USA, Inc.) to assess this technology given the ultimate goal to target stones and simulated stones are predominantly designed to match the mechanical and not chemical properties of a human kidney stone. Second, some of the stones used were of mixed composition, although the use of pure stones would limit the amount of stones available for testing as less than 10% of stones are reportedly composed of a single component [32]. Third, stones were tested in an in vitro environment. Future studies are planned to evaluate photonic lithotripsy with stones immersed in simulated urine. Fourth, the time periods chosen for energy exposure were not refined and additional optimization of timing as well as quantification of post-treatment fragment sizes will allow for more precise assessment of the different variables involved. Finally, only small-sized stones were tested for proof-of-concept and so evaluation of larger stones would be needed to translate this technology into a clinical setting.
Future directions include addressing several of the above limitations and preparing for in vivo testing. Safety studies in urothelial cell cultures as well as small animal models will be needed. We do not anticipate there to be toxicity concerns as prior in vivo studies have demonstrated the safety of these nanoparticles, including for oncologic applications [11, 33,34,35]. Various parameters will need to be optimized such as nanoparticle concentrations. In addition, nanoparticles that can specifically bind to stones may improve efficiency and decrease potential for tissue damage, as previously discussed. Ultimately, our goal is to assess the efficacy of photonic lithotripsy using the targeting nanoparticles in a porcine model and compare with current standard of care.




留言 (0)