
記住我





A detailed description of the methods, including procedures, intervention and measurement instruments, was described in our study protocol [22]. A comprehensive summary is included below.
Trial designThis investigator-blinded, randomised controlled trial studied the efficacy of the Tackle your Tics treatment (TYT), compared with a waiting list control group (WLCG, 3 months waiting) in children and adolescents with tic disorders in a 1:1 ratio.
Ethical considerationsThe study was registered at the International Clinical Trials Registry Platform (NL8052), approved by the medical ethical committee of Amsterdam UMC (NL66340.018.18) and adhered to the Declaration of Helsinki. Written informed consent was received from all parents and participants over 12 years. Representatives of the Dutch patient organisation continuously reviewed the research process, as members of the research team [23].
ParticipantsChildren and adolescents and their parents were recruited from July 2020 to May 2022 by the Dutch Tourette Association and three participating Dutch paediatric expert centres on tic disorders: Levvel, Yulius and Accare.
Children and adolescents had to meet the following inclusion criteria to be eligible for participation: (a) age 9–17 years, (b) having been diagnosed with TS or another chronic tic disorder (CTD), in accordance with the diagnostic criteria of the Diagnostic and Statistical Manual of Mental Disorders, 5th edition [1], (c) with at least moderate tic severity as indicated by a total tic score of more than 13 (or more than 9 for participants with motor or vocal tics only) on the Yale Global Tic Severity Scale, (YGTSS; [24]).
Exclusion criteria for participation were: (a) having received behavioural treatment for tics in the past 12 months (to safeguard that children were motivated to relearn the ERP exercises), (b) receiving pharmacological treatment for tics that has not been stable for the past six weeks or with planned changes during study participation, (c) poor mastery of the Dutch language, (d) IQ < 75, (e) serious physical disease, (f) substance abuse, (g) suicidality, (h) psychotic disorders, (i) poor group functioning or low motivation, as reported by the child, parents or local clinician. Co-occurring attention-deficit/hyperactivity disorder (ADHD), obsessive–compulsive disorder, anxiety disorders or mood disorders were no reason for exclusion, unless immediate treatment or an adaptation to the treatment protocol was required.
Demographics and medical history were derived from a clinical intake interview. Families reported the child’s age, sex and gender, cultural background, family composition, marital status, child’s education, parent’ highest completed educational level, parents’ professions, monthly family income (1–6 scale), previously diagnosed comorbidities, previous or current treatment for tics or other psychiatric problems and family history of tics. Parents’ professional level was determined by the coding system ISCO-08, 1–4 scale (International Standard Classification of Occupations: ISCO-08 [25].
Psychiatric comorbidities were determined with an online semi-structured interview at baseline (Anxiety Disorder Interview Schedule; ADIS, parent and child version) [26]. To limit unnecessary burden, the child version was only completed with children aged 12 years or older, who were able to give a one-hour online interview independently.
InterventionsParticipants in the TYT condition received treatment, in groups of 4–8 participants within 1 month after randomisation. Tackle your Tics is a brief, condensed group treatment with evidence-based ERP [27]. In this treatment, participants are trained to suppress all their tics simultaneously for a prolonged time (response prevention) while focussing on tolerating the preceding sensations or ‘tic alarms’. Treatment sessions were supplemented with innovative, supportive components including daily, one-hour workshops about living and coping with tics given by experts by experience. These young adult patients, trained for this study, taught the children how to cope with their symptoms in a positive, creative way. In the workshops, three themes were discussed and visualized (by writing, painting and mind mapping): self-acceptance, solution-oriented thinking and positive characteristics and strengths. See Appendix 1 for an overview of the programme content. Due to COVID-19 regulations, the treatment programme was slightly modified by providing all parent meetings online instead of face-to-face and introducing basic safety COVID-19 measures, in accordance with national guidelines, such as 1.5-m distance and self-tests. Online participation was available if a participant would not be able to complete the treatment face-to-face due to quarantine. Treatment was provided by therapists with 3–15 years of experience in treating tic disorders, assisted by co-therapists. Depending on group size (4–8 participants), a team of 2–3 experienced therapist and 1–2 co-therapists, and 1–2 trained experts by experience provided the programme. Treatment took place at Levvel, an academic centre for child and adolescent psychiatry in Amsterdam, the Netherlands.
Treatment integrity was enhanced by team intervision meetings before each treatment group and assessed by two independent, trained raters (bachelor students and one expert psychologist). Standardised forms to score the required programme components were used to rate a random 20% of all sessions, based on observations or audio recordings (forms available upon request).
Participants in the WLCG received this same treatment after a waiting period of 3 months, in which they received no psychosocial treatments for tics.
OutcomesOur primary outcome was tic severity, as assessed by the blinded, independent researcher (AH) in online interviews with the children, accompanied by and – if necessary – helped by their parents. Tic severity was measured by the total tic score of the YGTSS, covering the last week. This semi-structured interview for the assessment of tic severity is used in most clinical trials as the primary outcome measure [28] and has good reliability and other psychometric properties [29], as well as high reliability between online and in-person ratings [30]. A revised version of the YGTSS (YGTSS-R, [31]) was translated and analysed for this study as sensitivity analysis.
As secondary outcome measures, we used the YGTSS motor and vocal tic scores and the YGTSS tic-related impairment rating, which is an additional question to assess overall impairment in daily functioning that the child experiences as a consequence of having tics. Quality of life was measured by the Gilles de la Tourette Syndrome Quality of Life Scale for children and adolescents; C&A-GTS-QOL, total problem score and life satisfaction score [32]. We rated patients’ beliefs and cognitions about their tics using the Beliefs About Tics Scale [33]. This 20 item self report scale measures tic-related cognitions as beliefs about the sense of relief after ticking or the (negative) experiences while suppressing tics. The higher the score, the higher the degree to which the subject negatively perceives his/her experience when suppressing tics (or resisting tic urges).
As additional secondary outcome measures, tic-related cognitions, emotional/behavioural functioning, family functioning (including parenting stress, care-related quality of life in informal caregivers and overall family functioning) and treatment satisfaction and adherence were assessed. On the treatment satisfaction surveys, mean scores higher than 3 on a 5-point scale indicated a favourable treatment satisfaction. For the instruments used and their psychometric characteristics, see Table 1. All secondary outcomes apart from the YGTSS tic-related impairment rating and Outcome and Session Rating Scales (ORS/SRS) were completed online.
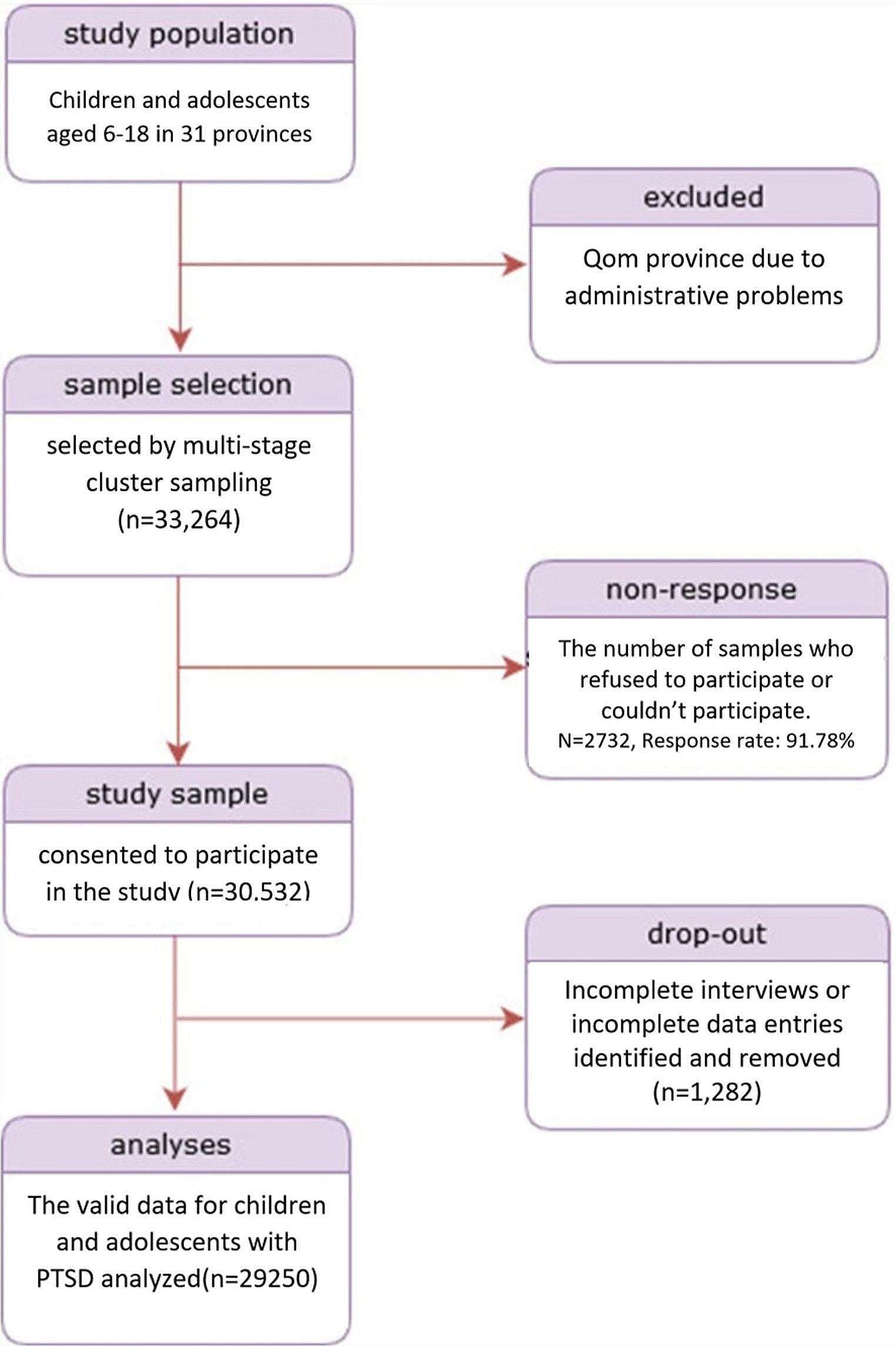
Table 1 Used Instruments, their Psychometric Characteristics and Time pointsAll outcomes were assessed at baseline (T1; for TYT: within two weeks before the start of the treatment; for WLCG: at the start of the study), post-treatment (T2, for TYT: one week after the fourth treatment day; for WLCG: four weeks after T1), at 3-months (T3, both conditions: 3 months after T1) and 6-months follow-up (T4, both conditions: 6 months after T1) at parallel time intervals for participants in the TYT and WLCG condition (see Fig. 1).
Fig. 1
Participation Flow of the Tackle your Tics Study
Sample sizeA sample size of 104 participants was needed to detect univariate differences between TYT and WLCG (p ≤ 0.05) at the primary outcome on T2, at an effect size of Cohen’s d = 0.5, with a power of 0.80.
RandomisationA research assistant randomly assigned eligible participants using a computerised data management system (Castor EDC) to either direct treatment (TYT) or the waiting list (WLCG), using block randomisation (block size 2–4 participants) and stratification by gender.
BlindingIncluded families were informed of randomisation outcome prior to the baseline assessments, since they had to make practical arrangements (e.g., taking time off from work, making hotel reservations). However, the investigator who assessed the primary outcome measure was blinded to treatment allocation.
Statistical analysesSPSS Version 28 was used for all analyses (IBM SPSS Statistics for Windows, NY: IBM Corp). Results with p < 0.05 were considered statistically significant. For significant results, the standardised mean difference (SMD) was calculated as a measure of effect size, considering values of 0.2–0.5 as small, values of 0.5–0.8 as medium, and values > 0.8 as large effect sizes.
Differences in background characteristics between participants and non-participants (who did not meet the inclusion criteria or did not provide consent) as well as differences in baseline characteristics between TYT and WLCG were analysed by independent t-tests, Chi-square tests or Fisher’s exact tests.
To determine the efficacy of Tackle your Tics, difference in change on the primary outcome YGTSS total tic severity scores over time (T1–T2 and T1–T2–T3) between the TYT condition versus WLCG were compared with Generalised Estimating Equations (GEE) [34], which accounts for the dependency between repeated observations. This way, we examined the interaction between time and group as a test of effectiveness. Since the WLCG received treatment after T3, analyses were conducted from T1 to T3. T4-results were reported descriptively. Participants were included in the analysis if a score was available at one or more assessments.
In the same way, difference in change in secondary outcomes between the TYT and WLCG were tested with GEE. For each outcome, a separate GEE analysis was conducted.
As sensitivity analyses, we reanalysed our data to check for possible influence of deviations from the protocol, i.e. (1) missed programme components (> 3 h of children’s sessions or > 2 h of parent meetings), (2) a different treatment than planned (> 3 h online participation or a different condition than randomised) or (3) changes in medication. Deviations were included as covariates in the GEE-analysis, to investigate if these had obscured the original analyses.
Furthermore, we examined whether tic severity at baseline, premonitory urge severity, age, sex, family functioning, and comorbidity predicted treatment response. These outcomes were included as covariates in the GEE-analyses, to test if these led to an extra differential change over time.
To compare the number of children with a positive treatment response in both treatment groups by means of a Chi square test, a 25% reduction of the total tic score of the YGTSS from pre- to post-treatment was defined as a positive response [29].
留言 (0)