
記住我







Available online 1 April 2024
 Author links open overlay panel, , , , , , , , , , , , , , Highlights•
Author links open overlay panel, , , , , , , , , , , , , , Highlights•Lp(a) level should be measured at least once in all adults.
•Lp(a) levels represent a continuum of risk, not a risk threshold at a dichotomous cutpoint.
•Risk classification by Lp(a) level ranges from low (<75 nmol/L) to high (≥125 nmol/L).
•Lp(a) risk categories apply across races and ethnicities.
•High Lp(a) levels warrant early and more-intensive risk factor management.
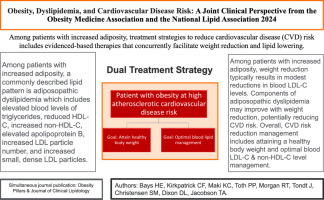
Since the 2019 National Lipid Association (NLA) Scientific Statement on Use of Lipoprotein(a) in Clinical Practice was issued, accumulating epidemiological data have clarified the relationship between lipoprotein(a) [Lp(a)] level and cardiovascular disease risk and risk reduction. Therefore, the NLA developed this focused update to guide clinicians in applying this emerging evidence in clinical practice. We now have sufficient evidence to support the recommendation to measure Lp(a) levels at least once in every adult for risk stratification. Individuals with Lp(a) levels <75 nmol/L (30 mg/dL) are considered low risk, individuals with Lp(a) levels ≥125 nmol/L (50 mg/dL) are considered high risk, and individuals with Lp(a) levels between 75 and 125 nmol/L (30–50 mg/dL) are at intermediate risk. Cascade screening of first-degree relatives of patients with elevated Lp(a) can identify additional individuals at risk who require intervention. Patients with elevated Lp(a) should receive early, more-intensive risk factor management, including lifestyle modification and lipid-lowering drug therapy in high-risk individuals, primarily to reduce low-density lipoprotein cholesterol (LDL-C) levels. The U.S. Food and Drug Administration approved an indication for lipoprotein apheresis (which reduces both Lp(a) and LDL-C) in high-risk patients with familial hypercholesterolemia and documented coronary or peripheral artery disease whose Lp(a) level remains ≥60 mg/dL [∼150 nmol/L)] and LDL-C ≥ 100 mg/dL on maximally tolerated lipid-lowering therapy. Although Lp(a) is an established independent causal risk factor for cardiovascular disease, and despite the high prevalence of Lp(a) elevation (∼1 of 5 individuals), measurement rates are low, warranting improved screening strategies for cardiovascular disease prevention.
Section snippetsIntroduction (Preface)The lipoprotein(a) [Lp(a)] field is rapidly evolving on many fronts, warranting this focused update to the 2019 National Lipid Association (NLA) Scientific Statement on Use of Lipoprotein(a) in Clinical Practice.1 Recent evidence has influenced our understanding of whom should have Lp(a) levels measured, how to interpret Lp(a) levels for use in risk assessment, and clinical management of patients with elevated Lp(a). The NLA now recommends: (1) measurement of Lp(a) levels at least once in every
Accumulating data from large, population-based studies indicate that elevated plasma Lp(a) is an important independent, causal risk factor for atherosclerotic cardiovascular disease and calcific aortic valve stenosisThe most notable of these studies are two analyses of the UK Biobank.2,3 Their enormous sample sizes (n = 460,506 and 413,734, respectively) allowed several key questions to be addressed with unprecedented statistical power.
First, a continuous, log-linear relationship between baseline Lp(a) and risk for atherosclerotic cardiovascular disease (ASCVD) events was observed, with a significant (albeit small) increase in risk at what would usually be considered “low-risk” levels of Lp(a)
The adult populationThe risk for ASCVD events that is associated with Lp(a) is independent of LDL-C and is attributed to the atherogenic, proinflammatory, and prothrombotic properties of Lp(a).20 Lp(a) is associated with an increased risk of incident ASCVD even in the absence of a family history of heart disease.21 Systematic universal Lp(a) screening can improve health outcomes by increasing awareness of, and enabling precision in, ASCVD prevention strategies22 and individualization of therapy selection.23
How should Lp(a) be measured?Lp(a) measurement is complicated by the unique structure of apolipoprotein(a) [apo(a)]. Apo(a) is characterized by a variable number of identically repeated kringle IV type 2 (KIV2) sequences (ranging from 3 to >40 copies) that correspond to differently sized isoforms of Lp(a).37 Therefore, antibodies that recognize epitopes in the KIV2 sequence tend to underestimate the concentrations of smaller Lp(a) isoform sizes (which tend to be associated with higher Lp(a) levels and higher ASCVD risk),
Risk assessmentThe assessment of CVD risk offers the opportunity to implement tailored risk-reducing strategies, matching the intensity of pharmacological treatments to the absolute global risk of the patient. Several professional cardiology societies have identified high Lp(a) as a “risk-enhancing” or “risk-modifying” factor. The 2019 American College of Cardiology (ACC)/American Heart Association (AHA) Guideline on the Primary Prevention of CVD identified an elevated Lp(a) ≥125 nmol/L as a “risk-enhancing”
E. SummaryWhile specific Lp(a)-lowering therapies are not currently available, elevated Lp(a) is actionable now88(Table 2; Table 3). Lp(a) level should be measured at least once in all adults to identify individuals with high Lp(a) levels for implementation of early and intensive risk factor management. For CVD risk assessment, Lp(a) levels should be used to stratify patients as low risk (<75 nmol/L) or high risk (≥125 nmol/L), and individuals with Lp(a) levels in between should be considered as
Use of AI and AI-assisted Technologies StatementAI has not been used in the writing process.
Ethical StatementThis work does not involve the use of human subjects or animals.
CRediT authorship contribution statementMarlys L. Koschinsky: Conceptualization, Writing – original draft, Writing – review & editing. Archna Bajaj: Writing – review & editing. Michael B. Boffa: Writing – original draft, Writing – review & editing. Dave L. Dixon: Writing – review & editing. Keith C. Ferdinand: Writing – review & editing. Samuel S. Gidding: Writing – original draft, Writing – review & editing. Edward A. Gill: Writing – review & editing. Terry A. Jacobson: . Erin D. Michos: Writing – original draft, Writing – review &
Declaration of interest statementMarlys L. Koschinsky received honoraria from Novartis and Eli Lilly as a consultant and a research contract from Abcentra as an independent research contractor; Archna Bajaj received research support from Amgen, Ionis, Novartis, NewAmsterdam Pharma, and Regeneron and consulting fees from Kaneka; Michael B. Boffa has no interests to declare; Dave L. Dixon received research funding from Boehringer Ingelheim as a PI; Keith C. Ferdinand received consulting fees from Amgen, Sanofi, Novartis, Eli
References (88)C. Yeang et al.Novel method for quantification of lipoprotein(a)-cholesterol: implications for improving accuracy of LDL-C measurementsJ Lipid Res
(2021)
D.K. Arnett et al.ACC/AHA guideline on the primary prevention of cardiovascular disease: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice GuidelinesJ Am Coll Cardiol
(2019)
G.J. Pearson et al.2021 Canadian Cardiovascular Society guidelines for the management of dyslipidemia for the prevention of cardiovascular disease in adultsCan J Cardiol
(2021)
M. Trinder et al.Repeat measures of lipoprotein(a) molar concentration and cardiovascular riskJ Am Coll Cardiol
(2022)
B. Enkhmaa et al.Non-genetic influences on lipoprotein(a) concentrationsAtherosclerosis
(2022)
E.D. Michos et al.Use of the coronary artery calcium score in discussion of initiation of statin therapy in primary preventionMayo Clin Proc
(2017)
A. Mehta et al.Independent association of lipoprotein(a) and coronary artery calcification with atherosclerotic cardiovascular riskJ Am Coll Cardiol
(2022)
C.L. Jackson et al.Lipoprotein(a) and coronary artery calcium in comparison with other lipid biomarkers: the Multi-Ethnic Study of AtherosclerosisJ Clin Lipidol
(2023)
N. Perrot et al.Ideal cardiovascular health influences cardiovascular disease risk associated with high lipoprotein(a) levels and genotype: the EPIC-Norfolk prospective population studyAtherosclerosis
(2017)
P.M. Ridker et al.Effects of bempedoic acid on CRP, IL-6, fibrinogen and lipoprotein(a) in patients with residual inflammatory risk: a secondary analysis of the CLEAR Harmony trialJ Clin Lipidol
(2023)
R.S. Wright et al.Pooled patient-level analysis of inclisiran trials in patients with familial hypercholesterolemia or atherosclerosisJ Am Coll Cardiol
(2021)
V.A. Bittner et al.Effect of Alirocumab on Lipoprotein(a) and Cardiovascular Risk After Acute Coronary SyndromeJ Am Coll Cardiol
(2020)
A. Sahebkar et al.Effect of extended-release niacin on plasma lipoprotein(a) levels: a systematic review and meta-analysis of randomized placebo-controlled trialsMetabolism
(2016)
P.L. Canner et al.Fifteen year mortality in Coronary Drug Project patients: long-term benefit with niacinJ Am Coll Cardiol
(1986)
D.I. Chasman et al.Polymorphism in the apolipoprotein(a) gene, plasma lipoprotein(a), cardiovascular disease, and low-dose aspirin therapyAtherosclerosis
(2009)
P. Lacaze et al.Aspirin for primary prevention of cardiovascular events in relation to lipoprotein(a) genotypesJ Am Coll Cardiol
(2022)
M.H. Sukkari et al.Is there a benefit of aspirin therapy for primary prevention to reduce the risk of atherosclerotic cardiovascular disease in patients with elevated lipoprotein (a) —A review of the evidenceAm J Prev Cardiol
(2023)
S. Tsimikas et al.Emerging RNA therapeutics to lower blood levels of Lp(a): JACC Focus Seminar 2/4J Am Coll Cardiol
(2021)
M.D. Kelsey et al.Contemporary patterns of lipoprotein(a) testing and associated clinical care and outcomesAm J Prev Cardiol
(2023)
P.E. Stürzebecher et al.Trends and consequences of lipoprotein(a) testing: cross-sectional and longitudinal health insurance claims database analysesAtherosclerosis
(2023)
H.S. Bhatia et al.Trends in testing and prevalence of elevated Lp(a) among patients with aortic valve stenosisAtherosclerosis
(2022)
A.P. Patel et al.Lp(a) (lipoprotein[a]) concentrations and incident atherosclerotic cardiovascular disease: new insights from a large national biobankArterioscler Thromb Vasc Biol
(2021)
P. Welsh et al.Lipoprotein(a) and cardiovascular disease: prediction, attributable risk fraction, and estimating benefits from novel interventionsEur J Prev Cardiol
(2022)
Wong N.D., Fan W., Hu X., et al. Lipoprotein(a) and long-term cardiovascular risk in a multi-ethnic pooled prospective...S.S. Virani et al.Associations between lipoprotein(a) levels and cardiovascular outcomes in black and white subjects: the Atherosclerosis Risk in Communities (ARIC) StudyCirculation
(2012)
W. Guan et al.Race is a key variable in assigning lipoprotein(a) cutoff values for coronary heart disease risk assessment: the Multi-Ethnic Study of AtherosclerosisArterioscler Thromb Vasc Biol
(2015)
G. Pare et al.Lipoprotein(a) levels and the risk of myocardial infarction among 7 ethnic groupsCirculation
(2019)
F. Kronenberg et al.Lipoprotein(a) in atherosclerotic cardiovascular disease and aortic stenosis: a european atherosclerosis society consensus statementEur Heart J
(2022)
M. Trinder et al.Clinical utility of lipoprotein(a) and LPA genetic risk score in risk prediction of incident atherosclerotic cardiovascular diseaseJAMA Cardiol
(2020)
N. Perrot et al.Genetic variation in LPA, calcific aortic valve stenosis in patients undergoing cardiac surgery, and familial risk of aortic valve microcalcificationJAMA Cardiol
(2019)
B.J. Arsenault et al.Association of long-term exposure to elevated lipoprotein(a) levels with parental life span, chronic disease-free survival, and mortality risk: a mendelian randomization analysisJAMA Netw Open
(2020)
Y.X. Cao et al.Lipoprotein(a) and cardiovascular outcomes in patients with previous myocardial infarction: a prospective cohort studyThromb Haemost
(2021)
S.C. Larsson et al.Lipoprotein(a) in Alzheimer, atherosclerotic, cerebrovascular, thrombotic, and valvular disease: mendelian randomization investigationCirculation
(2020)
P.E. Thomas et al.Lipoprotein(a) is linked to atherothrombosis and aortic valve stenosis independent of C-reactive proteinEur Heart J
(2023)
View full text© 2024 National Lipid Association. Published by Elsevier Inc. All rights reserved.
留言 (0)