
記住我


Osseous defects after orthopaedic trauma are often associated with poor viability of adjacent bone and a compromised soft tissue envelope. In addition, host factors such as age, medical comorbidities, and social factors become increasingly relevant when evaluating some of the various techniques for reconstruction. Distraction osteogenesis and the induced membrane (Masquelet) technique are particularly dependent on patient biology. In addition, distraction osteogenesis, whether performed with an external fixation device or medullary implant, requires the patient be strictly adherent to their prescribed lengthening schedule. Finally, periarticular bone remains particularly challenging to address.
The use of custom metallic implants offers unique benefits when evaluating the management of critical bone defects.1–4 First, as this is not a biologic reconstruction, the goal is incorporation of the metallic implant primarily at its bony interfaces so the total size, morphology, and location of the defect may not be as critical as it is when osseous regeneration is attempted. Next, although there are some various printed metallic structures used, these implants provide some degree of immediate structural support across the defect. Implants are usually used in conjunction with a medullary nail or plate and screw devices and the improved stability may facilitate earlier activity and weight-bearing. This all-internal solution and stability is also beneficial to the surrounding soft tissue envelope for healing. Finally, after custom implant placement and fixation, there is no schedule for adjustment of an external or internal device so reliance on patient compliance is dissimilar to many of the techniques used for distraction osteogenesis. In patients who desire limb salvage but refuse treatment with devices such as a circular fixator or techniques such as a vascularized fibula, an internal three-dimensional (3D)-printed implant may be an option.
Use of a metallic implant for a critical bone defect is unfamiliar for many orthopaedic traumatologists. Although osseous integration is desired at the bone–implant interface, and possible with any additional bone graft that is placed in/around the implant, this is not a true biologic reconstruction. This type of solution is more familiar to, and accepted by, orthopaedic oncologists after radical tumor resection but is often not considered by many orthopaedic traumatologists for bone defect management. The implications of this, especially as it relates to infection and osseous incorporation, are slightly different than those encountered with some of the other, more traditional, biologic reconstructions noted above.
INDICATIONS AND BENEFITSThe indications and use of custom 3D-printed metallic implants have increased in many orthopaedic subspecialties. Custom cages, augments, wedges, and cones are being used in joint arthroplasty, especially in the revision setting when there is bone loss.5–7 In orthopaedic oncology, the use of intercalary metallic implants after resection of large osseous segments has been described in multiple anatomic locations.8,9 In some instances, when the resection involves some or all of the articular surface, these implants can be combined with an arthroplasty component for joint reconstruction.10 In orthopaedic trauma, although biologic reconstruction remains the goal for most patients, nonbiologic reconstruction with metallic implants is an option for limb salvage with some specific advantages.
First, there is associated morbidity from each of the abovementioned biologic reconstructive options. Most surgeons will use some volume of autograft when performing this technique. There has been described donor site morbidity from harvest from the pelvis or long bone medullary canal, including (but not limited to) pain, hematoma formation, and iatrogenic fracture.11 Distraction osteogenesis can be performed using multiple orthopaedic devices. There can be morbidity with long-term use of external pins/wires and circular frames, especially on the surrounding soft tissues.12 In addition, if distraction is unsuccessful, additional bone grafting or skeletal stabilization procedures may be needed. Finally, harvest and use of a vascularized bone segment (1) requires access to a microvascular surgeon who will perform this technique, (2) may not be suitable for every defect because of location and nearby vascularity, and (3) is associated with both donor and recipient site complications.
Metallic implants can help provide immediate stability to the extremity. Most commonly, these implants are designed for use with an intramedullary implant.13 In the scenario of juxta-articular bone loss, these implants can be designed to accommodate screw fixation between the metallic implant and adjacent bone or in the more complex scenarios, may be fabricated with plate-like extensions that allow for additional points of fixation (Fig. 1). This is beneficial, especially in geriatric patients or end-segment lesions where the goal is immediate weight-bearing. Similarly, in scenarios where patient behavior or mental status may affect compliance, the ability to provide immediate stability across an osseous defect without waiting for graft incorporation or maturation may be advantageous.
 FIGURE 1.:
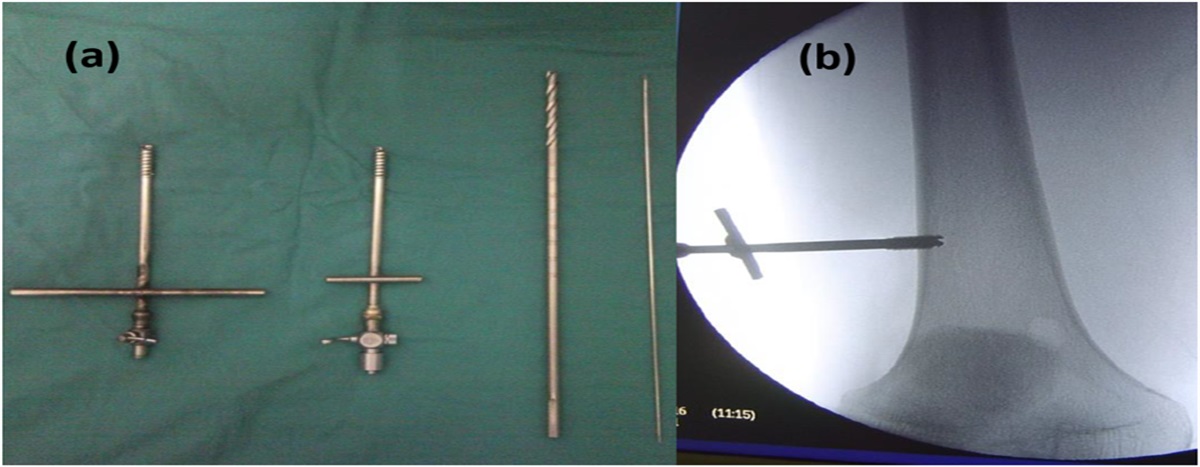
FIGURE 1.: A 30-year-old man presented with a persistent nonunion after multiple surgical procedures to his right distal tibia (A). A custom metaphyseal metallic implant was designed to fit a measured resection. The implant was designed to accommodate a medullary nail with additional distal phalanges for additional screw fixation (B). Final radiographs showing placement of custom metaphyseal implant with medullary rod (C).
A unique advantage of custom metallic implants is that after evaluation of the defect with a computed tomography scan of the affected area, as well as contralateral extremity (if available), the implant can be customized precisely to the exact size and shape of the defect.14,15 This can be extremely beneficial if the defect is irregular or if it would be beneficial to preserve a specific area of bone given soft tissue attachments or similar. If needed, cutting guides and instrumentation can also be made specifically for the procedure to ensure that implants fit exactly within the defect.
Unlike other biologic reconstructive options, metallic implants can also be customized in multiple different ways. The porosity and architecture of the implant can be designed for osseous ingrowth or allow for the addition of bone graft. The implant itself can be designed to be used with specific medullary nails, plates, screws, or suture for fixation or adjacent joint arthrodesis. If there is partial loss of articular cartilage, the implant can be designed to have a smooth joint-like surface that matches (or replaces) the remaining joint surface (Fig. 2). Similarly, implant locations can be polished to minimize muscle and tendon irritation with adjacent joint motion (Fig. 3). Neither of these options are available with free vascularized tissue transfer, distraction osteogenesis, or the induced membrane technique.
 FIGURE 2.:
FIGURE 2.: A 47-year-old morbidly obese (body mass index, 66) woman presented with a subacute right elbow fracture dislocation and unreconstructable capitellum (A). A custom metallic implant was designed to replace the capitellum and lateral column of the distal humerus (B). Final radiographs after measured resection and fixation of the custom joint hemiarthroplasty (C).
 FIGURE 3.:
FIGURE 3.: Design illustration of a distal fibular shaft custom implant designed for a patient with segmental bone loss. The implant was designed with a polished lateral surface to decrease peroneal tendon irritation, porous surface on medial face and on proximal and distal pegs, opportunities for nitinol staple fixation proximally, and transsyndesmotic fixation distally (A). Postoperative radiographs showing placement of custom metallic implant and intended points of fixation (B).
PERIOPERATIVE CONSIDERATIONS Availability and CostCurrently, custom metallic implants are available through a variety of manufacturers through the US Food and Drug Administration's custom device exemption. The cost of these implants is variable, depending on the size, shape, and degree of customization. This cost may include a backup implant or alternate size and oftentimes will include any specific cutting guides or instrumentation that is needed. One must also consider the additional cost of the orthopaedic plate or medullary nail that may be needed for stabilization across the defect.
It is important to note that the overall cost of custom implants continues to decrease as the technology improves and becomes more available. The number of orthopaedic device manufacturers who can produce such implants continues to increase. In addition, one must remember that management of complex critical bone defects is generally costly. Orthopaedic devices such as ring fixators or magnetic medullary devices are expensive. In addition, the additional hospital stays and surgical procedures that often accompany distraction osteogenesis (pin/wire exchange, docking site procedure, implant removal, etc.) may be greater than those that accompany use of a definitive metallic implant for a bone defect. Future cost analyses will help compare the cost of limb salvage techniques as more information and larger series are published.
Production TimeWhen considering use of a custom metallic implant for an osseous defect, staged reconstruction is necessary as time is required for design and fabrication of the implant. This time is variable but, in many instances, can be performed in as short as just a few weeks. Patients typically require computed tomography assessment of both the injured and noninjured sides to appropriately characterize the defect dimensions, map the contralateral uninjured anatomy, and assess the initial reduction and stabilization. In the scenario where length or alignment may not have been restored, the metallic implant can be designed to potentially correct these parameters and restore more accurate anatomy.
Soft TissueCustom metallic implants are designed to match the normal contour of the bone or any custom dimension necessary. In a segmental defect, this often is determined by digital planning software and is a distinct advantage of using a metallic implant. The soft tissue envelope surrounding the implant is very important and must be stable to avoid any wound healing complications after implantation. For this reason, most surgical procedures involving placement of these implants are staged procedures. As noted previously, ligament and tendons can also be incorporated into the reconstruction at the time of definitive surgery, an option that is not available for some of the other biologic reconstructions. Unfortunately, the ability to intentionally shorten or angulate the limb to allow for soft tissue closure does not exist. To be fair, this option does not exist with the induced membrane or vascularized osseous transfer either.
InfectionRegardless of the technique implemented for segmental defect reconstruction, infection is a primary concern. In trauma, bone loss is commonly the result of severe open fracture or chronic infection. Both are associated with significant complication risk at any point during their management. Infection after placement of a custom metallic implant can occur and the sequelae can be devastating. Removing the implant, revision surgical procedures and amputation are all possible if a deep infection occurs.
Comprehensive surgical debridement is critical to minimize the possibility of infection for these cases. Local antibiotic delivery can also mitigate infection and is implemented in the form of antibiotic-eluting cement spacers or beads placed into the open fracture site and osseous defect. There is no defined protocol, but a staged process to reconstruction with metallic implants allows for an observational period of 3–6 weeks between surgeries. During this time, patients are typically receiving local antibiotics through their spacer/beads that helps to further minimize the potential for infection. If these injuries are associated with significant soft tissue compromise or a reconstructive procedure is necessary, it is important to have a healthy soft tissue envelope over the implant. Given that any reconstruction with a metallic implant does not rely on the biologic activity of a membrane or similar, it is recommended that any concern or variable that may increase the risk of infection is addressed first.
CONCLUSIONSThe reconstruction of osseous defects poses a formidable challenge for orthopaedic surgeons regardless of approach for treatment. With the introduction of 3D printing technology, the use of patient-specific metallic implants is emerging as an increasingly formidable option for these injuries that may offer several potential surgical and patient benefits.
REFERENCES 1. Angelini A, Trovarelli G, Berizzi A, et al. Three-dimension-printed custom-made prosthetic reconstructions: from revision surgery to oncologic reconstructions. Int Orthop. 2019;43:123–132. 2. Mayfield CK, Ayad M, Lechtholz-Zey E, et al. 3D-printing for critical sized bone defects: current concepts and future directions. Bioengineering. 2022;9:680. 3. Meng M, Wang J, Huang H, et al. 3D printing metal implants in orthopedic surgery: methods, applications and future prospects. J Orthop Transl. 2023;42:94–112. 4. Westrick ER, Bernstein M, Little MT, et al. Orthopaedic advances: use of three-dimensional metallic implants for reconstruction of critical bone defects after trauma. J Am Acad Orthop Surg. 2023;31:e685–e693. 5. De Martino I, Strigelli V, Cacciola G, et al. Survivorship and clinical outcomes of custom triflange acetabular components in revision total hip arthroplasty: a systematic review. J Arthroplasty. 2019;34:2511–2518. 6. Berend ME, Berend KR, Lombardi AV, et al. The patient-specific Triflange acetabular implant for revision total hip arthroplasty in patients with severe acetabular defects: planning, implantation, and results. Bone Joint J. 2018;100-B:50–54. 7. Li Y, Wang X, Tian H. Reconstruction for massive proximal tibial bone defects using patient-customized three-dimensional-printed metaphyseal cones in revision total knee arthroplasty. Orthop Surg. 2022;14:1071–1077. 8. Guder WK, Hardes J, Nottrott M, et al. Highly cancellous titanium alloy (Tial6v4) surfaces on three-dimensionally printed, custom-made intercalary tibia prostheses: promising short-to intermediate-term results. J Pers Med. 2021;11:351. 9. Zhao D, Tang F, Min L, et al. Intercalary reconstruction of the “ultra-critical sized bone defect” by 3D-printed porous prosthesis after resection of tibial malignant tumor. Cancer Manag Res. 2020;12:2503–2512. 10. Liang H, Yang Y, Guo W, et al. Elbow hemiarthroplasty with a 3D-printed megaprosthesis for defects of the distal humerus or proximal ulna after tumour resection. Bone Joint J. 2022;104-B:747–757. 11. Oliva F, Migliorini F, Cuozzo F, et al. Outcomes and complications of the reamer irrigator aspirator versus traditional iliac crest bone graft harvesting: a systematic review and meta-analysis. J Orthop Traumatol. 2021;22:50. 12. Boksh K, Kanthasamy S, Divall P, et al. Hexapod circular frame fixation for tibial non-union: a systematic review of clinical and radiological outcomes. Strateg Trauma limb Reconstr. 2022;17:172–183. 13. Hou G, Liu B, Tian Y, et al. Reconstruction of ipsilateral femoral and tibial bone defect by 3D printed porous scaffold without bone graft: a case report. JBJS Case Connect. 2022;12:e20.00592. 14. Wong KC. 3D-printed patient-specific applications in orthopedics. Orthop Res Rev. 2016;8:57–66. 15. Zhou J, See CW, Sreenivasamurthy S, et al. Customized additive manufacturing in bone scaffolds—the gateway to precise bone defect treatment. Research. 2023;6:0239–325.
留言 (0)