
記住我



Despite the low incidence of CDC, they are relatively tricky to manage. For asymptomatic patients with small diverticular calculi, it can be observed conservatively and followed up regularly; for asymptomatic patients with certain requirements or special occupations (e.g., pilots), surgical treatment is also applicable [8]. When diverticular calculi cause lumbar pain, hematuria, and recurrent urinary tract infections, they should be managed surgically [6].
Currently, the main treatments for CDC include ESWL, F-URS, PCNL, and laparoscopic surgery. ESWL is a convenient and less-invasive procedure, but ESWL cannot dilate the narrow diverticular neck, fragmented stones are difficult to discharge from the diverticulum, and the recurrence rate of stones is high [3]. Turna et al. treated 38 patients with CDC by ESWL with a symptomatic relief rate of 61%, and only 8 patients (21%) had successful stone expulsion at a 3-month follow-up [3]. There was even a case of bacterial sepsis caused by CDC treated with ESWL has been reported in the literature [9]. In both our and previous studies, there were patients who first underwent ESWL but failed treatment and eventually chose F-URS to manage their stones [10, 11]. PCNL and F-URS are currently the most commonly used methods for the management of CDC. Literature reports that PCNL treatment of CDC has a stone clearance rate of 87.5–100%, a diverticulum closure rate of 76–100%, and symptomatic relief in more than 90% of patients at follow-up [6, 12]. In addition, after the removal of diverticular calculi, PCNL can mechanically dilate the diverticular neck to allow adequate drainage, or it can cauterize the mucosa of the diverticular cavity to promote its closure [13]. However, PCNL also has its limitations; for example, when dealing with small diverticula or diverticular calculi located in the upper and ventral calyces, due to the special location and angle of the puncture, it may cause serious complications, such as pleural, intestinal, and great vessel injuries [5, 6, 14]. Laparoscopy is appropriate for patients with diverticula located on the surface of the renal parenchyma and with thin renal parenchyma, but laparoscopic surgery is complicated and traumatic, and it is difficult to deal with diverticular calculi in the deeper part of the renal parenchyma, which restricts its wide application, and it is generally used as a complementary method to minimally invasive surgery [15].
Fuchs et al. made the first report on the use of F-URS for the management of CDC. Although intracavitary holmium laser lithotripsy was not available at that time, they successfully managed 15 cases of CDC with a stone-free rate of 73.3% by F-URS with electrohydraulic lithotripsy and ESWL [16]. In recent years, with the development of F-URS and holmium laser equipment and technology, F-URS with holmium laser has shown unique advantages in the management of CDC. First, F-URS utilizes the natural lumen of the human body, which has the advantages of less trauma, better healing, and faster recovery. Chen et al. reported that F-URS for the treatment of CDC achieved an initial surgical stone-free rate of 81.4% and a symptom relief rate of 90%. The overall stone-free rate was 93% after the second-stage surgery; the complication rate was 11.6%, all of which were minor complications (Clavien classification I–II) [11]. Bas et al. compared the efficacy of F-URS versus PCNL in the management of CDC. It was found that there was no significant difference between the two groups in terms of operation success rate, symptom relief rate, and stone-free rate (p = 0.537, p = 0.880, p = 0.539), but the incidence of major complications (Clavien III) was higher in the PCNL group [6]. Furthermore, the F-URS with holmium laser can incise the narrow diverticular neck, which completely solves the fundamental problem of diverticular neck stenosis and reduces the chance of stone residue and recurrence after surgery [14, 17]. Koopman et al. reported that 94% of patients had their diverticular neck successfully dilated or incised during F-URS treatment of CDC, with a postoperative stone-free rate of 90% [18]. In the current study, 92.6% of the 27 patients had their diverticular necks successfully incised for lithotripsy. Only 4 patients suffered minor complications postoperatively. The stone-free rate was 80% after initial surgery and 88% after second-stage treatment, which was like the results of Chen et al.’s research and reconfirmed the high efficiency and safety of F-URS with holmium laser management of CDC.
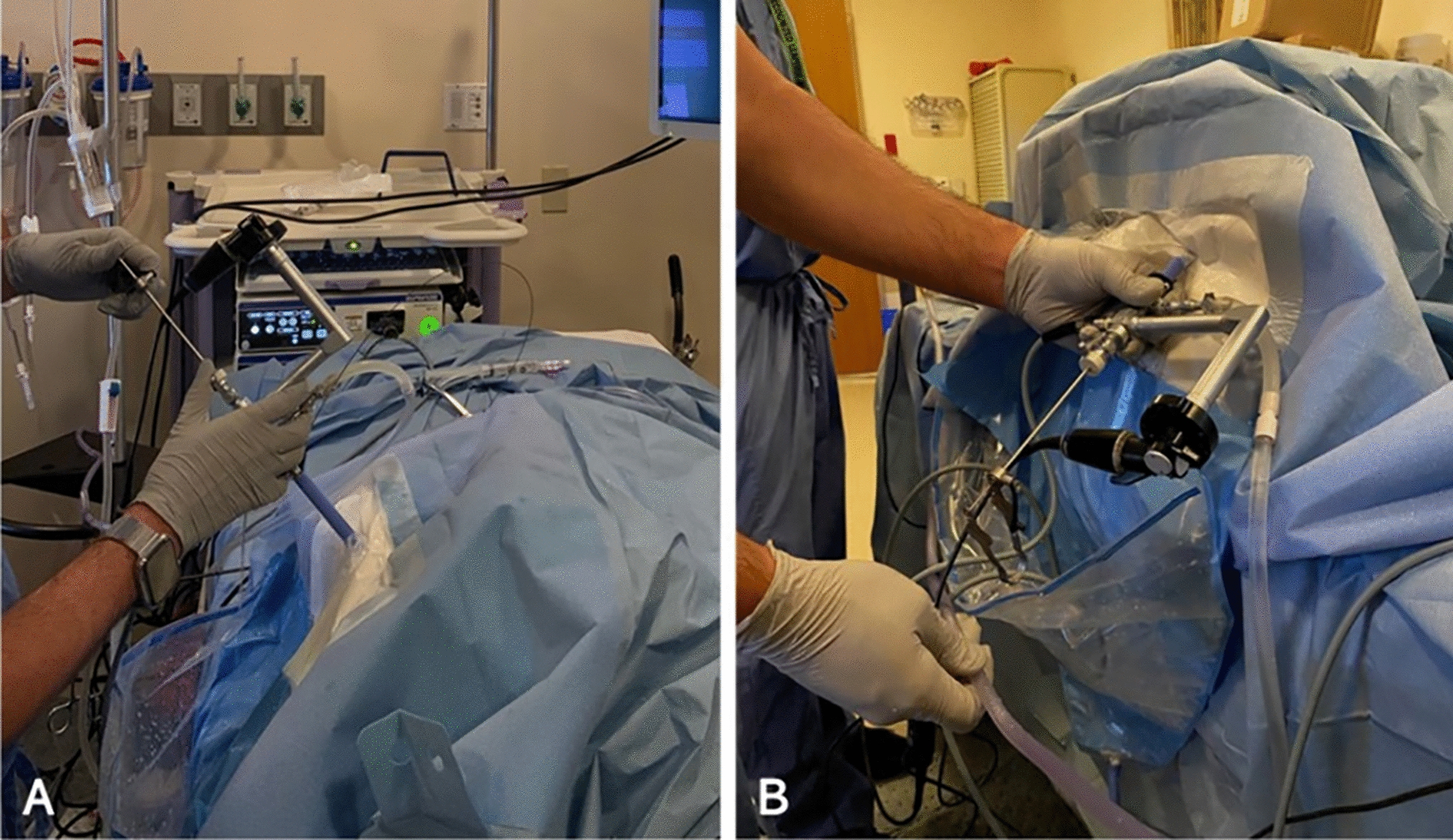
In theory, F-URS can treat all kidney calculi [4]. However, due to the limitations of infundibular pelvic angle (IPA), infundibular length and width of the lower calyx, and curvature of the end of the flexible ureteroscope, it was difficult to handle calculi in some diverticula of the lower calyx, and the stone-free rate was low [14]. Bas et al. found that the success rate of F-URS in the management of diverticular calculi of the lower calyx was only 60% influenced by the angle of deflection [6]. However, Sejiny et al. reported that although the efficacy of F-URS in treating calculi within the lower calyces diverticulum was lower than that of the upper and middle calyces, the difference between the three groups was not statistically significant (p = 0.369) [14]. Boonyapalanant et al. also found that the stone-free rate of F-URS treatment for CDC was not affected by the location of the diverticulum but affected by the size of the calculi and the length of the diverticular neck. They found that F-URS treatment of CDC with a stone size < 1.5 cm and a diverticular neck length < 0.4 cm achieved a high rate of stone clearance [13]. Chen et al. concluded that F-URS was appropriate for the management of CDC with large diverticular openings and short necks, but not appropriate for patients with slender diverticular necks or atresia diverticulum [11]. Our findings coincided with Sejiny’s as well as Boonyapalanant’s views. In our group, there were no statistically significant differences found in stone-free rates between the upper, middle, and lower calyx diverticula (p = 0.808). The 2 surgery failure cases both had slender diverticular necks, thick peri-neck renal parenchyma, and abundant blood supply. Concerned about bleeding after holmium laser incision, flexible ureteroscopic lithotripsy was not performed. Case 1 patient was admitted with lumbar pain, and the calculi were in the diverticulum of the right upper calyx with a diverticular neck length of about 6 mm. During the operation, a guide wire was used to probe the diverticular neck, and purulent urine was found to flow from the diverticular neck, but the patient refused to undergo PCNL. After the operation, the patient's lumbar pain was relieved (we considered that the patient's lumbar pain was relieved owing to the release of the diverticular neck obstruction during intraoperative guidewire exploration) (Fig. 2A–D), and he was discharged from our hospital. In another case, the calculi were in the middle calyx of the left kidney, and the diverticulum was found to have a small opening with a slender neck, so the ureteroscope could not enter the diverticulum, and the stone was successfully fragmented after PCNL.
Fig. 2
Preoperative and intraoperative imaging data of failed F-URS lithotripsy case 1. A CT coronal image shows that the stone was in the diverticulum of the middle calyx of the right kidney. The slender neck of the diverticulum (approximately 6 mm in length) was marked by the yellow arrow; B the diverticular neck opening; C guidewire exploration of the diverticular neck opening; D purulent fluid was seen flowing from the opening after removal of the guidewire
The key to F-URS treatment of CDC is the successful finding of the diverticular opening. We summarized several experiences: ① Preoperative ultrasonography, KUB + IVP, CT, CTU, and other relevant imaging examinations should be completed to identify the relationship between the diverticulum and the collecting system; ② F-URS should be performed as gently as possible to avoid intraoperative bleeding affecting the vision; ③ Maintain moderate perfusion pressure. In some cases with needle-like diverticular openings, an excessively low perfusion pressure makes it difficult to dilate the opening; an excessively high perfusion pressure increases the risk of urogenic sepsis; ④ For the suspected diverticular opening, insert a guidewire to explore, some cases can observe purulent urine flowing around the guidewire after insertion, and this sign can help us confirm that this is the diverticular opening; ⑤ If the diverticular opening cannot be found, try a methylene blue examination to look for it or look for it under ultrasound guidance. In addition, a successful and safe diverticular neck incision also appears to be extremely necessary. The following points should be noted during the incision process: ① When Holmium laser incises the diverticular neck, the energy parameter setting at low energy and high frequency (0.8–1.0 J/20–30 HZ) is recommended to have a better incision and hemostasis effect; ② The neck incision should be made along the thin mucosa of the diverticulum as much as possible and should be stopped when adjacent to thicker renal parenchymal tissue to avoid bleeding. The use of narrow band imaging (NBI) mode intraoperatively helps to identify the vascular distribution while not affecting the cutting procedure; ③ Under the premise of no bleeding, the diverticular neck incision should be large enough to enable the diverticulum to drain smoothly and prevent the stone recurrence after surgery; ④ Fragments within the diverticulum should be flushed out to the renal pelvis or adjacent calyces as far as possible to facilitate stone drainage; for lower calyces’ fragments, the Trendelenburg position can be used for flushing during the operation.
As for the management of CDC by F-URS, we believe that there are still many issues that need to be addressed. At first, most scholars believed that the diverticular lining should be fulgurated when CDC is treated with PCNL, resulting in collapse and closure of the diverticular cavity to prevent the recurrence of stone [12, 19]. Kim et al. reported that after intraoperative fulgurate through PCNL, all diverticula were reduced in size and 87.5% of diverticula disappeared at 3 months of follow-up [19]. Several existing studies have reported a high rate of stone-free during F-URS for the management of CDC but did not include factors such as whether the stones recurred after the operation and whether the diverticulum was closed [10, 11, 14]. Compared to PCNL, F-URS with holmium laser can sufficiently incise and drain the diverticular neck; therefore, whether it is necessary to close the diverticulum by fulguration needs further study. In addition, there is no consensus on whether the proximal end of the double J tube needs to be placed in the diverticulum after lithotripsy. Boonyapalanant et al. suggested that placing a double J tube into the renal calyces can provide drainage support, facilitate stone removal, and prevent restenosis of the diverticular neck [13]. Of the 25 patients successfully lithotripsy under F-URS in this study, 9 cases had the proximal end of the double J tube placed in the renal pelvis and 16 cases had the proximal end of the double J tube placed in the diverticulum, and no statistically significant difference was found in the stone-free rate comparing the two groups (p = 0.312) (Table 3). It can be seen that the placement of the double J tube does not affect the stone-free rate as long as the diverticular neck is adequately incised by the F-URS with holmium laser. Unfortunately, we did not follow up on the recurrence of diverticular neck stenosis. It is certain that when placing the guidewire, the position and depth of the tip of the guidewire must be clearly defined under the direct view of the flexible ureteroscope, thus avoiding the tip of the guidewire to penetrate the renal parenchyma, which may lead to double J tube ectopia. In the case of a postoperative subperitoneal hematoma in our group, the guidewire was not placed under direct view of the flexible ureteroscope, and the postoperative examination revealed that the double J tube penetrated the renal parenchyma in the diverticular dome, with the tip located under the peritoneum, and caused a subperitoneal hematoma. Due to the special anatomical location of the diverticula, most of the renal parenchyma in the diverticular dome is thin, which increases the probability of guidewire penetration into the renal parenchyma, and this case also provides experience for our following work.
Table 3 Association of different variables and stone-free rate (n = 25)
留言 (0)