
記住我




This randomized controlled trial was conducted using a pretest-posttest design in 2021. The study was registered in the Iranian Registry of Clinical Trial (IRCT# IRCT20131112015390N7).
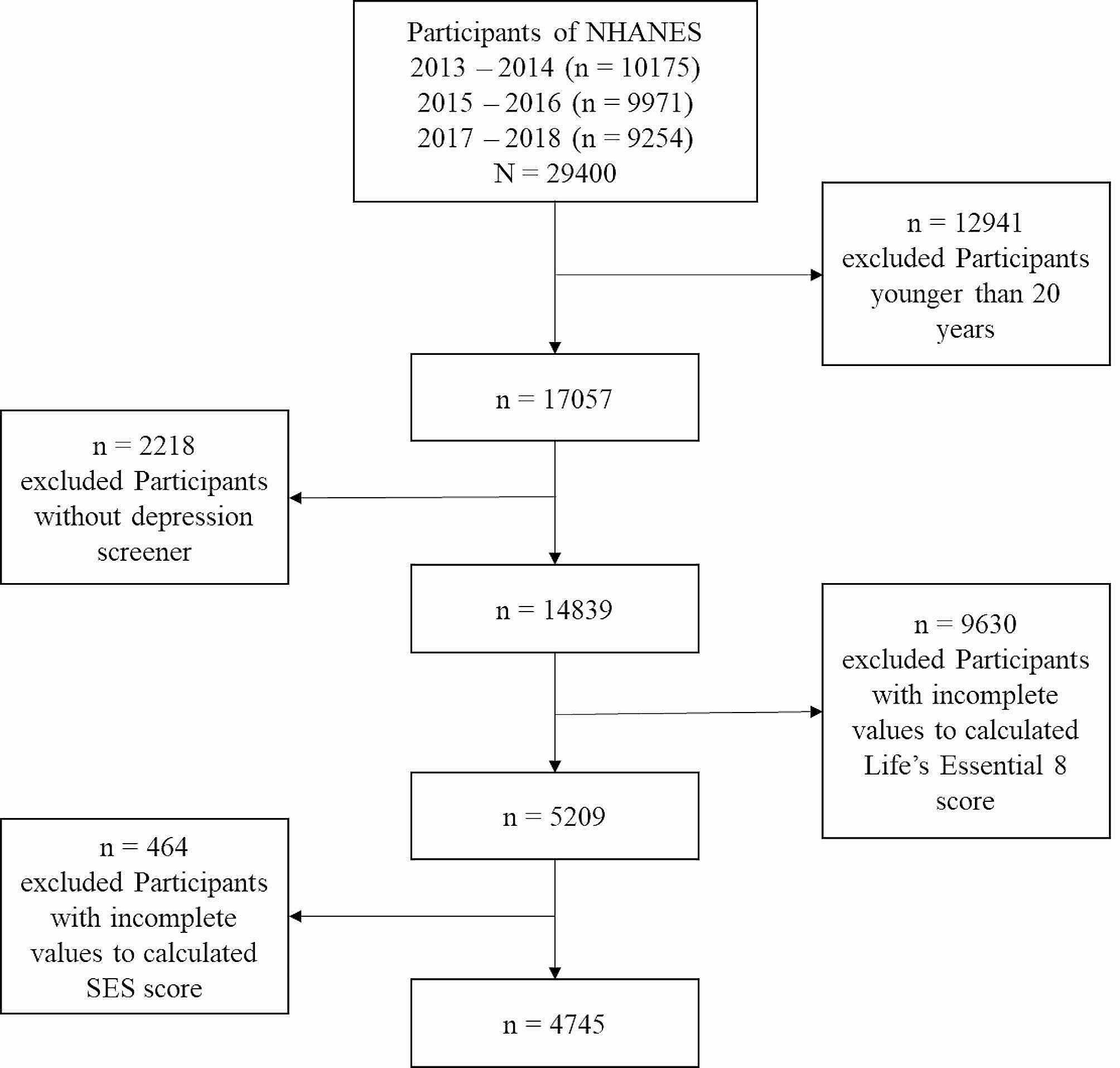
Study setting and samplingThe participants included patients with MDD who were referred to Razi Hospital (in Urmia, West Azerbaijan) and the Psychiatry Clinic of Madani Hospital (in Khoy, West Azerbaijan) in Iran. Considering the data provided in a study by Collins et al. (2020) [24], the initial sample size was determined to be n = 32 for each group.
After obtaining approval from the Research Ethics Committee of Urmia University of Medical Sciences, the researcher visited the determined study settings and granted the introduction letter to their authorities. Sixty-four patients diagnosed with MDD in the past year who met the inclusion criteria were recruited to participate in the study using convenience sampling. The inclusion criteria consisted of the following: (a) willingness to participate in the study, (b) being able to use a smartphone, install the application, and work with it, (c) being diagnosed with MDD according to DSM-5 criteria, (d) being literate, and (e) not being hospitalized. The exclusion criteria included the following: (a) unwillingness to continue participation in the study and (b) being hospitalized during the study.
RandomizationAfter obtaining the written informed consent and providing the necessary information about the study, the participants were randomly assigned to control and intervention groups using the simple randomization method. A pack of cards was used for random assignment, where patients who met the eligibility criteria selected either card A or B from the pack. Patients who selected card A were assigned to the control group, while those who picked card B were assigned to the intervention group.
The procedureThe Yara application was installed on the smartphones of the patients in the intervention group, and the researcher provided necessary instructions on how to use it during a justification session in the hospital conference room. The process of using the application was thoroughly taught to the patients. The leading researcher evaluated the patients' understanding and use of the application. Each patient logged into the application in the researcher's presence and used its different parts. All questions and concerns of patients about how to use the application were answered. Compliance with the use of the application was monitored by the option of sending an email to the researcher. Every time the patient logged into the application; an email was automatically sent to the researcher. Necessary information about anxiety, sleep quality, suicidal thoughts, and how to complete the questionnaires was provided to both groups. The questionnaires were completed before and after the intervention in the researcher's presence. The intervention was conducted using the Yara application for three months (February – April 2022). The patients in the control group only received routine care for three months. Routine care received by patients of both groups included doctor visits, medication prescriptions, and psychiatric consultations once a month. The consultation usually takes about 30 minutes.
Smartphone application (Yara)Due to the popularity of smartphone applications in managing chronic diseases, the lack of consistent results in their application, and especially the emergence of COVID-19, the research team decided to design and use a new smartphone application for patients with depression. With the cooperation of a computer software programmer, the researcher designed the Yara application. At first, the researcher designed the application's content under the supervisor's supervision, using reliable psychology sites and reliable books and following the examples of good existing applications. The app's content includes a daily exercise educational video to increase the client's physical activity, morning meditation exercise, a yoga video for bedtime, and standard wordless soothing music from nature that helps the client to fall asleep more easily. It helps to increase the quality of sleep; several authentic personal development books available in PDF format can help change the client's attitude towards life, and a section that includes three tests for the daily report of patients' sleep quality, suicidal thoughts, and anxiety. In this application, the client receives motivational sentences daily and records her daily activities. The client reports daily anxiety, sleep quality, and suicidal thoughts in the application on the page related to each parameter and receives an automatic solution. Then, the software was designed and built attractively. Every time the client uses the application, an email is sent to the researcher to ensure that the client complies with the use of the application. The patient will be contacted if the patient does not use the application for two consecutive days. The researcher will access this data in the application after completing the intervention. (Fig. 1)
Fig. 1
Images of the Yara smartphone application
To check the validity and reliability of the Yara application, ten experts from different fields were used, including two psychiatrists, two psychiatric mental health nurses with Ph.D. degrees, two computer and software engineers, two psychologists, and two musicologists. Validation was done by the Delphi method. The designed smartphone application and the thesis proposal were installed on the professors' smartphones. After a week of evaluation, the lead researcher took their comments and suggestions and applied the requested changes. After the changes, it was again re-checked by the professors and approved. Then, the application was installed on five patients with depression, and it was confirmed in terms of face validity and comprehensibility. After ensuring the validity and correctness of the application, it was checked by the ethics committee, and after its approval, it was given to the intervention group.
Data collectionIn this study, data were collected using a demographic questionnaire (age, gender, marital status, education, and job status), the Spielberger State-Trait Anxiety Inventory (STAI), the Pittsburgh Sleep Quality Index (PSQI), and the Beck Scale for Suicidal Ideation (BSSI).
The STAI is used to measure anxiety levels. This inventory consists of two parts. The first assesses the individual's state anxiety (situational anxiety) and contains 20 questions on a 4-point Likert scale (Not at all = 1, somewhat = 2, moderately = 3, Very much so = 4). The second part assesses the individual's trait anxiety and consists of 20 questions on a 4-point Likert scale (Almost never = 1, Sometimes = 2, Often = 3, Almost always = 4). Finally, scores for both parts (state and trait) are separately calculated and recorded as a score between 20 and 80 for each individual. Patients' anxiety levels were categorized based on their scores, ranging from mild to severe anxiety. Spielberger et al. (1983) reported Cronbach's alpha coefficients for the state and the trait part of the inventory to be 0.92 and 0.90, respectively. The test-retest reliability coefficients for the state and the trait part were also calculated as 0.62 and 0.68, respectively [25]. In studies conducted to investigate the validity and reliability of this inventory in Iran, its reliability and validity coefficients were reported to be 0.91 and 0.90, respectively. Accordingly, the STAI was indicated to have high levels of validity and reliability in the Iranian population [26]. In this study, the scale's reliability was confirmed in a pilot study with Cronbach's alpha coefficient of 0.92.
The BSSI was developed by Aaron Beck in 1961. This scale consists of 19 items and is scored on a three-point Likert scale ranging from "Not at all true = 0" to "Definitely true = 2". The sub-scales include five questions about the desire to die, seven questions about readiness for suicide, and five questions about actual suicide intent. Questions 18 and 19 are not included in the scoring. The individual's total score ranges from 0 to 38 and is calculated by adding the scores. Scores of 0-5 indicate suicidal ideation; scores of 6-19 indicate suicidal readiness; and scores of 20-38 indicate suicidal intent. The BSSI has been shown to have correlation coefficients ranging from 0.90 to 0.94 with standardized tests for depression and suicidal tendencies. The BSSI has also been indicated to have a correlation coefficient ranging from 0.64 to 0.75 with the Beck Depression Inventory and the Beck Hopelessness Scale. The reliability of the BSSI was assessed using the internal consistency and the test-retest reliability method, based on which its Cronbach's alpha coefficient was obtained from 0.87 to 0.97, and its test-retest reliability coefficient was calculated to be 0.54 [27]. In Iran, the BSSI was validated in a study conducted on soldiers by Anisi et al. (2005) with a concurrent validity coefficient of 0.76 and Cronbach's alpha coefficient of 0.95 [28]. A pilot study confirmed the scale's reliability with Cronbach's alpha coefficient of 0.91 in this study.
The PSQI was first developed by Dr. Buysse at the Pittsburgh School of Medicine in 1989. This tool consists of 18 items, all scored on a 4-point Likert scale ranging from 0 to 3. The questionnaire has seven sub-scales, including subjective sleep quality, sleep latency, sleep duration, sleep efficiency, sleep disturbance, use of sleep medication, and daytime dysfunction. To score the PSQI, participants must first assign one of three scores to each of the 18 items. A total score of higher than 5 indicates poor sleep quality. The internal consistency of this tool was approved with a Cronbach's alpha coefficient of 0.83, and its validity was reported to be appropriate by the scale developers, with a sensitivity of 89.6% and specificity of 86.5% [29]. In this study, the tool's reliability was approved in a pilot study with a Cronbach's alpha coefficient of 0.89.
Data analysisData were analyzed in IBM SPSS Statistics for Windows, version 22 (IBM Corp., Armonk, N.Y., USA). The frequency of characteristics was presented as number (%), and quantitative results as mean (±standard deviation), independent t, paired t, Mann-Whitney U, and Wilcoxon tests were performed to analyze data. All p values were two-tailed, and the significance level was considered as p < 0.05 (Fig. 2).
Fig. 2
Flow chart of research implementation
留言 (0)