
記住我


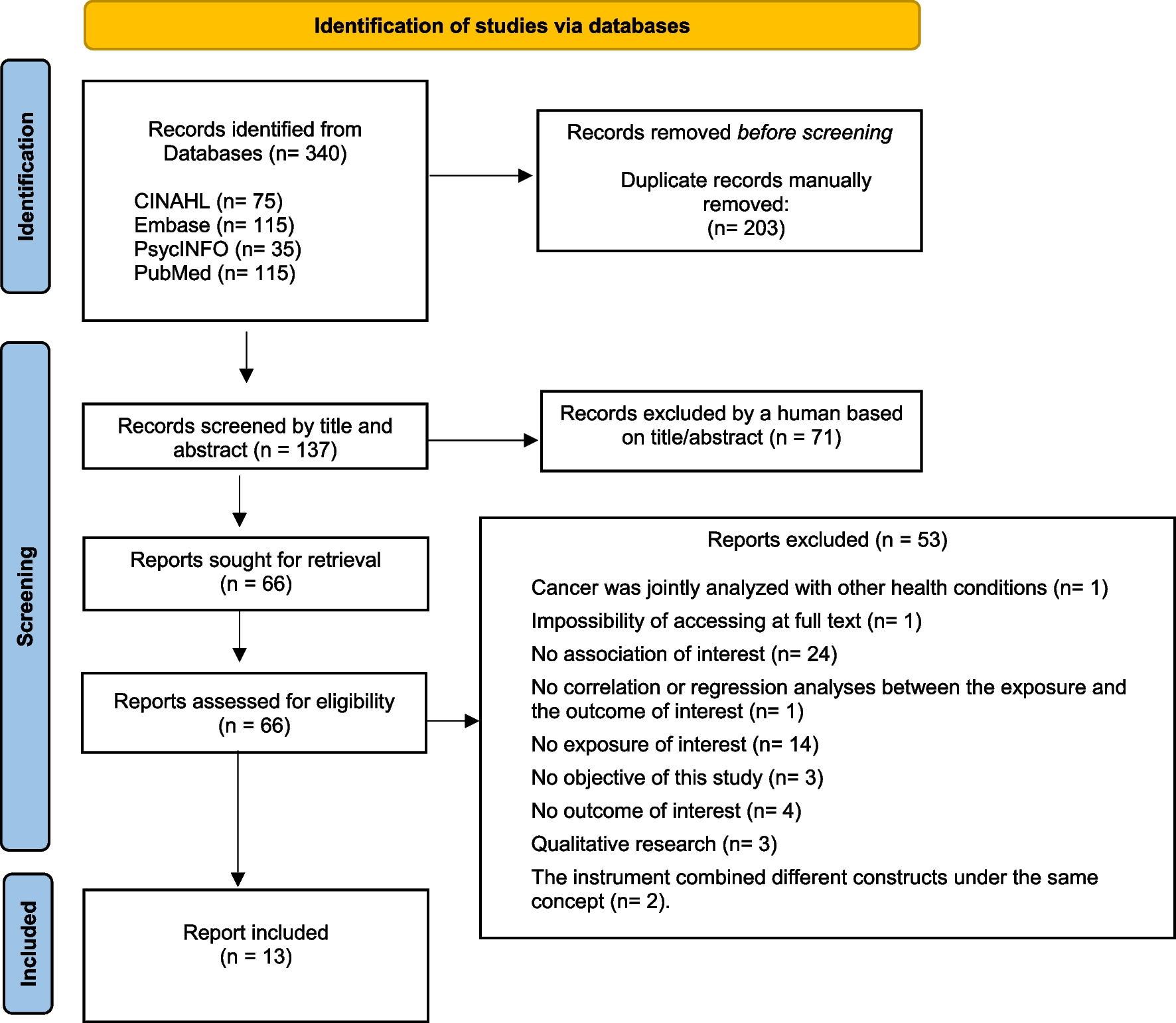
A total of 4576 results were produced from the database search. After screening by title/abstract, 80 full-text articles were reviewed resulting in 35 eligible studies (Fig. 2), including seventeen qualitative, fourteen quantitative, and four mixed or multi-method study designs, summarized in Table 1. In most studies, the term “parent” was an overarching term, which included biological parents or other caregivers. The studies were conducted in 11 different countries with parents of children with a variety of types of cancers. Only ten of the studies reported the race and ethnicity of the child or the parent. Results were categorized following the Adapted Parent Experiences of School Integration Support Model [11].
Fig. 2
Source: Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. https://doi.org/10.1136/bmj.n71
Table 1 Study characteristicsHealthcare providersSixteen of the included studies discussed parent experiences with communication, knowledge, and process of receiving support from healthcare providers.
CommunicationStudies reported parent–healthcare professional communication about child neurocognitive needs. There was limited communication from the oncology team on the child’s neurocognitive needs. Many parents reported that they did not receive communication about future treatment-related neurocognitive challenges from their oncology team [11, 46]. Thornton et al. found that fewer than half of parents (49%) had conversations regarding the neurocognitive effects of therapy with primary care providers at every visit, and 12% reported never having these conversations [52]. However, parents did report receiving communication from neuro/psychologists, if referred for these services by the oncology team. Parents described written reports from the neuro/psychologist as a method of clear communication about their child’s neurocognitive needs. Parents in both qualitative and quantitative studies found that the reports were written in easily understandable language that included “laymen’s terms” and clear explanations of complex terminology [21, 38].
KnowledgeThe neuropsychological report increased parent knowledge of available supports, such as specific assistance and accommodation strategies, as well as general knowledge about their child’s needs [11, 38]. In contrast, parents reported receiving limited information from the oncology team. Parents did not feel the oncology team fully comprehended or divulged the non-health aspects of school integration challenges, such as legal rights to educational access or additional resources to address learning difficulties [11, 46, 52]. Ruble et al. [46] reported that parents desired additional information on non-health aspects of school integration from their child’s oncology team but were rarely provided with this information.
ProcessParents frequently described their experience with neuropsychology evaluations [21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47] and found it to be an effective resource during the transition to school [21, 38]. Parents in a qualitative study completed in the USA reported that the neuropsychological reports lent authority to and helped establish validity for their requests for additional academic support [11]. Parents also described meetings with other healthcare professionals during their child’s transition to school, including physical and occupational therapists [33, 41], speech therapists [41], and psychologists [47, 33]; however, it was not clear from these studies whether these meetings with other providers were beneficial for school integration.
Parents reported desiring support from healthcare providers during the transition to school [40, 29]. However, they tended to find support from healthcare providers unsatisfactory or completely lacking [38, 47, 29, 27]. Regarding the support that did exist, parents reported that psychologists needed to provide more psychosocial support and guidance to parents [47], referrals from other healthcare providers to neuro/psychologists were infrequent [38], they felt abandoned by the oncology team after the completion of treatment [29], and that the healthcare team should provide education to school faculty on their child’s illness [40, 29]. Additionally, the timing of information received from healthcare providers was unhelpful — the information provided was too much all at once, and too early during the child's illness [46, 21].
School faculty and systemTwenty-five studies discussed parent experiences with school faculty or the school system, including communication with school faculty, school faculty knowledge, and the process of receiving support from school faculty and accessing resources in the school system.
CommunicationThere was a range of both negative and positive experiences with parent–school faculty communication. Parents who described negative experiences felt burdened with the responsibility of monitoring their child’s progress [11], reminding school faculty of their child’s needs [21, 38, 19], and taking the initiative to educate school faculty on their child’s illness [24]. Across studies, parents reported that teachers needed frequent reminders regarding their child’s needs and ongoing communication to get the appropriate support in place for their child [11, 21, 38, 19, 23]. Unfortunately, parents also perceived that teachers may not take their child’s needs seriously unless a healthcare provider communicated this information [25], which may be due to survivors not physically appearing to have a disability [19]. Some studies described fragmented communication. Many parents experienced the lack of a formal or systematic way for teachers to share information on their child’s needs. Particularly, systematic communication was lacking between teachers associated with a change in the child’s grade level and with parents regarding their child’s progress in school [11, 21, 33, 32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48].
Parents also reported positive experiences with teacher communication. One study reported frequent parent conversations with school faculty [37]. Other studies described that frequent communication and earlier identification of child needs may be facilitated through strong parent–teacher relationships [32, 26]. Positive experiences were also facilitated by communication and collaboration among teachers [27, 26]. In contrast to the barrier presented by fragmented communication, parents reported that it was helpful when teachers had a systematic method for identifying and sharing information about their child’s school needs. McLoone et al. [26] discussed that parents in Australia found it helpful when teachers placed their child’s photograph and a brief description of their school needs on the staff room notice board. Soejima et al. [51] reported positive experiences were further facilitated by teacher–child communication for parents in Japan; encouragement of the child by the teacher facilitated a positive experience for the child and in turn the parent [51].
School faculty–healthcare provider communicationParents reported few instances of communication between school faculty and healthcare providers. Three studies found that parents appreciated when hospital outpatient clinics and nurse coordinators interacted with the school through in-person visits and establishing communication pathways [21, 19, 25]. Parents felt it was important for healthcare professionals to educate school faculty and student–peers about the child’s disease and its consequences [21, 40, 29, 31]. Parents struggled when they had to act as communication intermediaries, as they did not always feel confident explaining their child’s neurocognitive and other medical issues [11, 33, 31].
KnowledgeParents reported lower confidence in teachers’ knowledge about cancer and its impacts on schooling. Many parents described that their child’s teachers lacked an understanding of long-term cancer treatment effects and how treatment may influence school performance [11, 19, 25, 32, 48, 18]. Teachers’ understanding of long-term treatment effects on schoolwork was an important facilitator in parents receiving transition support in Japan [51]. Parents attributed low teacher understanding to a limited expertise in healthcare, lack of knowledge concerning treatment effects, and their child’s absence of an outward appearance of being disabled [19, 25, 32]. In two studies, parents of survivors in the USA noted teachers appeared nervous or uncomfortable with having a survivor in the classroom due to a lack of understanding concerning their needs [11, 18].
ProcessParents reported experiences accessing resources during school integration. One resource was formal education support, to which parents reported limited access. Many parents struggled with obtaining and understanding the components of formal education support (Individualized Education Program or IEPs and 504 plans) and other accommodations within the classroom [11,
留言 (0)