
記住我










Abdominal aortic aneurysm (AAA) refers to the dilation of the abdominal aorta with a diameter greater than 3 cm (1, 2). It is more common in male smokers over the age of 65 years and other risk factors include dyslipidemia, hypertension, and other common risk factors for cardiovascular diseases (3, 4). Endovascular aortic aneurysm repair (EVAR) has become the main treatment for AAA due to its minimally invasive nature, excellent short-term and acceptable long-term prognosis (5). Endoleak is a common complication after EVAR, which refers to the continuous blood flow in the aneurysm sac after EVAR. Type I endoleak refers to incomplete sealing of the proximal aortic attachment site (IA) or distal iliac artery attachment site (IB). Type II endoleak is defined as the continuous filling of the aneurysm sac by the patent lumbar artery or inferior mesenteric artery, type III endoleak occurs when there is incomplete seal between components or component separation (6–8).
Dyslipidemia is common in patients with AAA. A previous study has shown that total cholesterol (TC) and low-density lipoprotein cholesterol (LDL-C) play a role in the pathogenesis of AAA (9). Patients with small-diameter AAA may benefit from treatment that reduces LDL-C (10). High-density lipoprotein (HDL) reduction and dysfunction are also related to AAA formation (11). Dyslipidemia also affects the surgical treatment of AAA. A study pointed out that type II endoleak after EVAR for AAA is associated with dyslipidemia (12). However, there is still insufficient research on the impact of dyslipidemia on the postoperative outcomes of patients with AAA after EVAR.
Therefore, we conducted a retrospective study to screen patients with AAA with concomitant dyslipidemia and explore the impact of dyslipidemia on EVAR.
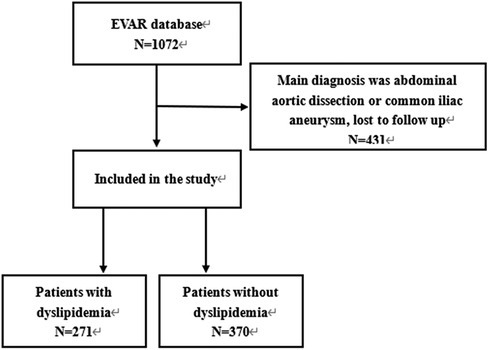
Methods PatientsThe medical records of 1,072 patients who received EVAR between 2010 and 2020 in our hospital were reviewed, and all patients with AAA who underwent EVAR were included, except for cases with: (1) The follow-up time less than three years or follow-up was lost; (2) The main diagnosis being abdominal aortic dissection or common iliac artery aneurysm. Finally, as shown in the Figure 1, 641 patients with AAA were included, and all patients were followed up by outpatient clinics or telephone for at least 3 years. The patients were divided into dyslipidemia and non-dyslipidemia groups based on whether they had dyslipidemia before EVAR. This study was approved by the ethics committee of West China Hospital, Sichuan University, the approve number was 20221827. The requirement for informed consent was waived due to de-identified patient information.
Figure 1. Patients inclusion and exclusion.
Data collectionWe collected the anatomical parameters of AAA, including neck angle, neck length, and maximum diameter, by comparing contrast-enhanced computed tomography and angiography. We collected the surgical records and baseline characteristics of each patient through an electronic medical record system, including age, sex, underlying disease, and smoking history. We obtained the occurrence of death and major adverse cardiovascular and cerebrovascular events (MACCEs) through outpatient clinics or telephone calls and assessed stent-related complications using ultrasound or computed tomography angiography of the abdominal aorta. All patients were followed up at 1, 6, and 12 months after EVAR and once a year thereafter. Dyslipidemia was defined as a large range of lipid abnormalities or their combination of increased TC ≥ 6.20 mmol/L, LDL-C > 4.13 mmol/L, and triglyceride (TG) levels >2.25 mmol/L or decreased HDL-C < 1.03 mmol (13). We collected blood samples from all patients after fasting for 12 h to detect lipid levels based on the lipid levels of the local population and defined dyslipidemia as the presence of any of the following criteria: (1) Blood TG level of >1.83 mmol/L; (2) Blood TC level of >5.70 mmol/L; (3) Blood LDL-C level >4.0 mmol/L; (4) Blood HDL-C level <0.90 mmol/L, or a combination of these features. Stent-related complications included endoleaks, stent displacement, and stent occlusion. Type I endoleak includes type Ia and type Ib endoleaks, while type II includes transient and persistent endoleaks. MACCEs include newly developed coronary artery disease (CAD), myocardial infarction (MI), and stroke after EVAR. Aneurysm-related death was defined as death within 30 days of EVAR or death associated with stent-related complications.
Stent-related complications were the primary outcome, and secondary outcomes included MACCEs and all-cause mortality.
Statistical analysisStatistical analysis was performed using SPSS, version 25, IBM. Continuous variables were represented as mean ± standard deviation (X ± SD) and compared using independent sample t-tests or Mann–Whitney U-test. The categorical variables were expressed as percentages and compared using χ2 tests. Endpoint events were analyzed using Kaplan–Meier survival curves. Cox regression model was used to evaluate the impact of each predictive factor on outcomes, we selected predictive factors with a univariate analysis P-value <0.1 for multivariate analysis to assess the independent effect of each predictor. Two-sided P < 0.05 was considered statistically significant.
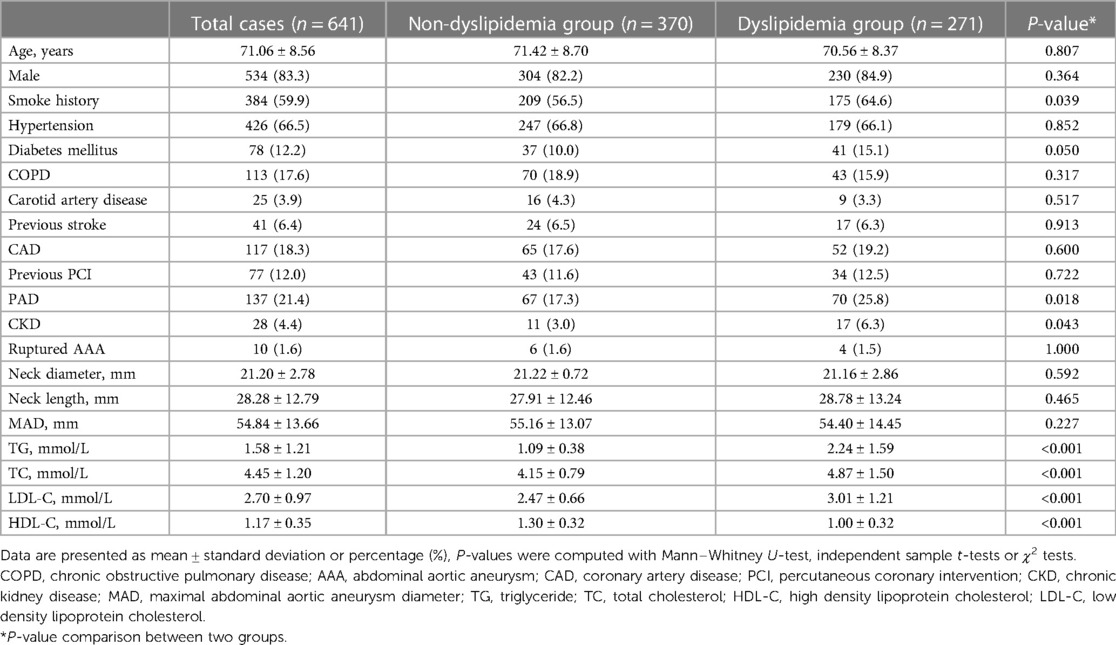
Results Baseline characteristicsAs shown in Table 1, 271 (42.3%) of the 641 patients with AAA had concomitant dyslipidemia. The average age of patients with AAA was 71.06 ± 8.56 years old, with male patients accounting for 82.3%. Patients in the dyslipidemia group had a higher smoking history rate (56.5% vs. 64.6%, P = 0.039). There was no statistically significant difference in the rates of hypertension (66.8% vs. 66.1%, P = 0.852), chronic obstructive pulmonary disease (18.9% vs. 15.9%, P = 0.317), carotid artery disease (4.3% vs. 3.3%, P = 0.517), previous stroke (6.5% vs. 6.3%, P = 0.913), CAD (17.6% vs. 19.2%, P = 0.600), and previous percutaneous coronary intervention (11.6% vs. 12.5%, P = 0.722) between the two groups. The prevalence of diabetes (10.0% vs. 15.1%, P = 0.050), peripheral arterial disease (17.3% vs. 25.8%, P = 0.018), and chronic kidney disease (CKD) (3.0% vs. 6.3%, P = 0.043) was higher in the dyslipidemia group than in the non-dyslipidemia group. There was no significant difference in anatomical parameters such as neck diameter (21.22 ± 0.72 vs. 21.16 ± 2.86, P = 0.869), neck length (27.91 ± 12.46 vs. 28.78 ± 13.24, P = 0.278), and maximum diameter of the AAA between the two groups. The plasma TG (1.09 ± 0.38 vs. 2.24 ± 1.59, P < 0.001), TC (4.15 ± 0.79 vs. 4.87 ± 1.50, P < 0.001), and LDL-C (2.47 ± 0.66 vs. 3.01 ± 1.21, P < 0.001) of patients in the dyslipidemia group were significantly higher than those of non-dyslipidemia group, while HDL-C (1.30 ± 0.32 vs. 1.00 ± 0.32, P < 0.001) was significantly lower in the dyslipidemia group.
Table 1. Baseline of characteristics.
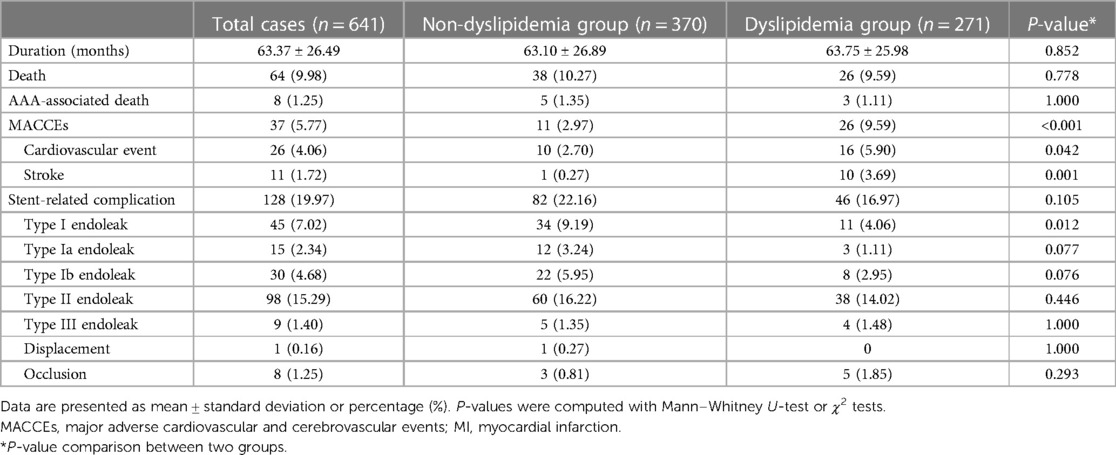
Follow-up outcomesAs shown in Table 2, all patients were followed up for more than three years, with an average follow-up time of 63.37 ± 26.49 months. There was no difference in follow-up time between the two groups (63.10 ± 26.89 vs. 63.75 ± 25.98, P = 0.760).
Table 2. Three-year follow-up outcomes.
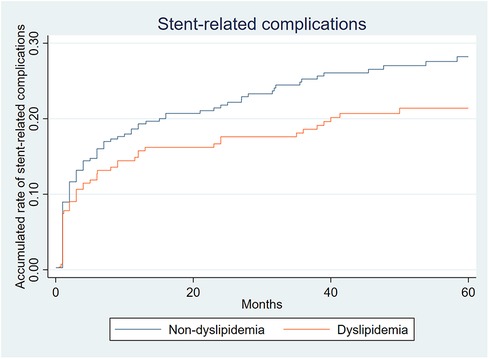
Stent related complicationsA total of 128 (19.97%) patients experienced stent-related complications, including 82 (22.16%) in the non-dyslipidemia group and 46 (16.97%) in the dyslipidemia group. Among all complications, the incidence of type II endoleak was the highest (98/641, 15.29%), and its incidence between the two groups was comparable (16.22% vs. 14.02%, P = 0.446). This was followed by type Ib endoleak (30/641, 4.68%) with comparable incidence between the two groups (5.95% vs. 2.95%, P = 0.076). Only nine type III endoleaks were observed, and there was no difference in the incidence between the two groups (1.35% vs. 1.48%, P = 1.00). A total of 45 (7.02%) type I endoleaks were observed, and the incidence of type I endoleaks in the dyslipidemia group was lower than that in the non-dyslipidemia group (9.19% vs. 4.06%, P = 0.012). After observing the simultaneous occurrence of various types of endoleaks in some patients, 152 endoleaks were noted. One stent displacement and eight iliac branch occlusions were observed. There was no significant difference in the rate of stent-related complications (22.16% vs. 16.97%, P = 0.105) between the two groups, except for type I endoleak. However, as shown in Figure 2, the incidence of stent-related complications in the non-dyslipidemia group was slightly higher than that in the dyslipidemia group.
Figure 2. Accumulated rate of stent-related complications.
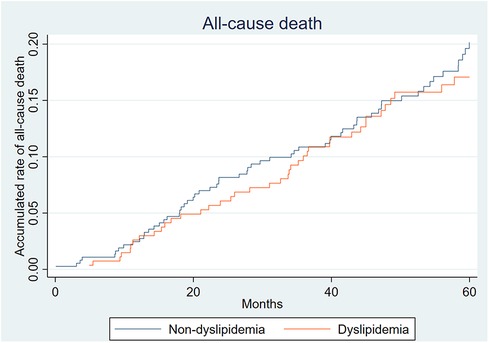
MortalityThe all-cause mortality rate 3 years after EVAR was 9.98% (64/641). The rate of aneurysm-related death was 1.23% (8/641). From Figure 3, it can be seen that the all-cause mortality rates of the two groups were similar. There was no significant difference in all-cause mortality between the two groups (10.27% vs. 9.59%, P = 0.778).
Figure 3. Accumulated rate of all-cause death.
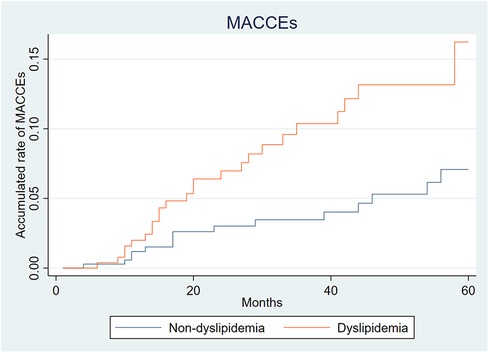
MACCEsA total of 37 (5.77%) MACCEs were observed within 3 years, including 26 cardiovascular events and 11 strokes. The incidence of MACCEs (2.97% vs. 9.59%, P < 0.001) in the dyslipidemia group were higher than that in the non-dyslipidemia group. Moreover, as shown in Figure 4, the difference in the incidence of MACCEs between the 2 groups gradually increased within 3 years after EVAR.
Figure 4. Accumulated rate of major adverse cardiovascular and cerebrovascular events (MACCEs).
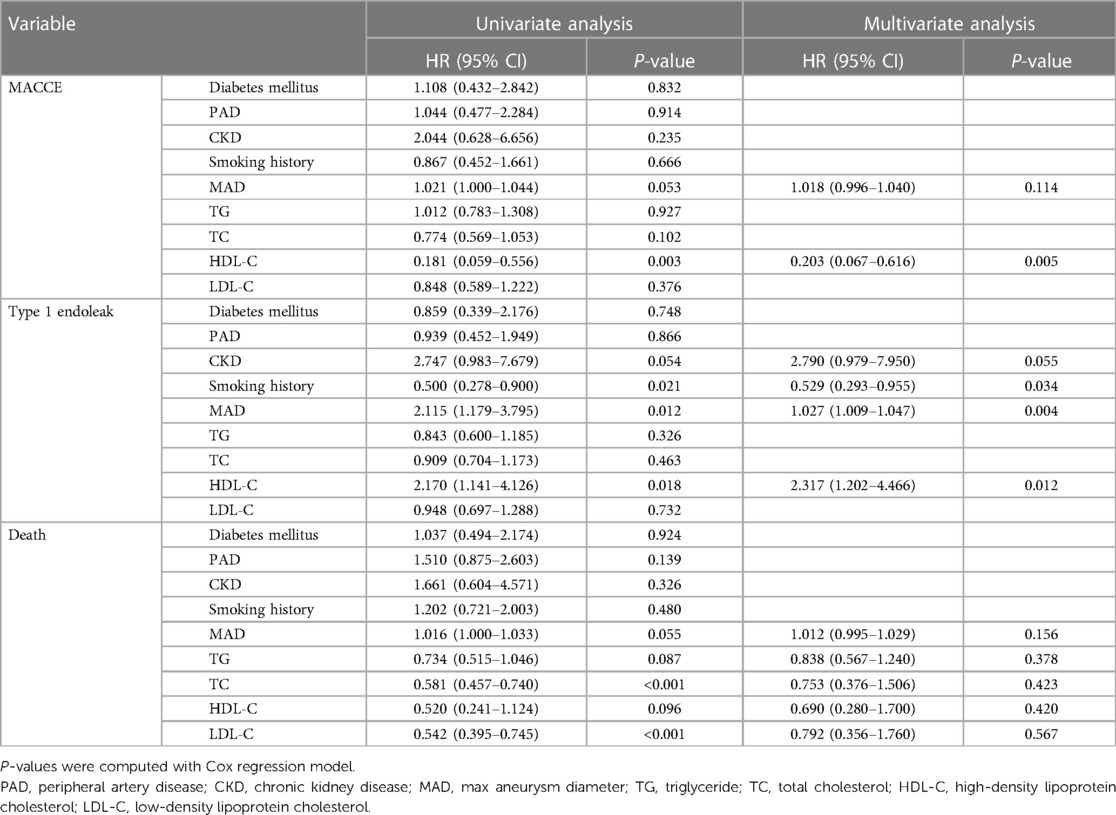
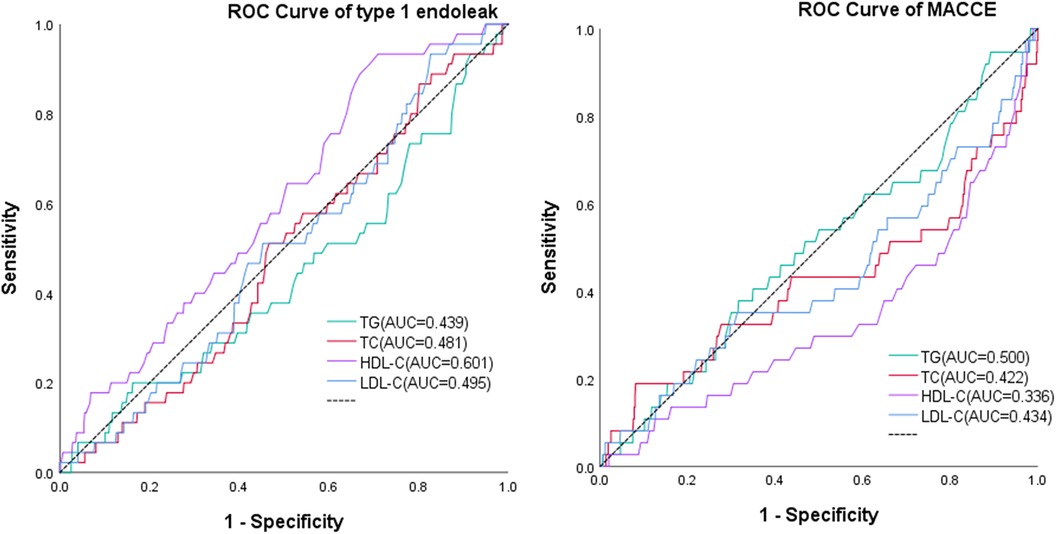
Analysis for follow-up outcomesAs shown in Table 3 and Figure 5, multivariate analysis showed that high level of HDL-C was the protective factor (HR, 0.203, 95% CI, 0.067–0.616, P = 0.005) for MACCES, but it was the risk factor for type I endoleak (HR, 2.317, 95% CI, 1.202–4.466, P = 0.012), ROC analysis showed that the level of HDL-C can be used to predict Type I endoleak (AUC = 0.601). Smoking history was the protective factor (HR, 0.529, 95% CI, 0.293–0.955, P = 0.034) for type I endoleak, the larger MAD was the risk factor (HR, 1.027, 95% CI, 1.009–1.047, P = 0.004) for type I endoleak.
Table 3. Univariate and multivariate analyses for predictors of follow-up outcomes.
Figure 5. ROC analysis of TG, TC, HDL-C, and LDL-C compared to MACCEs and type 1 endoleak.
DiscussionDyslipidemia includes a series of lipid abnormalities that may involve elevated TG, TC, and LDL-C levels or a decrease in HDL-C (13). There are regional differences in blood lipid levels, which are related to economic level and dietary structure (14). Our definition of dyslipidemia was based on the distribution of blood lipid levels in the population of our region, which may differ from the blood lipid limit values of other institutions for dyslipidemia. Due to the population distribution characteristics of patients with AAA, dyslipidemia is a common risk factor and comorbidity of AAA (15, 16). A previous study reported an 47.5% incidence of dyslipidemia in patients with AAA, close to 42.3% reported in our study (12). Patients with CKD have a characteristic lipid pattern of hypertriglyceridemia and reduced level of HDL-C (17), which were also often seen in patients with diabetes (18). Smoking is widely recognized as a risk factor for dyslipidemia (19), and dyslipidemia is a risk factor for peripheral artery disease (20). As shown in Table 1, the rates of CKD (3.0% vs. 6.3%, P = 0.043), diabetes (10.0% vs.15.1%, P = 0.050), smoking history (56.5% vs. 64.6%, P = 0.039), and PAD (17.3% vs. 25.8%, P = 0.018) in the dyslipidemia group were higher than those in the non-dyslipidemia group. Our study outcomes were consistent with the above viewpoints. Dyslipidemia is an important risk factor for CAD and stroke (13, 21), which is consistent with our study outcome that the dyslipidemia group had a higher rate of MACCEs (2.97% vs. 9.59%, P < 0.001), but there was no difference in the incidence of preoperative CAD (17.6% vs. 19.2%, P = 0.517), PCI (11.6% vs.12.5%, P = 0.722) and stroke (6.5% vs. 6.3%, P = 0.913) between the two groups.
Dyslipidemia is more common among people in high-income countries; however, due to dietary structure changes worldwide, its prevalence is increasing, even in low-income countries, particularly in rapidly developing China (14, 22, 23). In the future, the proportion of concomitant dyslipidemia in patients with AAA is predicted to increase. There is still a lack of research on the impact of dyslipidemia on the prognosis of patients with AAA after EVAR. This may be the first study conducted in southwestern China to explore the impact of dyslipidemia on the prognosis of patients with AAA after EVAR. Our study outcomes show that dyslipidemia will not increase the all-cause mortality incidence (10.27% vs. 9.59%, P = 0.778) and overall stent-related complications incidence (22.16% vs. 16.97%) in patients with AAA who underwent EVAR, but it will increase the risk of MACCEs (2.97% vs. 9.59%, P < 0.001) in patients with AAA who underwent EVAR, specially, it will increase the risk of type I endoleak in patients with AAA who underwent EVAR (9.19% vs. 4.06%, P = 0.012), ROC analysis also showed that the level of HDL-C can be used to predict Type I endoleak (AUC = 0.601). Currently, research on the effects of dyslipidemia on the formation of type I endoleak after EVAR is limited, why elevated HDL-C increased the risk of type I endoleak was unclear, there may be a lack of theoretical basis to explain it, this may also be a coincidence limited to statistics, and we need more researches to explore it. The relationship between elevated HDL-C levels and MACCEs risk is still controversial (24, 25), our study outcome suggested that high level of HDL-C was the protective factor (HR, 0.203, 95% CI, 0.067–0.616, P = 0.005) for MACCES, the larger MAD was the risk factor (HR, 1.027, 95% CI, 1.009–1.047, P = 0.004) for type I endoleak, which was consistent with the outcome of previous study (26). Why patient with smoking hirtory had a lower risk of type I endoleak (HR, 0.529, 95% CI, 0.293–0.955, P = 0.034) was unclear, this may be related to patients strictly quitting smoking and staying away from second-hand smoking environments after surgery.
A study pointed out that type II endoleak in patients with AAA after EVAR was associated with dyslipidemia (12); however, the main risk factors for type II endoleak include patent inferior mesenteric artery and patent lumbar artery (27, 28) Whether type II endoleaks can affect the formation of type II endoleaks after EVAR remains to be confirmed. The incidence of type II endoleaks in our study was 15.29%, which was lower than the 19.2% reported in a previous study (29), as shown in Table 2. There was no difference in the incidence of type II endoleaks between the two groups (16.22% vs. 14.02%, P = 0.446). In addition, dyslipidemia is closely related to atherosclerosis (30, 31), which also affects the lumbar and inferior mesenteric arteries. It may influence the patency of these arteries and may even reduce the incidence of type II endoleaks. The incidence of type III endoleaks, stent displacement, and iliac branch occlusion was low because of advancements in material technology and surgical techniques. The 2021 Canadian Cardiovascular Society Guidelines state that patients with AAA, dyslipidemia, and clinical atherosclerosis can benefit from statin therapy (32). Each patient with dyslipidemia was advised to take statins after EVAR, even after receiving treatment with statins, some patients' blood lipid levels were not well controlled, which may have been caused by irregular medication use, TG-rich lipoproteins and LDL particles were found to play key roles in the onset and development of cardiovascular disease (33, 34), we can see the incidence of MACCEs after EVAR was still significantly higher in the dyslipidemia group. Furthermore, many patients with dyslipidemia do not make dietary adjustments. For patients with dyslipidemia, more comprehensive management and treatment are needed, and it is imperative to monitor patients in order to prevent the transition to a state of dyslipidemia, with patient compliance playing a pivotal role.
Our study has a few limitations. First, this was a single-center retrospective study with small sample size. Second, due to the interval between postoperative follow-up examinations, records of endoleak occurrence time points may be inaccurate. Third, the completion of statin treatment in patients with dyslipidemia after EVAR has not been effectively monitored. Fourth, many patients do not return to the hospital for follow-up as planned, resulting in many patients being lost during midway visits; thus, postoperative management needs to be strengthened.
ConclusionDyslipidemia does not affect the mortality of patients with AAA who undergo EVAR but may increase the incidence of MACCEs. Dyslipidemia may decrease the incidence of type I endoleaks after EVAR; however, further studies are warranted. We should strengthen the postoperative management of patients with dyslipidemia, prevent the occurrence of MACCEs.
Data availability statementThe raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statementThe studies involving humans were approved by the ethics committee of West China Hospital, Sichuan University. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributionsXL: Writing – original draft, Methodology, Formal Analysis, Data curation, Conceptualization. QG: Writing – review & editing, Conceptualization, Methodology. JW: Writing – review & editing, Supervision, Data curation. YL: Software, Data curation, Writing – review & editing. JZ: Writing – review & editing, Supervision, Conceptualization. BH: Writing – review & editing, Methodology, Supervision, Conceptualization. XC: Methodology, Writing – review & editing, Data curation.
FundingThe authors declare that no financial support was received for the research, authorship, and/or publication of this article.
AcknowledgmentsThanks to all the medical staff in the Vascular Surgery Department and Information Department of West China Hospital for their help and guidance in collecting medical records.
Conflict of interestThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's noteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References6. Chaikof EL, Dalman RL, Eskandari MK, Jackson BM, Lee WA, Mansour MA, et al. The society for vascular surgery practice guidelines on the care of patients with an abdominal aortic aneurysm. J Vasc Surg. (2018) 67(1):2–77.e2. doi: 10.1016/j.jvs.2017.10.044
PubMed Abstract | Crossref Full Text | Google Scholar
7. Li C, de Guerre L, Dansey K, Lu J, Patel PB, Yao M, et al. The impact of completion and follow-up endoleaks on survival, reintervention, and rupture. J Vasc Surg. (2023) 77(6):1676–84. doi: 10.1016/j.jvs.2023.02.009
PubMed Abstract | Crossref Full Text | Google Scholar
8. Akmal MM, Pabittei DR, Prapassaro T, Suhartono R, Moll FL, van Herwaarden JA. A systematic review of the current status of interventions for type II endoleak after EVAR for abdominal aortic aneurysms. Int J Surg. (2021) 95:106138. doi: 10.1016/j.ijsu.2021.106138
PubMed Abstract | Crossref Full Text | Google Scholar
9. Weng LC, Roetker NS, Lutsey PL, Alonso A, Guan W, Pankow JS, et al. Evaluation of the relationship between plasma lipids and abdominal aortic aneurysm: a Mendelian randomization study. PLoS One. (2018) 13(4):e0195719. doi: 10.1371/journal.pone.0195719
PubMed Abstract | Crossref Full Text | Google Scholar
10. Nastasi DR, Norman R, Moxon JV, Quigley F, Velu R, Jenkins J, et al. The potential benefits and costs of an intensified approach to low density lipoprotein cholesterol lowering in people with abdominal aortic aneurysm. Eur J Vasc Endovasc Surg. (2021) 62(4):643–50. doi: 10.1016/j.ejvs.2021.06.031
PubMed Abstract | Crossref Full Text | Google Scholar
11. Martínez-López D, Cedó L, Metso J, Burillo E, García-León A, Canyelles M, et al. Impaired HDL (high-density lipoprotein)-mediated macrophage cholesterol efflux in patients with abdominal aortic aneurysm-brief report. Arterioscler Thromb Vasc Biol. (2018) 38(11):2750–4. doi: 10.1161/ATVBAHA.118.311704
Crossref Full Text | Google Scholar
12. Hall MR, Protack CD, Assi R, Williams WT, Wong DJ, Lu D, et al. Metabolic syndrome is associated with type II endoleak after endovascular abdominal aortic aneurysm repair. J Vasc Surg. (2014) 59(4):938–43. doi: 10.1016/j.jvs.2013.10.081
PubMed Abstract | Crossref Full Text | Google Scholar
16. Sakalihasan N, Michel JB, Katsargyris A, Kuivaniemi H, Defraigne JO, Nchimi A, et al. Abdominal aortic aneurysms. Nat Rev Dis Primers. (2018) 4(1):34. doi: 10.1038/s41572-018-0030-7
PubMed Abstract | Crossref Full Text | Google Scholar
17. Ferro CJ, Mark PB, Kanbay M, Sarafidis P, Heine GH, Rossignol P, et al. Lipid management in patients with chronic kidney disease. Nat Rev Nephrol. (2018) 14(12):727–49. doi: 10.1038/s41581-018-0072-9
PubMed Abstract | Crossref Full Text | Google Scholar
20. Berger JS, Hochman J, Lobach I, Adelman MA, Riles TS, Rockman CB. Modifiable risk factor burden and the prevalence of peripheral artery disease in different vascular territories. J Vasc Surg. (2013) 58(3):673–81.1. doi: 10.1016/j.jvs.2013.01.053
PubMed Abstract | Crossref Full Text | Google Scholar
22. Opoku S, Gan Y, Yobo EA, Tenkorang-Twum D, Yue W, Wang Z, et al. Awareness, treatment, control, and determinants of dyslipidemia among adults in China. Sci Rep. (2021) 11(1):10056. doi: 10.1038/s41598-021-89401-2
PubMed Abstract | Crossref Full Text | Google Scholar
23. Xing L, Jing L, Tian Y, Yan H, Zhang B, Sun Q, et al. Epidemiology of dyslipidemia and associated cardiovascular risk factors in northeast China: a cross-sectional study. Nutr Metab Cardiovasc Dis. (2020) 30(12):2262–70. doi: 10.1016/j.numecd.2020.07.032
PubMed Abstract | Crossref Full Text | Google Scholar
24. Bowe B, Xie Y, Xian H, Balasubramanian S, Zayed MA, Al-Aly Z. High density lipoprotein cholesterol and the risk of all-cause mortality among U.S. veterans. Clin J Am Soc Nephrol. (2016) 11(10):1784–93. doi: 10.2215/CJN.00730116
PubMed Abstract | Crossref Full Text | Google Scholar
25. Kaur M, Ahuja KR, Khubber S, Zhou L, Verma BR, Meenakshisundaram C, et al. Effect of high-density lipoprotein cholesterol levels on overall survival and major adverse cardiovascular and cerebrovascular events. Am J Cardiol. (2021) 146:8–14. doi: 10.1016/j.amjcard.2021.01.014
PubMed Abstract | Crossref Full Text | Google Scholar
26. Zuccon G, D'Oria M, Gonçalves FB, Fernandez-Prendes C, Mani K, Caldeira D, et al. Incidence, risk factors, and prognostic impact of type Ib endoleak following endovascular repair for abdominal aortic aneurysm: scoping review. Eur J Vasc Endovasc Surg. (2023) 66(3):352–61. doi: 10.1016/j.ejvs.2023.06.017
PubMed Abstract | Crossref Full Text | Google Scholar
27. Müller-Wille R, Güntner O, Zeman F, Dollinger M, Hälg C, Beyer LP, et al. The influence of preoperative aneurysmal thrombus quantity and distribution on the development of type II endoleaks with aneurysm sac enlargement after EVAR of AAA. Cardiovasc Intervent Radiol. (2016) 39(8):1099–109. doi: 10.1007/s00270-016-1386-2
Crossref Full Text | Google Scholar
28. Lo RC, Buck DB, Herrmann J, Hamdan AD, Wyers M, Patel VI, et al. Risk factors and consequences of persistent type II endoleaks. J Vasc Surg. (2016) 63(4):895–901. doi: 10.1016/j.jvs.2015.10.088
PubMed Abstract | Crossref Full Text | Google Scholar
29. Mulay S, Geraedts ACM, Koelemay MJW, Balm R. Type 2 endoleak with or without intervention and survival after endovascular aneurysm repair. Eur J Vasc Endovasc Surg. (2021) 61(5):779–86. doi: 10.1016/j.ejvs.2021.01.017
PubMed Abstract | Crossref Full Text | Google Scholar
30. Sandesara PB, Virani SS, Fazio S, Shapiro MD. The forgotten lipids: triglycerides, remnant cholesterol, and atherosclerotic cardiovascular disease risk. Endocr Rev. (2019) 40(2):537–57. doi: 10.1210/er.2018-00184
PubMed Abstract | Crossref Full Text | Google Scholar
31. Hurtubise J, McLellan K, Durr K, Onasanya O, Nwabuko D, Ndisang JF. The different facets of dyslipidemia and hypertension in atherosclerosis. Curr Atheroscler Rep. (2016) 18(12):82. doi: 10.1007/s11883-016-0632-z
PubMed Abstract | Crossref Full Text | Google Scholar
32. Pearson GJ, Thanassoulis G, Anderson TJ, Barry AR, Couture P, Dayan N, et al. 2021 Canadian cardiovascular society guidelines for the management of dyslipidemia for the prevention of cardiovascular disease in adults. Can J Cardiol. (2021) 37(8):1129–50. doi: 10.1016/j.cjca.2021.03.016
留言 (0)