
記住我
Chronic spontaneous urticaria (CSU) is a mast cell-mediated disease characterized by the recurrent appearance of wheals and/or angioedema for longer than 6 weeks.1 The main pathophysiology that drives mast cell activation is thought to involve autoimmune mechanisms; research indicates that viral infections are a triggering factor for new-onset urticaria. Many reports have noted the occurrence of acute urticaria (AU) with COVID-19 infection, with incidences ranging from 12.5% to 19.0% and a median symptom duration of 6.8 days.2–5 Although AU may be seen before or after the start of COVID-19 symptoms, it most commonly occurs simultaneously.2 In addition, exacerbation of chronic urticaria during COVID-19 infection has been reported in one-third of patients with CSU.6
Although COVID-19 infection is frequently reported to cause AU and exacerbate CSU, there have been no reports of CSU triggered by COVID-19 infection. The underlying mechanism and features associated with the chronicity of urticaria after COVID-19 infection need to be determined. In this study, the authors report COVID-19 infection-induced CSU (C-19-CSU) and compare its features with COVID-19 infection-induced AU (C-19-AU). They aimed to determine in which patients COVID-19 infection leads to CSU and possible indicators of chronicity by comparing the laboratory and clinical features of possible C-19-AU and C-19-CSU cases.
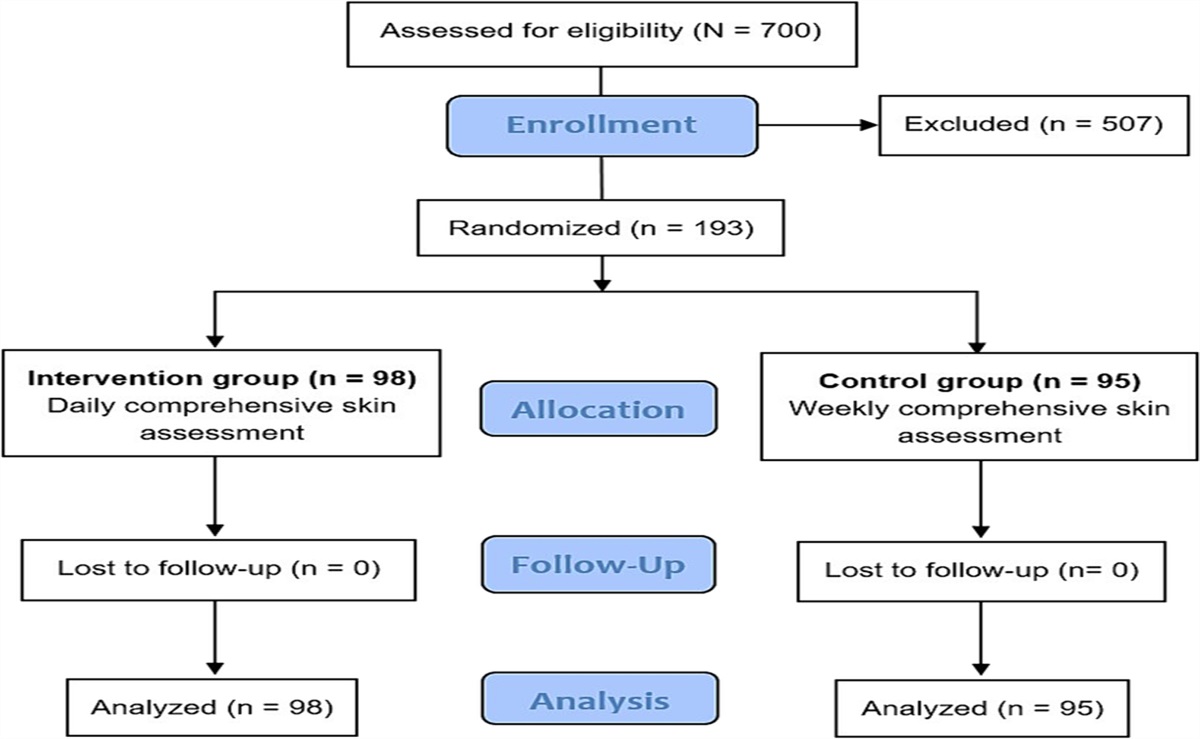
METHODSThis retrospective case-control study of the Urticaria Centers of Reference and Excellence in Turkey took place between March 2020 and September 2022.7 Patients were divided into either the study group or the control group based on the timing and duration of their urticaria. Those with CSU who reported their urticaria started within 4 weeks after COVID-19 infection and lasted for longer than 6 weeks composed the study group (C-19-CSU) and those whose urticaria started within 1 week before and 3 weeks after COVID-19 infection and lasted less than 6 weeks composed the control group (C-19-AU). To avoid confounding, patients with less than 3 months between COVID-19 vaccination and the onset of urticaria were excluded from the control group but because of limited patient numbers were included in the study group when indicated. Patients were excluded from the study if they had immunosuppression, chronic thyroid disease, chronic autoimmune disease, active viral infections, incomplete file records, or a history of immunization suggesting that it may trigger CSU; did not have complete blood counts; or did not provide informed consent. The research protocol was approved by the Sakarya University Ethics Committee and was conducted in accordance with the ethical regulations of the Declaration of Helsinki.
The researchers retrieved the following data from patient’ clinical files: demographic characteristics, interval between COVID-19 and onset of urticaria, duration of urticaria, COVID-19 disease severity, COVID-19 vaccination and treatment status, and laboratory test results during active urticaria complaints (eosinophil count, basophil count) and during remission (total serum immunoglobulin E [IgE] level, antinuclear antibody [ANA] positivity, and anti-thyroid peroxidase antibody [anti-TPO] positivity). They compared the C-19-CSU and C-19-AU groups in terms of clinical, demographic, and laboratory features; such as autoimmune parameters including anti-TPO, ANA positivity, low total IgE, eosinopenia, and basopenia.
The presence of angioedema was lacking in the AU group and was not included in the analysis. Further, some case files lacked information on autoimmune parameters; analysis was performed with patients who had those data in their files.
The researchers classified the participants’ COVID-19 infection severity with the assistance of the most current WHO definitions for COVID-19.8 Patients with acute respiratory distress syndrome, sepsis, septic shock, or other conditions that require the provision of life-sustaining therapies such as mechanical ventilation (invasive or noninvasive) or vasopressor treatment were classified as having critical COVID-19 infection. Patients with severe pneumonia and signs of severe respiratory distress (in adults: accessory muscle use, inability to complete full sentences, respiratory rate > 30 breaths/min, and an oxygen saturation < 90% on room air) were classified as having severe COVID-19 infection. Patients with no criteria for severe or critical COVID-19 infection were placed in the nonsevere COVID-19 group (WHO).
Statistical analyses were performed using IBM SPSS version 20.0 for Windows statistical software (IBM Corp). Continuous variables were expressed as mean and SD, and categorical variables were expressed as percentages. Kolmogorov-Smirnov analysis was performed for distribution normality analyses, and nonparametric tests were preferred according to the results of this analysis. The Kruskal-Wallis analysis was used for pairwise comparisons between groups, and the χ2 test was used to compare categorical variables. P < .05 was considered significant.
RESULTSThe authors identified 144 patients with COVID-19 infection-triggered AU. Of these, 85 met the inclusion criteria and were included in the control group (C-19-AU). Seven patients with possible C-19-CSU were included in the study group (C-19-CSU). The mean age of patients in the C-19-CSU group was 27.14 (SD, 7.84) years, and 71.4% were women, whereas patients in the C-19-AU group had a mean age of 36.44 (SD, 19.58) years, and 60.0% were women (Table 1). The differences were not statistically significant when the groups were compared in terms of age or sex distribution (Ps = .325 and .551, respectively).
Table 1. - COMPARISON OF FEATURES OF COVID-19-INDUCED CSU AND AU Characteristic COVID-19-Induced CSU (n = 7), Mean ± SD or n/n (%) COVID-19-Induced AU (n = 85), Mean ± SD or n/n (%) P Age, y 27.14 ± 7.84 36.44 ± 19.58 .325 Sex (male/female) 5/7 (71.4%) 51/85 (60%) .551 Interval between COVID-19 and urticaria, d 17.92 ± 6.17 4.48 ± 2.78 .000 Urticaria duration 7.55 ± 3.97 mo 7.10 ± 3.43 d — COVID-19 disease severity (ratio of severe cases) 1/7 (14.2%) 18/85 (21.2%) .892 Eosinopenia (<0.05 K/μL) 2/7 (28.4%) 5/85 (6%) .031 Basopenia (<0.01 K/μL) 2/7 (28.4%) 7/85 (8.3%) .085 Low total IgE level (<40) 2/7 (14.3%) 6/28a (21.4%) 1.000 Antinuclear antibody positivity 0/7 (30.8) 3/19a (15.8) — Antithyroid peroxidase positivity 1/7 (14.2) 8/19a (42.1) .186Abbreviations: AU, acute urticaria; CSU, chronic spontaneous urticaria; IgE, immunoglobulin E.
Some of the laboratory data were lacking in the COVID-19 AU group. The missing values were not analyzed.
aOnly patients with relevant data were included in the analysis.
In the C-19-CSU group, four patients (57.1%) had isolated CSU, and three had accompanying chronic inducible urticaria (two symptomatic dermographism, one cholinergic urticaria). Although urticaria was the leading symptom in all seven patients, two patients (28.6%) also presented with angioedema. The characteristics of the patients in the C-19-CSU group are shown in Table 2.
Table 2. - THE CHARACTERISTICS OF PATIENTS WITH CSU INDUCED BY COVID-19 INFECTION Variable Case 1 Case 2 Case 3 Case 4 Case 5 Case 6 Case 7 Age, y 17 26 30 32 19 26 40 Sex Female Female Male Female Female Female Male Angioedema + − − − + − − Accompanying CinDU4 Cholinergic SD None None SD None None Diagnosis of COVID-19 PCR PCR PCR PCR PCR PCR Clinical Interval between COVID-19 and CSU, d 15 20 20 28 20 23 19 CSU duration, mo 7 10 mo 21 11 8 12 22 Chronic disease None None HBV carrier None None AR and AA None COVID-19 disease severity Not severe Severe Not severe Not severe Not severe Not severe Not severe Eosinopenia (<0.05 K/μL) Yes Yes No No No No No Basopenia (<0.01 K/μL) Yes No No No Yes No No Total serum IgE level <17 201 56 155 128 56 35 Anti-TPO (+) Yes No No No Yes No No ANA (+) − − − − − − − Vaccination None BNT None Sinovac None BNT Sinovac Interval between vaccination and CSU, mo − 2 − 6 − − − Treatment for COVID-19 None None None None None None FavipiravirAbbreviations: AA, allergic asthma; ANA, antinuclear antibody; anti-TPO, anti-thyroid peroxidase; AR, allergic rhinitis; AU, acute urticaria; CinDU, chronic inducible urticaria; CSU, chronic spontaneous urticaria; HBV, hepatitis B; IgE, immunoglobulin E.
Six of the C-19-CSU patients were diagnosed with COVID-19 by polymerase chain reaction test, whereas one had a history of contact with infected people and clinical findings of COVID-19. In the C-19-AU group, all patients’ diagnoses were confirmed by polymerase chain reaction test.
The mean durations of urticaria for the C-19-CSU and C-19-AU groups were 7.55 (SD, 3.97) months (range, 7-22 months) and 7.10 (SD, 3.43) days (range, 2-21 days), respectively. The average time between COVID-19 infection and the start of urticaria differed significantly between groups (20.71 [SD, 3.98] days in C-19-CSU vs 4.48 [SD, 2.78] days in C-19-AU, respectively; P = .000). In the C-19-CSU group, none of the patients’ urticaria started before or simultaneously with COVID-19 symptoms. In contrast, 83.5% of the patients in the C-19-AU group had urticaria concurrent with COVID-19 infection symptoms, and 5.9% developed urticaria before COVID-19 symptoms (P < .001; Table 3). All of the patients in the C-19-AU group and 78.6% (n = 11) of the patients in the C-19-CSU group were treated with antihistamines; one patient in the C-19-CSU group (14.2%) required omalizumab treatment (300 mg per month).
Table 3. - THE TIMING OF URTICARIA IN RELATION TO COVID-19 SYMPTOMS Variable COVID-19-Induced CSU (n = 7), n (%) COVID-19-Induced AU (n = 85), n (%) P Eruption of lesions before COVID-19 symptoms — 5 (5.9) .000 Eruption of lesions simultaneous with COVID-19 symptoms — 71 (83.5) Eruption of lesions after COVID-19 symptoms 7 (100) 9 (10.6)Abbreviations: AU, acute urticaria; CSU, chronic spontaneous urticaria.
When the groups were classified according to the severity of COVID-19 infection, most patients in both groups (85.7% in CSU, 78.2% in AU) were in the nonsevere category. One patient in the C-19-AU group (2%) was in the critical category. One patient in the C-19-CSU group (14.2%) and 17 patients in the C-19-AU group (20.0%) were in the severe category (P = .892; Table 1).
To avoid possible cases of urticaria induced by vaccination, the researchers excluded 12 patients who were vaccinated within 3 months of AU onset. Two patients were vaccinated before CSU onset; one was vaccinated with Sinovac (CoranaVac) and one with BNT162b2 mRNA (Pfizer-BioNTech). The patient who was vaccinated with BNT162b2 mRNA had an approximately 2.5-month prodromal period between vaccination and CSU onset. During the follow-up period after CSU diagnosis, the patient readministered the BNT162b2 mRNA vaccine, and no exacerbation of urticaria was observed. The patient who was vaccinated with Sinovac had a COVID-19 infection 6 months after vaccination and developed CSU. Considering the circumstances of both patients, it is unlikely that vaccination caused urticaria.
Urticaria secondary to COVID-19 medication use was also not considered likely in either group. One patient in the study group received favipiravir treatment and developed urticarial symptoms 19 days afterward. Thus, favipiravir was not considered a trigger for CSU because of the long time interval.
Among the laboratory tests examined, eosinopenia was the only parameter that served as an indicator for chronicity of C-19-CSU. In the C-19-CSU group, two patients (14.2%) had eosinopenia, and two (14.2%) had basopenia. In the C-19-AU group, five patients (6%) had eosinopenia, and seven (8.3%) had basopenia. The laboratory findings in the remission period of CSU showed that two patients (14.2%) had low total IgE levels, and two (14.2%) had anti-TPO positivity. None of the patients had ANA positivity in the C-19-CSU group. In the C-19-AU group, six patients (21.4%) had high total IgE levels, eight (42.1%) had anti-TPO positivity, and three (15.8%) had ANA positivity. Eosinopenia was the only parameter to differ significantly between groups (P < .05; Table 1).
DISCUSSIONSimilar to previous reports, the population of patients with urticaria in the present study was primarily composed of middle-aged women.2 Tan et al2 reported that urticarial lesions triggered by C-19-AU occurred before the symptoms of COVID-19 in 4.6% of patients, simultaneously in 51.7%, and after in 33.1%. Similarly, Algaadi9 stated that most patients in their series reported simultaneous infection and urticaria. Consistent with the literature data, most of the patients in the C-19-AU group in the present study had urticarial symptoms simultaneously with COVID-19 infection (83.5%), whereas none of the patients in the C-19-CSU group presented concurrently with COVID-19 infection. The duration of urticaria in the AU group was 1 week, which is consistent with the previously reported duration of C-19-AU cases.1,2 Likewise, the interval between the onset of infection and urticaria complaints in C-19-AU patients was similar to the data in the literature. However, one of the most striking findings of the present research was the more extended time between infection and urticaria in the C-19-CSU group compared with the C-19-AU group.
The longer time interval between infection and urticaria onset in patients with CSU versus those with AU suggests that mechanisms involved in CSU and AU might differ. The natural course of progression from AU to CSU in the adult population is yet to be fully understood. Different immune response components to infection may be responsible for the difference, such as the various receptors that are involved in mast cell activation, including Toll-like, retinoic acid-inducible gene I-like, high-affinity IgE, complement, and interleukin 1 receptors.10,11 Activation of these receptors results in mast cell activation and degranulation and de novo synthesis of eicosanoids, cytokines, chemokines, and growth factors. In addition, immune complexes accumulated in the circulation lead to complement activation, which might explain how urticaria becomes chronic in some cases.10 This mechanism was supported by the demonstration of colocalization of SARS-CoV-2 glycoproteins with complement components in cutaneous blood.2
Likewise, in a case series with COVID-19 vaccination-induced CSU, Magen et al12 found that patients with AU progressing to CSU are characterized by a positive autologous serum skin test result, thyroid autoimmunity, and deep basopenia at baseline. The mast cell might be activated by IgE and IgG autoantibodies against the thyroid and nuclear antigens, which, at a more fundamental level, can promote the secretion of type I interferons by plasmacytoid dendritic cells, stimulate the recruitment of basophils to lymph nodes, and directly activate adaptive immune responses via B and T cells.13 In the present study, eosinopenia, which is suggested to be a marker of autoimmunity (PURIST), was present in a significantly higher number of patients in the C-19-CSU group. There was no significant between-group difference in basopenia. However, many patients with AU lacked other autoimmune parameters such as anti-TPO and ANA in their files, and it is possible that the analysis would be more precise if there were no missing data. Future prospective studies should include these parameters.
Vaccines developed for the prevention of COVID-19 infection may be another trigger for CSU. Many CSU cases that were possibly triggered by COVID-19 vaccinations have been reported.14 Most of the cases were associated with BNT162b2 mRNA or AstraZeneca vaccines, and the median time of urticaria onset has been reported to range between 1 day and 3 months.14 In particular, patients have developed CSU following vaccination with the BNT162b2 mRNA and ChAdOx1-S vaccines.15–17 It is thought that the immunologic response to the vaccine stimulates the CSU, possibly by releasing suppressed histamine-releasing autoantibodies or by stimulating the production of anti-high-affinity IgE receptor α autoantibodies.15 In the present study, the researchers excluded patients with a history of vaccination within 3 months from participating in the C-19-AU group to avoid including cases of vaccine-related AU. However, because of the limited number of patients in the CSU group, patients meeting this criterion were not automatically excluded but examined in more detail. Two patients were vaccinated before CSU with no established correlation between symptoms and vaccination.
When considering an association between infections and urticaria, the possibility of drug-induced urticaria must be ruled out. Although there are cases of AU associated with favipiravir, there are no reports of CSU.18 Punyaratabandhu and Vanitchpongphan18 reported that AU developed in two patients with COVID-19 who were treated with favipiravir. The time between favipiravir treatment and the formation of urticarial rash in these two patients was 1 day and 7 days, and urticarial eruptions regressed 1 day after cessation of favipiravir treatment. One of the patients in the present study received favipiravir treatment. For that patient, urticarial symptoms occurred 19 days after favipiravir treatment, which makes favipiravir unlikely as a trigger for CSU.
LimitationsThis study has limitations because of its retrospective nature, such as a need for more information on angioedema and missing laboratory data. In addition, the number of patients in the CSU group is limited. The role of COVID-19 infection as a trigger of urticaria cannot be proven or disproven and so remains possible. Moreover, the possibility of inactive hepatitis virus B infection, drugs, stress, or other unknown factors as triggering causes of CSU cannot be ruled out.
CONCLUSIONSCOVID-19 infection-induced CSU and C-19-AU have distinct characteristics and seem to arise by different mechanisms. The onset of urticaria 2 or more weeks after COVID-19 infection may serve as the main indicator for urticaria that will last longer than 6 weeks and may help physicians foresee the possible course of urticaria associated with COVID-19 infection.
REFERENCES 1. Zuberbier T, Abdul Latiff AH, Abuzakouk M, et al. The international EAACI/GA2LEN/EuroGuiDerm/APAAACI guideline for the definition, classification, diagnosis, and management of urticaria. Allergy 2022;77(3):734–66. 2. Tan SW, Tam YC, Oh CC. Skin manifestations of COVID-19: a worldwide review. JAAD Int 2021;2:119–33. 3. Recalcati S. Cutaneous manifestations in COVID-19: a first perspective. J Eur Acad Dermatol Venereol 2020;34(5):e212–3. 4. Freeman EE, McMahon DE, Lipoff JB, et al. The spectrum of COVID-19-associated dermatologic manifestations: an international registry of 716 patients from 31 countries. J Am Acad Dermatol 2020; 83:1118–29. 5. Galván Casas C, Català A, Carretero Hernández G, et al. Classification of the cutaneous manifestations of COVID-19: a rapid prospective nationwide consensus study in Spain with 375 cases. Br J Dermatol 2020;183(1):71–7. 6. Kocatürk E, Salman A, Cherrez-Ojeda I, et al. The global impact of the COVID-19 pandemic on the management and course of chronic urticaria. Allergy 2021;76(3):816–30. 7. Maurer M, Metz M, Bindslev-Jensen C, et al. Definition, aims, and implementation of GA(2) LEN Urticaria Centers of Reference and Excellence. Allergy 2016;71(8):1210–8. 8. World Health Organization. Living guidance for clinical management of COVID-19. https://www.who.int/publications/i/item/WHO-2019-nCoV-clinical-2021-2. Accessed November 23, 2021. 9. Algaadi SA. Urticaria and COVID-19: a review. Dermatol Ther 2020;33(6):e14290. 10. Imbalzano E, Casciaro M, Quartuccio S, et al. Association between urticaria and virus infections: a systematic review. Allergy Asthma Proc 2016;37(1):18–22. 11. Arias-Santiago SA, Almazán-Fernandez FM, Burkhardt-Perez P, Naranjo-Sintes R. Cold urticaria associated with Epstein Barr virus mononucleosis. Actas Dermosifiliogr 2009;100(5):435–6. 12. Magen E, Zueva E, Mishal J, Schlesinger M. The clinical and laboratory characteristics of acute spontaneous urticaria and its progression to chronic spontaneous urticaria. Allergy Asthma Proc 2016;37(5):394–9. 13. Bansal CJ, Bansal AS. Stress, pseudoallergens, autoimmunity, infection and inflammation in chronic spontaneous urticaria. Allergy, Asthma Clin Immunol 2019;11;15:56 14. De Montjoye L, Herman A, Baeck M. Chronic spontaneous urticaria following COVID-19 vaccination. JAAD Case Rep 2022;25:35–8. 15. Magen E, Yakov A, Green I, Israel A, Vinker S, Merzon E. Chronic spontaneous urticaria after BNT162b2 mRNA (Pfizer-BioNTech) vaccination against SARS-CoV-2. Allergy Asthma Proc 2022;43(1):30–6. 16. Pescosolido E, Muller YD, Sabaté-Brescó M, et al. Clinical and immunological data from chronic urticaria onset after mRNA SARS-CoV-2 vaccines. Clin Exp Allergy 2022;52(11):1343–6. 17. Suan D, Lee AYS. Chronic spontaneous urticaria following ChAdOx1-S COVID-19 vaccination. Allergo J Int 2022;31(4):121–2. 18. Punyaratabandhu P, Vanitchpongphan S. Favipiravir-induced cutaneous adverse reactions in patients infected with COVID-19. Clin Exp Dermatol 2022;47(3):573–7.
留言 (0)