
記住我



Acute retinal necrosis (ARN) is a rare but severe ophthalmic pathology defined by panuveitis, retinal necrosis, and high rates of retinal detachment [1]. ARN may lead to poor visual outcomes even if promptly diagnosed and treated [2, 3]. The primary goal of treating ARN with intravenous antiviral drugs such as aciclovir, valaciclovir, and ganciclovir is to halt the progression of the disease in the affected eye and prevent it from developing to the other eye [4, 5]. The use of polymerase chain reaction analysis of aqueous or vitreous fluid can aid in the prompt diagnosis of ARN [2]. Additional treatment options may include intravitreal antiviral agents, as well as topical and oral corticosteroids, antithrombotic treatment, prophylactic laser barricade, and vitrectomy, but the effectiveness of these treatments can vary [2]. A combination of therapies may help to reduce the risk of severe vision loss and improve visual acuity, but more research is needed in this area. The focus of this review is to highlight the latest developments in the diagnosis and treatment of ARN. Specifically, it explores the use of a combination of antiviral therapy and surgical interventions to manage the disease.
Historical aspectsIn 1971, a Japanese ophthalmologist named Akira Urayama [6] first identified ARN as a unilateral disease, characterized by panuveitis and retinal arteritis that ultimately led to retinal detachment and necrotizing retinitis. A few years later, the term “BARN” was coined by Young and Bird [7] to describe the occurrence of bilateral ARN (BARN). The definitive identification of a viral cause affecting all layers of the retina was shown by Culbertson et al. [8] using electron microscopy. The examination of tissue samples revealed severe acute necrosis of the retina, retinal arteritis, and the presence of eosinophilic intranuclear inclusions in retinal cells. It is now widely accepted that the primary cause of ARN is the varicella-zoster virus (VZV), with herpes simplex virus 1 and 2 (HSV-1 and 2) being the second most common cause, and cytomegalovirus (CMV) being a less common cause [9]. Although the Epstein-Barr virus (EBV) has been occasionally linked to ARN [10], it is generally not considered pathogenic in most cases [11].
EpidemiologyARN is still considered a rare yet dreadful clinical entity. In the United Kingdom, two studies were conducted by the British Ophthalmological Surveillance Unit (BOSU) utilizing a monthly surveillance system [12, 13] and reported an incidence rate ranging from 0.5 to 0.63 cases per million population per year [13]. In Japan, ARN accounts for around 1.3-1.4% of all uveitis cases [14, 15]. There is no known gender or race predilection for ARN; however, a genetic link has been found in Caucasians with the HLA-DQw7 antigen and HLA-Bw62 phenotype, suggesting a potential immune predisposition to developing ARN [16]. Older individuals are more likely to develop ARN due to the varicella-zoster virus (HZV) and herpes simplex virus 1 (HSV-1), whereas those under 25 years old are more frequently affected by HSV-2 [9, 17]. It has been reported that HSV-2 can cause ARN even up to 30 years after a neonatal infection [18]. ARN typically affects immunocompetent and healthy adults, in contrast to Progressive Outer Retinal Necrosis (PORN), another type of herpetic retinopathy that occurs in immunocompromised individuals [2]. Interestingly, one report showed a seasonal variation in ARN incidence, with the highest rates occurring during winter and spring [19]. ARN can occur several years after the primary infection or follow a systemic herpetic infection (e.g., herpetic dermatitis or encephalitis) [20]. Interestingly, studies have documented a history of a prior herpetic infection in up to 55% of ARN patients [12, 21]. It is important to consider ARN in patients with herpes encephalitis, as the incidence of ARN in these patients has been reported to be 4% to 8% [22].
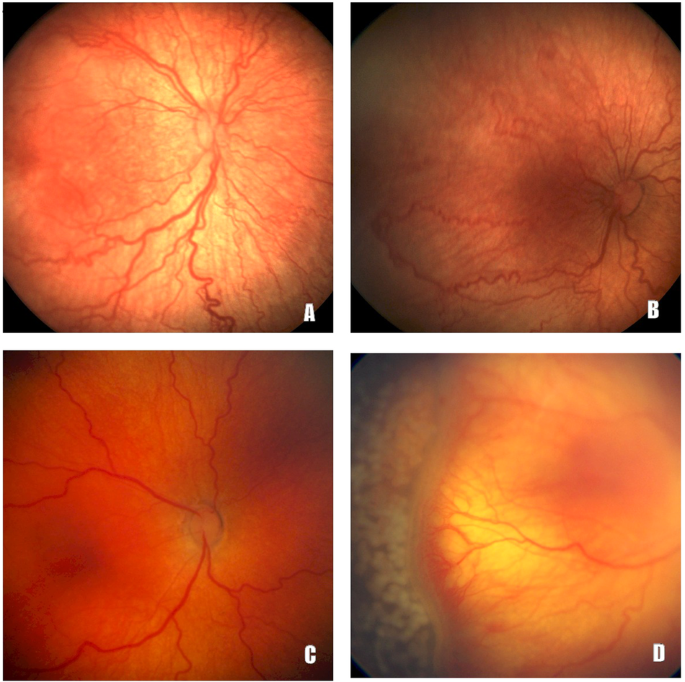
Clinical features and complicationsARN may present with a wide spectrum of clinical findings compatible with panuveitis including anterior uveitis, scleritis, vitritis, necrotizing retinitis, occlusive vasculitis, and optic disc oedema [2, 3]. Initially, ARN may manifest with mild and nonspecific symptoms such as redness, photophobia, floaters, blurry vision, and pain. Most cases are confined to a single eye, but some cases may involve both eyes (BARN). The clinical features of ARN can be divided into two phases. In the first phase, anterior chamber reaction and typically granulomatous keratic precipitates can be observed. A dilated fundoscopy may reveal varying degrees of vitritis with distinct, multifocal, confluent patches of yellowish-white infiltrates in the deep retina and the retinal pigment epithelium (RPE) [Fig. 1a, b]. These infiltrates typically begin in the peripheral regions of the eye, and there may be signs of vasculitis (usually arteritis) with limited retinal haemorrhages. Atypical features of ARN, such as Kyrieleis arteriolitis [23], segmental granular lesions aligned along the retinal vessels [24], and choroidal involvement [25] have also been reported. As the disease progresses, necrosis occurs, vitreous inflammation increases and the peripheral lesions rapidly spread toward the posterior pole. In the late cicatricial phase, retinal atrophy [Fig. 1c, d] and vitreous traction develop due to inflammatory changes, often leading to the development of a retinal detachment (RD) [11,12,13, 26]. Despite antiviral treatment, the incidence of RD in ARN cases can vary from 20% to 60% [1]. According to a recent systematic review and meta-analysis, approximately 2% of eyes with ARN have a RD at presentation, while 47% of cases eventually develop a RD over the course of the disease [27].
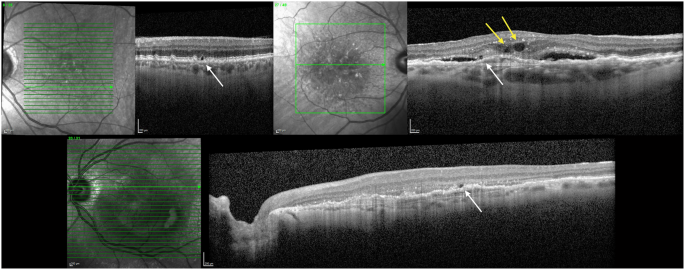
Fig. 1: A 63-year-old gentleman with a free ophthalmic and systemic history presented to the eye casualty with gradual worsening of his right eye vision over the last 48 h.
At presentation, the visual acuity of the affected eye did not exceed counting fingers at a 1-metre distance. a Dilated fundoscopy revealed dense vitritis (vitreous haze: 3 + ) (green asterisk) with distinct, multifocal, peripheral, confluent patches of yellowish infiltrates in the deep retina (blue arrows). Retinal haemorrhages can also be observed (yellow arrow). Aqueous humour was obtained with anterior chamber paracentesis and was sent for polymerase chain reaction (PCR) and flow cytometry. Due to the high suspicion of acute retinal necrosis patient was empirically started on antiviral treatment. PCR was positive for varicella-zoster virus. b Signs of occlusive vasculitis (blue arrows) with limited retinal haemorrhages (yellow arrows). c Patient was initially treated with intravenous aciclovir 750 mg three times daily. On the 6th day of this course 16 mg of oral prednisolone was added to the therapeutic regimen. Due to the occlusive vasculitis oral aspirin 100 mg once daily was also administered to the patient. He received an overall of 11 intravitreal ganciclovir injections Fundoscopic image after two months. Best corrected Snellen visual acuity remained stable at 5/10. d Examination of the peripheral retina with evidence of peripheral retinal atrophy.
It is expected that a greater extent of retinal changes in ARN patients can result in a higher risk of RD and a worse visual prognosis [1, 27, 28]. However, there is currently no uniform system to classify the extent of retinal changes in ARN. Some proposed classification systems include the cytomegalovirus retinitis classification system [29] and others based on the number of quadrants [27, 30] or the percentage of retina involved [31]. These classifications can be difficult to implement due to the vitreous inflammation and haze characteristic of ARN. Other factors that may worsen visual prognosis in ARN include VZV as the causative virus [27], more posterior location of retinitis [32], longer duration of symptoms before diagnosis [20], worse presenting visual acuity [12, 30, 32], and optic nerve involvement. ARN may also lead to other complications such as ocular hypotony, macular oedema, proliferative vitreoretinopathy (PVR), epiretinal membrane (ERM), optic atrophy, and phthisis.
Diagnostic approachDiagnostic criteriaThe American Uveitis Society introduced clinical criteria in 1994 for the diagnosis of ARN [33], while more recent criteria have been proposed by the Standardization of Uveitis Nomenclature (SUN) Working Group [34] and the Japanese ARN Study Group [35]. The aforementioned criteria are summarized in Table 1. Furthermore, our suggested diagnostic and therapeutic algorithm for the management of patients with ARN is outlined in Fig. 2.
Table 1 Available diagnostic criteria for ARN.Fig. 2: Suggested diagnostic and therapeutic algorithm for the management of patients with suspected acute retinal necrosis.
ARN is a rare but severe ophthalmic pathology defined by panuveitis, retinal necrosis, and high rates of retinal detachment. ARN may lead to poor visual outcomes even if promptly diagnosed and treated. The primary goal of treating ARN is to halt the progression of the disease in the affected eye and prevent it from developing to the other eye. Clinicians must always inquire about a possible history of a prior herpetic infection, and request medical assessment from other specialties (e.g., neurology) and neuro-imaging (e.g., in cases with herpes encephalitis) when necessary. The precise identification of the viral cause in suspected ARN cases has been greatly enhanced by the advancements in PCR techniques used for intraocular fluids. AC tap can be obtained and used for PCR testing and flow cytometric analysis to establish a diagnosis of ARN. Systemic treatment can be commenced empirically while waiting for the laboratory results. Further treatments (e.g., intravitreal antiviral agents or oral steroids) can be also added to the therapeutic regimen. Multimodal imaging is a valuable tool in evaluating patients with ARN, particularly in unusual cases. Close follow-up is mandatory to control the inflammatory process and evaluate the risk of potential complications (e.g., CMO, RD). AC anterior chamber, ARN acute retinal necrosis, CMO cystoid macular oedema, HZO herpes zoster ophthalmicus, Hx history, IOP intraocular pressure, PCR polymerase chain reaction, PPV pars plana vitrectomy, RD retinal detachment, VA visual acuity.
The role of multimodal imagingMultimodal imaging is a valuable tool in evaluating patients with ARN, particularly in unusual cases [36]. Fundus photography is essential in all cases, playing a crucial role in both diagnosis and ongoing monitoring [3, 20]. The significance of ultra-widefield imaging has been underscored due to its ability to offer a broader view of the posterior segment, thereby exposing additional peripheral lesions. This imaging technique could prove especially beneficial in several pathologies, including ARN. Since a considerable portion of their manifestations is expected to be situated in the mid-periphery and distal periphery, ultra-widefield imaging becomes particularly valuable in these cases [3, 20]. Fluorescein angiography can be useful in providing additional details that may not be visible during the fundoscopic examination, but its usefulness can be limited due to vitritis. Although it is not a diagnostic tool, it can reveal signs of occlusive arteritis and areas of capillary nonperfusion. The choroidal vasculature is typically affected, and areas of early hypofluorescence and late staining consistent with ischaemia-induced inflammatory changes may be visible. Diffuse leakage from retinal vessels due to active vasculitis may be seen as intense extravasation of dye. Early optic nerve involvement is common, and hyperfluorescence of the optic nerve can be observed on angiography [37]. The use of B-scan ultrasonography can be beneficial in detecting the onset of retinal detachment, particularly when limited visibility is present due to vitritis. Ultrasonography has the capability of penetrating through the haze of vitritis and identifying the elevation of the optic nerve head, along with the expansion of the optic nerve sheath [37]. Ultra-wide-field fundus imaging is especially useful in detecting and recording retinal lesions in ARN, especially those located at the periphery or concealed behind opaque media. This imaging method can provide critical information about the patient’s visual prognosis [38]. Ward and Reddy [39] observed that fundus autofluorescence (FAF) imaging can be used to identify and describe pathological changes in the neurosensory retina and RPE that occur in ARN. High contrast autofluorescence patterns can indicate disease activity borders in ARN, which can aid in monitoring disease progression. Optical coherence tomography (OCT) can also provide essential information in cases with early macular involvement. According to Jain et al. [40], hyperreflectivity and thickening of the inner plexiform layer were the initial changes seen on spectral domain OCT (SDOCT), followed by the involvement of all retinal layers corresponding to the yellowish-white lesion. The hyperreflectivity seen on SDOCT correlates with histopathologic evidence of oedema in the inner retinal layers, caused by occlusive vasculopathy of the arteries. En-face widefield OCT angiography (OCTA) can be utilized to non-invasively monitor changes in retinal vessel architecture in ARN over time [41]. However, OCTA artifacts caused by intraocular inflammation make interpretation difficult and will likely continue to be problematic in the future. Therefore, replacing fluorescein angiography completely may be challenging for some time due to issues with image clarity.
Diagnostic modalities Polymerase Chain Reaction (PCR)The precise identification of the viral cause in suspected ARN cases has been greatly enhanced by the advancements in PCR techniques used for intraocular fluids. This has resulted in a considerably high rate of virus detection, ranging from 79–100%, as reported in [42]. Due to the high sensitivity of PCR testing, if the results are negative, the ophthalmologist should either obtain another sample or explore other possible causes of inflammation. It has been observed [43] that there are no significant differences in the detection rates of aqueous and vitreous fluid samples. Aqueous humour is generally preferred as anterior chamber paracentesis is safer and less invasive compared to vitreous biopsy [44]. Studies have reported varying levels of sensitivity for herpesvirus PCR in aqueous humour samples, ranging from 84% to 100% [9]. Similar tests performed on vitreous samples have yielded values between 77.9% and 100% [26]. In addition to detecting the virus, quantitative PCR can also be useful in monitoring the levels of intraocular DNA in patients undergoing treatment or experiencing refractory cases to systemic and intravitreal treatment. By tracking the viral load, useful information can be obtained about treatment resistance and prognosis [1].
Goldmann–Witmer Coefficient (GWC)Initially, serum antibody titres were investigated to assist in diagnosing ARN. However, their interpretation proved challenging due to the high prevalence of antibodies to the viruses that cause ARN in most adults [45]. Additionally, serum antibody levels may not be elevated despite the significant reactivation of the virus in the eye in cases of ARN [46]. While serum antibodies alone are not useful for diagnosing ARN, a comparison of intraocular to serum antibodies can be used to calculate the Goldmann–Witmer coefficient (GWC), which has a high diagnostic value [45, 47]. The GWC has been proposed as a complementary diagnostic tool to PCR analysis of intraocular fluids for infectious uveitis. A GWC of 6 or higher is considered positive for intraocular infection, while a titre between 1 and 5 is considered suspect and a titre below 1 is negative [46]. However, this method has its limitations, including inadequate intraocular antibody production in the early onset of the disease and the variation in the positivity of the GWC over time from the onset of ARN [48]. Therefore, obtaining PCR of aqueous humour is typically recommended as the first-line test in suspected cases of ARN, with GWC calculation considered only if diagnostic challenges persist [47].
Flow cytometry (FC)In addition to PCR testing of intraocular fluids, flow cytometric (FC) analysis can be utilized to investigate lymphocyte subsets in the aqueous or vitreous humour [Fig. 3] and peripheral blood [49]. Kang et al. [50] reported that patients with VZV-induced ARN exhibit unique T lymphocyte subsets and cytokine profiles in intraocular fluids compared to those with non-infectious ARN. A high proportion of CD8 + T lymphocytes and low CD4/CD8 T cell ratios could potentially be used as a biomarker for diagnosing viral-infectious uveitis. Studying T lymphocytes at the site of inflammation could serve as a valuable research tool for distinguishing between viral and non-viral uveitis.
Fig. 3: Flow cytometry analysis of aqueous humour.
CD45 marker and side scatter are used to characterize ly
留言 (0)