
記住我









The data utilized in this analysis were derived from the Wave 3 (2015) of the China Health and Retirement Longitudinal Study (CHARLS). This longitudinal study, conducted by the National School for Development at Peking University, is an ongoing investigation concentrating on the demographic and health dynamics of middle-aged and older populations in China. CHARLS provides longitudinal data on a variety of factors, such as socioeconomic status and health, in a nationally representative sample of middle-aged and older Chinese. The conceptual approach and metrics have been adapted to be consistent with the HRS and other sister surveys. CHARLS utilized the multistage stratified probability sampling method to obtain a representative sample of the population from 150 municipalities within 28 provinces, municipal communities, and autonomous regions. The CHARLS collected data on demographics, household characteristics, biomedical measurements, health status, and functioning for the first time in 2011–2012, and then every two years thereafter. The survey design has been described in detail elsewhere [12].
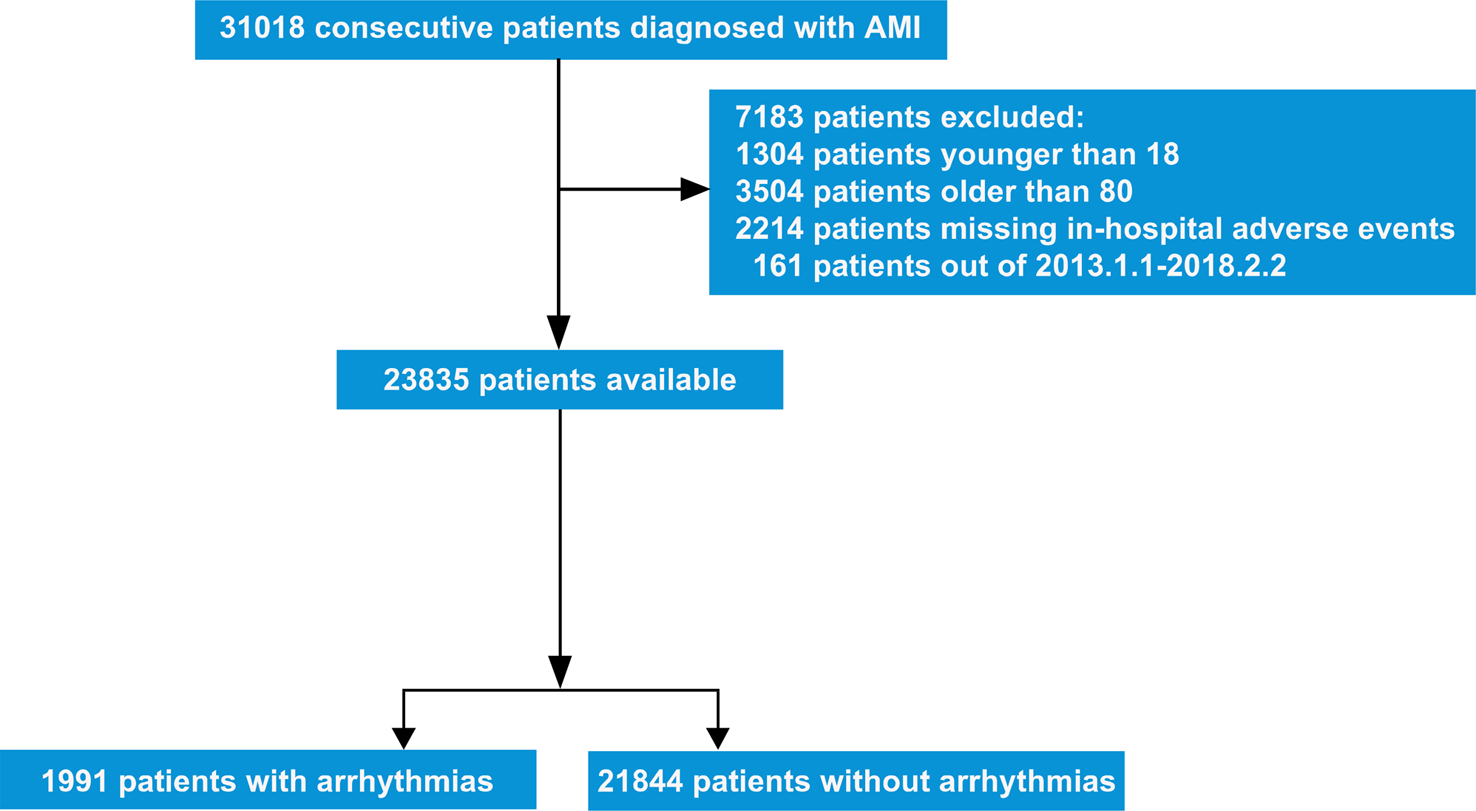
In wave 3, a total of 20,284 participants were questioned and asked to consent to venous blood samples. Participants under 45 years old (n = 571) and those without venous blood samples were excluded (n = 7,194). Eventually, a total of 12,519 adults were enrolled in our study. Further details on the inclusion and exclusion of study participants were shown in the Fig. 1.
Fig. 1
Flowchart of the participants selection
Definition of ambient PM2.5 and high-density lipoprotein cholesterol levelThe high-quality and high-resolution data on PM2.5 exposure concentrations for each residential city were obtained from the CHAP dataset [13]. The CHAP dataset utilized a combination of multi-source satellite remote sensing and artificial intelligence technology, carefully considering the spatial and temporal heterogeneity of air pollution. This comprehensive approach integrated diverse datasets, including ground observations, satellite remote sensing products, atmospheric reanalysis, and model simulations, to generate high-quality PM2.5 data records at a 1-km resolution spanning the period from 2000 to 2018 in China. This dataset has been successfully employed in numerous studies investigating the impact of air pollution on public health, including examinations of associations with conditions such as diabetes and cardiovascular diseases [14, 15]. Given privacy considerations pertaining to individual residential addresses, access was limited to city-level PM2.5 data, serving as a proxy for individual-level data. Participants were consequently matched to the city-level average PM2.5 concentration. The PM2.5 exposure level for each individual was computed as the average from the inception of the study in 2011 to its conclusion in 2015.
The study targeted the entire cohort of 21,100 individuals who participated in the third wave of the China Health and Retirement Longitudinal Study (CHARLS). A response rate of 64% yielded a total of 13,420 collected blood samples. The analysis of blood samples occurred in two distinct phases. Initially, local county health centers promptly conducted a comprehensive blood count (CBC) analysis, encompassing hemoglobin, hematocrit, white blood cell count, platelet count, and mean corpuscular volume, immediately following blood collection. Subsequently, the samples were transported to the central study headquarters, where the measurement of high-density lipoprotein (HDL) cholesterol was carried out [16].
CovariatesTo address potential confounding variables, this study incorporated specific parameters known to exert influence on the HDL level. Age was quantified in units of years, education was categorized into three levels: less than lower secondary, upper secondary & vocational training, and tertiary. Marital status was dichotomized into two categories: married or partnered, and separated, divorced, widowed, or never married. Residential locations were differentiated as rural or urban. BMI was calculated by dividing the weight in kilograms by the square of the height in meters. Participants were stratified based on their history of smoking and drinking. Additionally, numerous chronic diseases were identified as potential confounding factors through a structured inquiry, asking participants, “Have you received a doctor’s diagnosis for any of the listed conditions?” These conditions encompassed hypertension, lung diseases, stroke, psychiatric disorders, arthritis, liver disease, kidney disease, stomach/digestive diseases, and asthma. Relying on predictive mean matching approaches, missing covariate variables were addressed using multivariate imputation techniques.
Statistical analysisStandard deviations and means are utilized as measures of central tendency and dispersion for continuous variables that adhere to a normal distribution in the baseline characteristics, while the interquartile range and median are employed to represent continuous variables that conform to a skewed distribution. Rates and percentages are used to depict categorical variables. The Kruskal-Wallis test was utilized to determine p-values for continuous variables conforming to a skewed distribution. Conversely, chi-square tests were employed to analyze categorical data. The Fisher exact test was applied in cases where the expected cell count was less than 10 [17].
The ambient PM2.5 and HDL levels were treated as continuous variables in this study. We stratified the baseline data by gender to examine whether there are potential disparities within the middle-aged and elderly populations. Multiple linear regression analysis was employed to explore the relationship between ambient PM2.5 and HDL levels. To mitigate the influence of potential confounding variables on the investigation’s outcomes, several covariates were adjusted. Participants were stratified into four age groups based on cutoffs of 50, 60, and 70. Model I was adjusted solely for age groups. Conversely, Model II incorporated adjustments for age, gender, education level, marital status, and residence. Furthermore, Model III included additional adjustments for smoking condition, drinking condition, and BMI. In the present study, Model IV encompassed further adjustments for various covariates, including hypertension, diabetes, lung diseases, heart diseases, stroke, psychological problems, arthritis, dyslipidemia, liver diseases, kidney diseases, digestive diseases, and asthma. To assess the heterogeneity of the association between ambient PM2.5 and HDL levels, interaction analyses were conducted, stratified by covariates. Subgroup analyses utilized stratified linear regression, and the p-value for interaction was determined through the log-likelihood ratio test, involving the comparison of models with and without covariate interactions. A significance level of 0.05 was deemed statistically significant for all the statistical findings in this study. The analyses were performed using R version 4.2.2.
留言 (0)